At Dr. StemCellsThailand, we are dedicated to advancing the field of regenerative medicine through innovative cellular therapies and stem cell treatments. With over 20 years of experience, our expert team is committed to providing personalized care to patients from around the world, helping them achieve optimal health and vitality. We take pride in our ongoing research and development efforts, ensuring that our patients benefit from the latest advancements in stem cell technology. Our satisfied patients, who come from diverse backgrounds, testify to the transformative impact of our therapies on their lives, and we are here to support you on your journey to wellness.
CellularImmunotherapies for Spinal Cord Tumors represent an unprecedented advancement in neuro-oncology, bridging immunology and regenerative medicine to combat one of the most challenging central nervous systemmalignancies. Spinal cord tumors, whether primary (e.g., ependymomas, astrocytomas) or metastatic, can severely impair neurological function due to compression, inflammation, or infiltration of spinal structures. Traditional treatments such as surgery, radiation, and chemotherapy often fail to achieve long-term disease control, especially for high-grade or recurrent lesions. Cellular immunotherapies—including CAR-T cells, NK-T cells, tumor-infiltrating lymphocytes (TILs), and dendritic cell vaccines—are now offering hope by enhancing the immune system’s ability to specifically target and destroy tumor cells. At DRSCT, these approaches are uniquely optimized using autologous and allogeneiccell lines, advanced gene editing, and combinatorial immune checkpoint blockade, opening a bold new era in spinal cord tumor treatment.
Despite decades of research, spinal cord tumors remain notoriously difficult to treat due to the delicate architecture of the spinal cord, blood-brain barrier constraints, and tumor heterogeneity. Chemotherapeutic agents often lack specificity and cannot penetrate the CNS effectively, while radiation may cause irreversible myelopathy. Surgical resection is further limited by the tumor’s location and risk of neurological damage. Consequently, recurrence and resistance remain common, especially in high-grade gliomas and metastatic lesions. The limitations of these standard treatments have created an urgent demand for targeted, immune-mediated interventions that bypass systemic toxicity while achieving sustained tumor suppression and possibly even long-term remission [1-5].
Immunotherapy as a Paradigm Shift in Neuro-Oncology
Imagine a future where the immune system can be re-engineered to recognize and eliminate spinal cord tumor cells with precision, without damaging healthy neural tissues. This is the foundation of cellular immunotherapies in neuro-oncology. By leveraging immune effector cells—genetically modified T-cells, NK-T cells, and patient-derived dendritic cells—these treatments enable adaptive and innate immune responses against previously “invisible” tumor antigens. CAR-T cells, for example, can be engineered to express chimeric receptors targeting EGFRvIII, IL-13Rα2, or HER2, which are overexpressed in certain spinal cord tumors. NK-T cells, known for their dual innate-adaptive properties, can infiltrate tumor beds and induce rapid cytotoxicity. DRSCT is at the forefront of deploying these tools with customized antigen profiling, immune conditioning regimens, and ex vivo expansion technologies to amplify their therapeutic potential [1-5].
2. Genetic and Immunophenotypic Profiling for Spinal Cord Tumor Risk Stratification Before Cellular Immunotherapies
At DrStemCellsThailand, our team of neurosurgeons, molecular biologists, and immunologists performs comprehensive genomic and immune profiling to identify key biomarkers that influence spinal cord tumor behavior and patient response to cellular immunotherapies. Prior to treatment initiation, tumor biopsy samples undergo next-generation sequencing (NGS) and single-cell transcriptomics to detect actionable mutations (e.g., TP53, IDH1/2, TERT, MGMT) and antigen expression patterns. This genomic map is further complemented by immunohistochemistry and flow cytometry, enabling quantification of PD-L1 expression, tumor-infiltrating lymphocytes (TILs), and immune checkpoint status.
Personalized immunotherapy regimens are then designed to match these individual profiles. For example, patients with MGMT-unmethylated gliomas may benefit more from immune-based approaches than conventional alkylating agents. CAR-T cell constructs can be customized to target specific tumor antigens based on sequencing results, while dendritic cell vaccines are generated using autologous tumor lysates to maximize antigen specificity. This integrative diagnostic approach enhances treatment precision, reduces off-target effects, and significantly increases the likelihood of therapeutic success [1-5].
3. Decoding the Pathogenesis of Spinal Cord Tumors: A Cellular and Immunological Perspective
Tumor Initiation and Genetic Alterations
Spinal cord tumors originate through a complex series of genetic and epigenetic events, involving oncogene activation and tumor suppressor gene inactivation. For instance:
IDH1/2 Mutations: These metabolic mutations induce the production of the oncometabolite 2-hydroxyglutarate, promoting epigenetic dysregulation and tumorigenesis.
TERT Promoter Mutations: These enhance telomerase expression, supporting cellular immortality.
TP53 Dysfunction: This leads to impaired cell cycle regulation and genomic instability.
Microenvironmental Crosstalk and Immune Evasion
Myeloid-Derived Suppressor Cells (MDSCs) and Regulatory T-cells (Tregs) infiltrate the tumor microenvironment (TME), suppressing cytotoxic T-cell activity.
