At Dr. StemCellsThailand, we are dedicated to advancing the field of regenerative medicine through innovative cellular therapies and stem cell treatments. With over 20 years of experience, our expert team is committed to providing personalized care to patients from around the world, helping them achieve optimal health and vitality. We take pride in our ongoing research and development efforts, ensuring that our patients benefit from the latest advancements in stem cell technology. Our satisfied patients, who come from diverse backgrounds, testify to the transformative impact of our therapies on their lives, and we are here to support you on your journey to wellness.
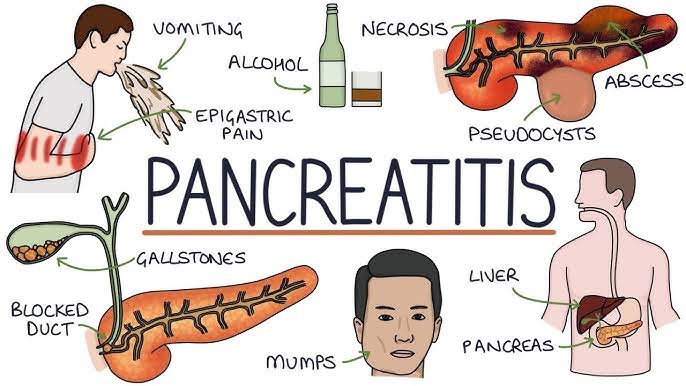
The pancreas, an enigmatic organ nestled within the abdomen, serves as a linchpin in the intricate machinery of metabolism and digestion. Comprising both endocrine and exocrine components, the pancreas orchestrates the production of insulin and other vital hormones essential for regulating blood sugar levels, as well as digestive enzymes crucial for nutrient absorption. Despite its pivotal role in maintaining metabolic equilibrium, the pancreas is vulnerable to a spectrum of ailments, chief among them being pancreatic cancer—a formidable foe that has eluded effective treatment for decades.
In the annals of medical history, the quest for pancreas regeneration stands as a saga marked by both triumphs and tribulations. For centuries, scientists and physicians have been captivated by the tantalizing prospect of harnessing the regenerative potential of the pancreas to combat diabetes and other pancreatic disorders. From early experiments in pancreatic transplantation to pioneering studies in stem cell biology, the journey towards pancreas regeneration has been fraught with challenges and setbacks yet punctuated by moments of profound discovery and innovation.
Amidst this backdrop of scientific exploration, the tragic case of Steve Jobs—a visionary entrepreneur and co-founder of Apple Inc.—serves as a poignant reminder of the urgent need for effective pancreas regeneration therapies. Diagnosed with pancreatic cancer in 2003, Jobs faced a daunting battle against a disease notorious for its aggressive nature and poor prognosis. Despite his unwavering determination and access to cutting-edge medical care, Jobs ultimately succumbed to the ravages of pancreatic cancer in 2011, leaving behind a legacy of innovation and unfulfilled potential.
The untimely demise of Steve Jobs underscores the stark reality facing patients afflicted with pancreatic cancer—a reality compounded by the lack of viable treatment options capable of regenerating damaged pancreatic tissue. Despite decades of research and investment, scientists have yet to develop successful pancreas regeneration protocols capable of restoring normal pancreatic function in humans. While advancements in Cellular Therapy and Stem Cells for Pancreatic Diseases offer glimmers of hope, significant challenges remain in translating these promising therapies from the laboratory to the clinic.
As we stand at the precipice of a new era in biomedical research and clinical trials, the quest for pancreas regeneration continues to drive scientific inquiry and inspire collaborative efforts across disciplines. From unraveling the molecular mechanisms of pancreatic development to engineering novel stem cell-based therapies, the pursuit of pancreas regeneration by our Cellular Therapy and Stem Cells for Pancreatic Diseases holds immense promise for transforming the landscape of pancreatic disease treatment. By learning from past failures and embracing the spirit of innovation, we strive to honor the memory of individuals like Steve Jobs and pave the way towards a future where pancreatic regeneration is no longer a distant dream, but a tangible