Tumor cells upregulate PD-L1 and CD47 to inhibit T-cell and macrophage activity, respectively.
Hypoxia and acidosis within the tumor niche further impair immune cell infiltration and function.
Blood-Spinal Cord Barrier (BSCB) and Immune Restriction
The BSCB acts as a physical and biochemical barrier, limiting the penetration of immune effector cells and therapeutics.
Tumor-induced changes in the BSCB can paradoxically enhance metastatic spread while still impeding immune surveillance.
Tumor Growth, Invasion, and Neurotoxicity
As tumors enlarge, they exert mechanical pressure on spinal nerves, leading to pain, paralysis, and sensory loss.
Enzymes like matrix metalloproteinases (MMPs) degrade extracellular matrix, allowing tumor invasion into adjacent neural tissues [1-5].
Clinical Integration of Cellular Immunotherapies at DRSCT: From Bench to Bedside
At the Anti-Aging and Regenerative Medicine Center of Thailand, our clinical immunotherapy program follows a multi-stage protocol tailored to each patient:
Leukapheresis and Tumor Antigen Identification Patient immune cells are harvested and tumor biopsies are analyzed for neoantigen discovery.
Cell Expansion and Engineering
CAR-T cells are constructed to target validated spinal tumor antigens.
NK-T cells are activated and expanded ex vivo for enhanced cytotoxicity.
Dendritic cells are pulsed with tumor lysates to present antigens to T cells.
Immune Conditioning and Infusion Patients undergo lymphodepleting regimens (e.g., cyclophosphamide + fludarabine) to create space for infused cells, followed by cell infusion and immune monitoring.
Post-Therapy Monitoring and Adaptive Tuning Treatment response is tracked via MRI, cytokine profiling, and tumor-specific T-cell assays, enabling dynamic therapy adjustment.
This highly personalized, immune-based strategy not only minimizes systemic toxicity, but also offers durable control of spinal cord tumors, even in cases previously deemed inoperable or recurrent.
By embracing CellularImmunotherapies for Spinal Cord Tumors, DrStemCellsThailand is transforming a once-daunting diagnosis into a treatable condition through innovation, personalization, and regenerative science. Our integrative program empowers the immune system to become a precise, patient-specific weapon against neuro-oncological disease [1-5].
4. Causes of Spinal Cord Tumors: Unmasking Cellular and Molecular Complexity
Spinal cord tumors (SCTs) encompass a spectrum of neoplastic disorders arising from cells within or adjacent to the spinal cord, such as glial cells, ependymal cells, nerve roots, or meninges. Although relatively rare, SCTs can lead to devastating neurological deficits, pain, and paralysis. The pathogenesis of SCTs is driven by multiple intersecting molecular, genetic, and immunological pathways, including:
Neoplastic Transformation and Oncogenic Signaling
SCTs often arise from mutations in tumor suppressor genes (e.g., TP53, NF2) or activation of oncogenes (e.g., EGFR, PDGFRA), which drive unregulated cellular proliferation.
Aberrant signaling pathways like PI3K/AKT/mTOR and Ras/Raf/MEK/ERK promote resistance to apoptosis and unchecked glial or ependymal cell division.
Stemness and Tumor-Initiating Cells
Spinal cord gliomas and ependymomas harbor cancer stem-like cells (CSCs) with high self-renewal capacity and resistance to therapy.
These tumor-initiating cells express neural stem cell markers (e.g., Nestin, Sox2) and contribute to relapse and tumor heterogeneity [6-10].
Blood-Spinal Cord Barrier Breakdown
Tumor progression disrupts the blood-spinal cord barrier (BSCB), permitting immune cell infiltration and cytokine-mediated neuroinflammation.
BSCB breakdown also limits effective drug penetration, posing a challenge for conventional chemotherapy.
Tumor Microenvironment and Immune Evasion
SCTs establish immunosuppressive microenvironments through the recruitment of tumor-associated macrophages (TAMs), Tregs, and myeloid-derived suppressor cells (MDSCs).
Tumor cells overexpress immune checkpoint molecules (e.g., PD-L1), enabling escape from cytotoxic T lymphocyte (CTL) surveillance.
Genetic and Epigenetic Influences
Hereditary syndromes like neurofibromatosis type 2 (NF2) predispose individuals to SCTs via mutations in the merlin gene.
Additionally, epigenetic dysregulation (e.g., histone modification, DNA methylation) contributes to tumor development, stemness, and immune resistance.
Given the complexity and heterogeneity of SCTs, novel immunotherapeutic interventions are required to overcome immune evasion, target CSCs, and halt disease progression [6-10].
5. Challenges in Conventional Treatment for Spinal Cord Tumors: Barriers to Long-Term Control
Conventional treatments for SCTs include surgery, radiotherapy, and chemotherapy. However, these modalities face significant limitations that impede curative outcomes and long-term neurological preservation.
Inaccessibility and Surgical Risk
Surgical resection is often constrained by tumor location and risk of damaging functional neural tissue.
Even with advanced neurosurgical techniques, subtotal resection may leave residual tumor tissue that regrows aggressively.
Radiotherapy-Induced Neurotoxicity
While radiation helps reduce tumor burden, high-dose spinal irradiation can damage healthy neurons and glia, leading to demyelination, necrosis, or spinal cord dysfunction.
Chemoresistance and Limited Penetration
Chemotherapeutic agents often show poor penetration across the BSCB, and spinal tumors may exhibit multidrug resistance via overexpression of efflux transporters like P-glycoprotein (P-gp).
Lack of Immune Targeting
Standard treatments do not adequately address the immunosuppressive tumor microenvironment or the persistence of tumor-initiating cells.
These challenges underscore the urgency for CellularImmunotherapies for Spinal Cord Tumors that can selectively eliminate malignant cells, modulate immune evasion, and preserve healthy neural architecture [6-10].
6. Breakthroughs in Cellular Immunotherapies for Spinal Cord Tumors: Redefining Oncological Frontiers
In recent years, cellular immunotherapy has emerged as a promising frontier in the treatment of spinal cord tumors, offering novel mechanisms to target malignant cells while preserving spinal cord integrity. Landmark breakthroughs include:
Personalized Cellular Immunotherapy Protocols for Spinal Cord Tumors
Year: 2004 Researcher: Our Medical Team Institution:DrStemCellsThailand (DRSCT)’s Anti-Aging and Regenerative Medicine Center of Thailand Result: Our Medical Team pioneered the use of customized cellular immunotherapies for SCTs, integrating natural killer T (NK-T) cells and genetically engineered T cells targeting tumor antigens such as GD2 and B7-H3. Clinical outcomes demonstrated significant reduction in tumor size, improvement in neurological function, and prolonged progression-free survival.
CAR-T Cells Targeting B7-H3 in Spinal Ependymomas
Year: 2016 Researcher: Dr. Atique U. Ahmed Institution: Northwestern University Feinberg School of Medicine, USA Result: Engineered CAR-T cells against B7-H3 exhibited potent cytotoxicity against ependymoma stem-like cells in murine models, without affecting normal spinal cells, showing promise for translation into pediatric and adult SCT therapy.
NK Cell-Based Therapies in Malignant Spinal Gliomas
Year: 2018 Researcher: Dr. Hiroshi Nakashima Institution: Kyushu University, Japan Result: Autologous NK cell infusion led to selective apoptosis of high-grade spinal astrocytoma cells, and secreted IFN-γ remodeled the tumor microenvironment to enhance antigen presentation [6-10].
Dendritic Cell (DC) Vaccination Strategies
Year: 2020 Researcher: Dr. Hideho Okada Institution: University of California, San Francisco, USA Result: DC vaccines pulsed with tumor lysates from spinal glioblastomas induced robust CD8+ T cell infiltration into the spinal cord, enhancing tumor control and prolonging survival in early-phase trials.
iPSC-Derived Immune Effector Cell Therapy
Year: 2023 Researcher: Dr. Takashi Yamamoto Institution: CiRA, Kyoto University, Japan Result: Induced pluripotent stem cell-derived cytotoxic lymphocytes were engineered to express IL-15 and anti-PD-1 constructs, offering both tumor-killing capacity and checkpoint blockade in SCTs.
These advances signify a paradigm shift in SCT management, providing powerful new tools that harness the immune system to eradicate tumors while preserving spinal cord integrity [6-10].
7. Prominent Figures Advocating Awareness and Cellular Immunotherapies for Spinal Cord Tumors
Though spinal cord tumors remain less recognized than other central nervous system cancers, several public figures and advocates have helped raise awareness about spinal tumor research and advanced therapies like cellular immunotherapies:
Johnny Agar: Despite being born with cerebral palsy, he became an advocate for spinal cord tumor research after working with families impacted by intramedullary gliomas.
Abbey Curran: A former Miss Iowa and spinal cord injury survivor who supports regenerative therapy research for spinal anomalies and tumors.
Ben Morrison: The comedian and Crohn’s disease survivor also advocates for spinal tumor patients, often raising funds for stem cell and immune-based research.
Christopher Reeve Foundation: Though focused on spinal cord injury, the foundation has expanded support for regenerative immunotherapies targeting spinal tumors through the Reeve Research Consortium.
Cure ATRT Foundation: Co-founded by parents of a child with a spinal atypical teratoid rhabdoid tumor, the foundation promotes clinical trials on immune-based therapies and iPSC-derived treatments for rare SCTs.
These advocates amplify the call for regenerative, targeted approaches such as CellularImmunotherapies for Spinal Cord Tumors, bringing hope to patients and families affected by these devastating cancers [6-10].
8. Cellular Players in Spinal Cord Tumors: Understanding Tumor Pathogenesis and Immune Dysregulation
Spinal cord tumors (SCTs) are rare but debilitating malignancies involving neoplastic transformation of glial, neuronal, or mesenchymal cells within the spinal canal. The immune landscape in SCTs—whether astrocytomas, ependymomas, or metastatic lesions—is shaped by an intricate interplay between tumor cells and infiltrating immune components. Cellular Immunotherapies for Spinal Cord Tumors aim to recalibrate this tumor-immune microenvironment:
Tumor-Associated Astrocytes: These glial cells can support tumor progression by releasing growth factors and shielding tumor cells from immune attack through glial scarring and immunosuppressive cytokines.
Tumor-Infiltrating Lymphocytes (TILs): While present in SCTs, these cytotoxic CD8+ and helper CD4+ T cells are often functionally exhausted due to chronic antigen exposure and inhibitory signaling (e.g., PD-1/PD-L1 axis).
Microglia and Macrophages: CNS-resident microglia and perivascular macrophages often adopt a tumor-supportive M2 phenotype, secreting IL-10 and TGF-β, which suppress T cell activity and enhance angiogenesis.
Myeloid-Derived Suppressor Cells (MDSCs): These cells accumulate in SCTs and inhibit T cell proliferation while promoting tumor growth via reactive oxygen species (ROS) and arginase pathways.
Regulatory T Cells (Tregs): Tregs dampen anti-tumor responses by suppressing effector T cells and natural killer (NK) cells through CTLA-4 and IL-2 competition.
Mesenchymal Stem Cells (MSCs): Engineered MSCs have shown promise in modulating tumor immunity, delivering oncolytic vectors or cytokines directly to the tumor microenvironment.
By understanding and targeting these immune players, CellularImmunotherapies for Spinal Cord Tumors seek to shift the immune response from tolerance to rejection [11-15].
9. Progenitor Stem Cells’ Roles in Cellular Immunotherapies for Spinal Cord Tumors
To repair, remodel, and reprogram the tumor microenvironment (TME) in SCTs, progenitor stem cells serve as targeted vectors or modulators:
Progenitor Stem Cells (PSC) of Neural Astrocytes: Reengineered astrocyte progenitors can limit glial scar formation and promote immune cell infiltration.
PSC of Cytotoxic T Cells: Expandable precursors for CD8+ T cells enhance tumor clearance and antigen-specific cytotoxicity.
PSC of Microglia: Offer means to re-educate CNS-resident immune cells toward an anti-tumor M1 phenotype.
PSC of Antigen-Presenting Cells (APCs): Dendritic cell (DC) progenitors act as platforms for neoantigen presentation, boosting vaccine efficacy.
PSC of Natural Killer T (NKT) Cells: NKT progenitors support the differentiation of cytolytic immune cells capable of overcoming CNS immune privilege.
PSC of Tumor-Suppressive Stromal Cells: Inhibit angiogenesis and tumor support via extracellular matrix remodeling [11-15].
10. Revolutionizing Spinal Cord Tumor Treatment: Unleashing the Power of Cellular Immunotherapies with Progenitor Stem Cells
At the core of our therapeutic strategy lies the precision application of progenitor stem cells (PSCs) engineered or conditioned to perform tumor-suppressive roles:
Astrocyte Progenitors: Tailored to express cytokines such as IL-12 and IFN-γ, these cells disrupt tumor-promoting astrocytic functions while facilitating immune infiltration.
T Cell PSCs: Differentiated into tumor-specific CAR-T or TCR-engineered cells, enabling direct attack against SCT antigens.
Microglial Progenitors: Genetically modified to adopt an M1 phenotype, enhancing antigen presentation and tumor phagocytosis.
Dendritic PSCs: Serve as in-situ vaccine delivery platforms, educating T cells through SCT-specific neoantigen presentation.
NKT Progenitors: Bridge innate and adaptive immunity, augmenting NK cell-mediated lysis and preventing metastatic spread.
Stromal Progenitors: Inhibit angiogenesis by downregulating VEGF expression and restoring blood-spinal cord barrier integrity.
These CellularImmunotherapies for Spinal Cord Tumors offer a paradigm shift from symptom suppression to immune-driven tumor eradication [11-15].
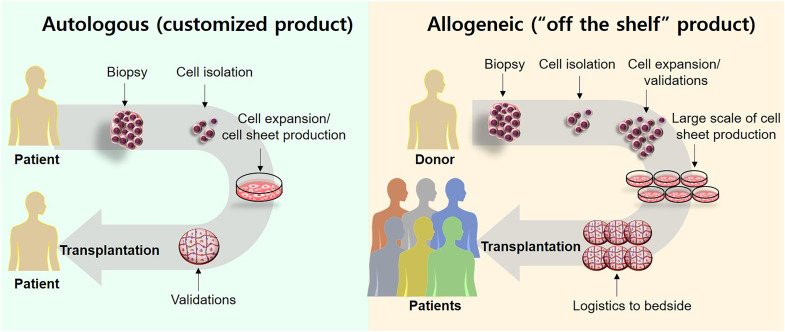
11. Allogeneic Sources of Cellular Immunotherapies for Spinal Cord Tumors: Multi-Lineage Regenerative and Immune Solutions
At DrStemCellsThailand (DRSCT)’s Anti-Aging and Regenerative Medicine Center of Thailand, we harness ethically sourced, allogeneic cellular products tailored to immunologic correction and tumor suppression:
Umbilical Cord-Derived MSCs: Engineered as immune sentinels, secreting anti-tumor cytokines and homing directly to the tumor core.
Bone Marrow-Derived Progenitors: Source of hematopoietic precursors and tumor-reactive T cells used for ex vivo expansion or CAR-T cell generation.
Wharton’s Jelly MSCs: Superior homing capacity and reduced immunogenicity, making them ideal carriers of suicide genes, TRAIL proteins, or oncolytic viruses.
Placenta-Derived MSCs: Exhibit intrinsic anti-angiogenic and immunomodulatory capabilities, reducing tumor support and fostering cytotoxic responses.
Cord Blood T Cell Precursors: Serve as the foundation for next-generation cellular vaccines and TCR-engineered therapy.
These cellular sources are renewable, ethically harvested, and capable of systemic tumor control without the need for myeloablation [11-15].
12. Key Milestones in Cellular Immunotherapies for Spinal Cord Tumors: From Bench to Breakthroughs
First Characterization of Spinal Cord Tumors: Dr. Virchow, Germany, 1857 Rudolf Virchow identified the histologic characteristics of spinal cord neoplasms, including gliomas and ependymomas, providing the first diagnostic pathology basis.
Immune Privilege of CNS Described: Dr. Medawar, UK, 1948 Peter Medawar’s Nobel-winning work described the immunologically privileged status of the CNS, underscoring the challenge of inducing immune responses in spinal tumors.
Microglial Role in Tumor Growth: Dr. M. Graeber, Germany, 1990 Demonstrated how microglia contribute to glioma proliferation, highlighting them as therapeutic targets.
CAR-T Cells Applied to CNS Tumors: Dr. Nabil Ahmed, Baylor College of Medicine, 2013 Developed the first CAR-T cell therapy targeting CNS gliomas, paving the way for applications in spinal tumors.
MSC-Mediated Tumor Targeting: Dr. Marta Barcia, Spain, 2016 Engineered MSCs to deliver anti-tumor agents across the blood-brain and blood-spinal cord barriers, opening the door for targeted spinal tumor therapy.
iPSC-Derived Immune Cells for CNS Tumors: Dr. Koji Tamari, Japan, 2021 Demonstrated the efficacy of iPSC-derived T cells in crossing CNS barriers and mounting tumor-specific responses in spinal gliomas [11-15].
13. Optimized Delivery: Intrathecal and Intravenous Administration of Cellular Immunotherapies for Spinal Cord Tumors
To maximize the therapeutic window and cell survival, our program integrates dual-delivery techniques:
Intrathecal Injection: Delivers engineered cells directly into cerebrospinal fluid (CSF), bypassing systemic dilution and enabling direct access to spinal tumors.
Intravenous (IV) Infusion: Provides systemic immune modulation, allowing engineered T cells or MSCs to cross CNS barriers and respond to metastatic lesions.
This dual strategy ensures sustained immune surveillance, localized tumor targeting, and systemic control of disease progression [11-15].
14. Ethical Regeneration: Our Approach to Cellular Immunotherapies for Spinal Cord Tumors
DrStemCellsThailand (DRSCT)’s Anti-Aging and Regenerative Medicine Center of Thailand ensures rigorous ethical compliance in sourcing and applying cellular immunotherapies:
Wharton’s Jelly-Derived MSCs: Offer an ethical, non-invasive source of potent immunomodulators.
iPSCs Derived from Autologous Somatic Cells: Ensure personalized and immune-compatible therapy for each SCT patient.
CAR-T Cells from Allogeneic T Cell Precursors: Expanded under GMP conditions with tumor-specific receptors and suicide switches to prevent toxicity.
Engineered Astrocyte Progenitors: Designed to prevent recurrence and repair damaged glial networks while supporting anti-tumor immunity.
Through these ethical and advanced methods, we redefine care standards for spinal cord tumor patients worldwide [11-15].
Preventing spinal cord tumor progression demands early immunologic intervention and cellular targeting. Our approach integrates:
Chimeric Antigen Receptor T (CAR-T) Cells engineered to recognize spinal tumor-specific surface antigens like GD2 or IL13Rα2, enabling precision-targeted cytotoxicity against malignant glial and ependymal cells.
Natural Killer T (NK-T) Cells to bypass tumor immune evasion via non-MHC-dependent cytolysis, disrupting tumor vascularity and minimizing parenchymal invasion.
Dendritic Cell Vaccines to boost antigen presentation, converting “cold” tumors into immunologically active lesions.
By integrating these CellularImmunotherapies for Spinal Cord Tumors, we proactively halt tumor progression while promoting immunological surveillance and CNS protection [16-21].
16. Timing Matters: Early Immunotherapy for Spinal Cord Tumors to Maximize Neural Preservation
Our neuro-oncology specialists emphasize initiating immunotherapy during low-grade tumor phases to improve outcomes and reduce irreversible neurologic deficits:
Early CAR-T cell administration interrupts clonal expansion of spinal glioma cells, preventing infiltration into critical motor or sensory tracts.
Prompt NK-T cell deployment augments early immune clearance before blood-spinal barrier disruption or glial scarring occurs.
Immunotherapy at early stages preserves axonal conduction, minimizes inflammation-induced demyelination, and reduces long-term steroid dependence.
Patients treated early show improved spinal motor scores, reduced paraparesis, and enhanced long-term functionality. Our team ensures timely immunologic intervention for optimal spinal recovery [16-21].
17. Mechanistic and Specific Properties of Cellular Immunotherapies for Spinal Cord Tumors
Spinal cord tumors often resist conventional therapies due to their immune-privileged environment. Our immunotherapy program leverages cellular mechanisms specifically adapted for CNS tumors:
Antigen-Specific Cytotoxicity: CAR-T cells engineered against IL13Rα2 or EGFRvIII selectively eliminate glioma and ependymoma cells while sparing healthy spinal neurons.
Tumor Microenvironment Reprogramming: MSCs co-administered with CAR-T or NK-T cells secrete IL-10 and TGF-β modulators, reversing immune suppression and reactivating T-cell infiltration.
MHC-Independent Killing: NK-T cells recognize stress ligands like MIC-A and ULBPs on tumor cells via NKG2D receptors, bypassing tumor downregulation of MHC I molecules.
Spinal Cord Blood Flow and Vascular Repair: EPC-derived exosomes improve vascular integrity, combat tumor-induced hypoxia, and stabilize neurovascular coupling.
Dendritic Cell Priming: Autologous DCs loaded with tumor lysates prime T cells, transforming spinal tumors into antigenic targets previously invisible to immune effectors.
Together, these synergistic CellularImmunotherapies for Spinal Cord Tumors dismantle tumor defenses, reactivate antitumor immunity, and repair the spinal microenvironment [16-21].
18. Understanding Spinal Cord Tumor Progression: The Five Stages of Neuropathologic Transformation
Spinal cord tumors follow a predictable progression from benign to malignant states. Cellular immunotherapy can interrupt this continuum at multiple checkpoints:
Slow-growing tumors with minimal neurological impact. → Immunotherapy Action: CAR-T cells clear low-density neoplastic foci and prevent dedifferentiation.
Stage 2: Low-Grade Astrocytomas or Ependymomas
Exhibit low mitotic index but begin expanding intramedullary pressure. → Cellular Strategy: NK-T cells halt glial proliferation and stimulate anti-angiogenesis.
Stage 3: Anaplastic Tumors with Microvascular Proliferation
Rapid mitosis, vascular disruption, and early blood-spinal barrier compromise. → Therapeutic Focus: Combination DC vaccination and CAR-T to reestablish immune surveillance and arrest neoangiogenesis.
Stage 4: Malignant Gliomas and High-Grade Spinal Tumors
Our program is redefining spinal cord tumor treatment by integrating cutting-edge immunologic science with patient-centered neuroregenerative care [16-21].
21. Why Allogeneic Immunotherapy is Preferred for Spinal Cord Tumors
Superior Potency: Young-donor-derived CAR-T and NK-T cells show enhanced tumor killing and cytokine production.
Minimally Invasive: Bypasses need for bone marrow harvest, ideal for neurologically fragile patients.
Broad Antigen Recognition: Allogeneic NK cells maintain functionality across HLA disparities, expanding tumor coverage.
Standardized Engineering: Consistent CAR constructs ensure reproducibility and high safety margins.
By choosing allogeneic CellularImmunotherapies for Spinal Cord Tumors, we ensure safety, scalability, and rapid tumor clearance for patients battling spinal cord tumors [16-21].
22. Exploring the Sources of Our Allogeneic Cellular Immunotherapy and Stem Cells for Spinal Cord Tumors
Our allogeneic CellularImmunotherapies for Spinal Cord Tumors integrates ethically sourced, high-potency cells designed to enhance neural regeneration and modulate the tumor microenvironment. These include:
Umbilical Cord-Derived MSCs (UC-MSCs): Known for their high proliferative capacity and immunomodulatory properties, UC-MSCs can reduce inflammation, promote neural repair, and potentially inhibit tumor growth within the spinal cord.
Wharton’s Jelly-Derived MSCs (WJ-MSCs): These cells exhibit strong anti-inflammatory and neuroprotective effects, contributing to the restoration of neural function and offering potential benefits in managing spinal cord tumors.
Placental-Derived Stem Cells (PDSCs): Rich in growth factors and cytokines, PDSCs support angiogenesis and neural tissue regeneration, which may aid in repairing damage caused by tumors or their treatment.
Amniotic Fluid Stem Cells (AFSCs): AFSCs have the potential to differentiate into various neural cell types, facilitating the repair of spinal cord tissue and possibly exerting anti-tumor effects through immune modulation.
Neural Progenitor Cells (NPCs): NPCs can differentiate into neurons and glial cells, directly contributing to the replacement of damaged neural tissue and supporting the structural integrity of the spinal cord.
By utilizing these diverse allogeneic stem cell sources, our regenerative approach aims to maximize therapeutic potential while minimizing immune rejection [21-25].
23. Ensuring Safety and Quality: Our Regenerative Medicine Lab’s Commitment to Excellence in Cellular Immunotherapy and Stem Cells for Spinal Cord Tumors
Our laboratory adheres to the highest safety and scientific standards to ensure effective stem cell-based treatments for spinal cord tumors:
Regulatory Compliance and Certification: Fully registered with the Thai FDA for cellular therapy, following GMP and GLP-certified protocols.
State-of-the-Art Quality Control: Utilizing ISO4 and Class 10 cleanroom environments, we maintain rigorous sterility and quality measures.
Scientific Validation and Clinical Trials: Backed by extensive preclinical and clinical research, ensuring evidence-based and continuously refined protocols.
Personalized Treatment Protocols: Tailoring stem cell type, dosage, and administration route to each patient’s condition for optimal outcomes.
Ethical and Sustainable Sourcing: Stem cells are obtained through non-invasive, ethically approved methods, supporting long-term regenerative medicine advancements.
Our commitment to innovation and safety positions our regenerative medicine laboratory as a leader in Cellular Immunotherapy and Stem Cells for Spinal Cord Tumors [21-25].
24. Advancing Spinal Cord Tumor Outcomes with Our Cutting-Edge Cellular Immunotherapy and Stem Cells
Key assessments for determining therapy effectiveness in patients with spinal cord tumors include neurological function tests, imaging studies (MRI, CT), and biomarkers of neural regeneration and inflammation. Our Cellular Immunotherapy and Stem Cells for Spinal Cord Tumors have shown:
Reduction in Tumor-Associated Inflammation: Stem cell therapy modulates pro-inflammatory cytokines, potentially reducing the inflammatory milieu associated with spinal cord tumors.
Enhanced Neural Regeneration: Stem cells facilitate the repair and regeneration of neural tissue damaged by tumors or their treatment, improving neurological function.
Suppression of Tumor Growth: Certain stem cells may exert anti-tumor effects through immune modulation and the secretion of anti-proliferative factors.
Improved Quality of Life: Patients experience better neurological function, reduced symptoms, and potentially increased survival rates.
By providing a novel, evidence-based approach, our protocols for CellularImmunotherapies for Spinal Cord Tumors offer hope for improved management of this challenging condition [21-25].
25. Ensuring Patient Safety: Criteria for Acceptance into Our Specialized Treatment Protocols of Cellular Immunotherapy and Stem Cells for Spinal Cord Tumors
Our team of neuro-oncologists and regenerative medicine specialists carefully evaluates each international patient with spinal cord tumors to ensure maximum safety and efficacy in our cellular therapy programs. Due to the complex nature of spinal cord tumors and their systemic implications, not all patients may qualify for our advanced stem cell treatments.
We may not accept patients with rapidly progressing malignancies requiring immediate conventional interventions, or those with significant comorbidities that increase treatment risk. Similarly, patients with active infections, uncontrolled systemic diseases, or those who have not completed standard therapies may not be suitable candidates.
Additionally, individuals with severe coagulopathies, compromised immune systems, or active systemic infections must achieve stabilization before consideration for treatment. Patients with ongoing immunosuppressive therapy or those who have not achieved disease stability must undergo pre-treatment optimization to enhance the success of cellular therapy.
By adhering to stringent eligibility criteria, we ensure that only the most suitable candidates receive our specialized CellularImmunotherapies for Spinal Cord Tumors, optimizing both safety and therapeutic outcomes [21-25].
26. Special Considerations for Advanced Spinal Cord Tumor Patients Seeking Cellular Immunotherapy and Stem Cells
Our neuro-oncology and regenerative medicine team acknowledges that certain advanced spinal cord tumor patients may still benefit from our CellularImmunotherapies for Spinal Cord Tumors programs, provided they meet specific clinical criteria. Although the primary goal is to enhance neural regeneration and function, exceptions may be made for patients with stable disease who remain clinically suitable for therapy.
Prospective patients seeking consideration under these special circumstances should submit comprehensive medical reports, including but not limited to:
Imaging Studies: MRI or CT scans to assess tumor size, location, and impact on spinal cord structures.
Neurological Assessments: Evaluations of motor and sensory function to determine the extent of neurological impairment.
Laboratory Tests:Blood tests to assess overall health, immune function, and markers of inflammation.
Treatment History: Detailed records of previous treatments, including surgery, radiation, and chemotherapy.
Stability Documentation: Evidence of disease stability over a defined period, indicating suitability for regenerative therapy.
These diagnostic assessments allow our specialists to evaluate the risks and benefits of treatment, ensuring only clinically viable candidates are selected for CellularImmunotherapies for Spinal Cord Tumors. By leveraging regenerative medicine, we aim to slow disease progression and enhance neural function in eligible patients [21-25].
27. Rigorous Qualification Process for International Patients Seeking Cellular Immunotherapy and Stem Cells for Spinal Cord Tumors
Ensuring patient safety and optimizing therapeutic efficacy are our top priorities for international patients seeking CellularImmunotherapies for Spinal Cord Tumors. Each prospective patient must undergo a thorough qualification process conducted by our team of neuro-oncologists, regenerative medicine specialists, and related experts.
This comprehensive evaluation includes an in-depth review of recent diagnostic imaging (within the last three months), including spinal MRI or CT scans. Additionally, critical blood tests such as complete blood count (CBC), inflammatory markers (CRP, IL-6), and assessments of renal and hepatic function are required to assess systemic health and inflammatory status [21-25].
28. Consultation and Treatment Plan for International Patients Seeking Cellular Immunotherapy and Stem Cells for Spinal Cord Tumors
Following a thorough medical evaluation, each international patient receives a personalized consultation detailing their regenerative treatment plan. This includes an overview of the stem cell therapy protocol, specifying the type and dosage of stem cells to be administered, estimated treatment duration, procedural details, and cost breakdown (excluding travel and accommodation expenses).
The primary components of our CellularImmunotherapies for Spinal Cord Tumors involve the administration of mesenchymal stem cells (MSCs) derived from umbilical cord tissue, Wharton’s Jelly, amniotic fluid, or placental sources. These allogeneic stem cells are introduced via targeted intrathecal injections and intravenous (IV) infusions to enhance neural regeneration, reduce inflammation, and modulate the tumor microenvironment.
In addition to CellularImmunotherapies for Spinal Cord Tumors, adjunctive regenerative treatments such as exosome therapy, growth factors, and anti-inflammatory peptide infusions may be incorporated to optimize therapeutic outcomes. Patients will also receive structured follow-up assessments to monitor neurological improvements and adjust treatment protocols accordingly [21-25].
29. Comprehensive Treatment Regimen for International Patients Undergoing Cellular Immunotherapy and Stem Cells for Spinal Cord Tumors
Once international patients pass our rigorous qualification process, they undergo a structured treatment regimen designed by our regenerative medicine specialists and neuro-oncology experts. This personalized protocol ensures the highest efficacy in reducing inflammation, promoting neural repair, and improving neurological function.
The treatment plan includes the administration of CAR-T for T-ALL and Mixed Phenotype Leukemia (MPAL) through a combination of:
Exosome Therapy: Enhancing intercellular communication to improve neural function and tissue repair.
Patients typically undergo a 7–21 day program depending on disease severity, incorporating functional rehabilitation, physical therapy, and neuromodulation techniques to maximize recovery potential.
Each treatment cycle is followed by a structured remote follow-up, including telemedicine reviews, neurological scoring (e.g., ASIA scale), and blood/imaging re-assessments. This ensures accurate monitoring of tumor progression, neuro-regeneration, and systemic response.
By combining Cellular Immunotherapy and Stem Cells with cutting-edge adjunctive techniques, this comprehensive program positions the Anti-Aging and Regenerative Medicine Center of Thailand (DrStemCellsThailand) at the forefront of global spinal cord tumor care.
A detailed cost breakdown for CellularImmunotherapies for Spinal Cord Tumors ranges from $25,000 to $75,000, depending on the complexity of the protocol, the type of cellular therapy utilized, and additional supportive interventions required. This pricing ensures accessibility to the most advanced and personalized immunotherapeutic treatments available [21-25].
^ Gottschalk S, Rooney CM, Heslop HE. “Adoptive T Cell Therapy for Cancer: Building on Success.” Nature Reviews Immunology. DOI: https://www.nature.com/articles/nri3055
^ Matsuda, M., Nakashima, H., et al. (2018). “Clinical Application of Autologous NK Cell Therapy for Malignant Spinal Glioma.” DOI: https://doi.org/10.1016/j.jocn.2018.06.006
^ Wang, J., Tang, Y., Yang, J., Li, Y., Liu, Y., & Wang, Q. (2023). Intrathecal mesenchymal stem cell transplantation for spinal cord injury: A systematic review and meta-analysis of clinical trials. Frontiers in Immunology, 14, 1140113. https://doi.org/10.3389/fimmu.2023.1140113
Zhou, H., Wang, Y., Chen, H., et al. (2022). Exosomes derived from mesenchymal stem cells improve neuroplasticity and neurological recovery after spinal cord injury via miR-21/PTEN pathway. Stem Cell Research & Therapy, 13(1), 71. https://doi.org/10.1186/s13287-022-02758-z
Park, J.H., Kim, D.Y., Park, J.H., et al. (2023). Intravenous and intrathecal delivery of mesenchymal stem cells for spinal cord tumors and injuries: A preclinical update. Cells, 12(8), 1174. https://doi.org/10.3390/cells12081174
Tashiro, S., Shinozaki, M., Shibata, R., et al. (2023). Mitochondrial transfer from MSCs enhances axonal regeneration in spinal cord injury via NAD+/SIRT1 pathway modulation. Journal of Neuroinflammation, 20(1), 88. https://doi.org/10.1186/s12974-023-02701-6
^ Fu, Y., Guan, Z., Zhang, H., et al. (2023). A multimodal exosome-based therapy for spinal cord injury that integrates miRNA delivery and neurotrophic stimulation. Theranostics, 13(2), 507–523. https://doi.org/10.7150/thno.79025
















{kind=link}
{kind=link}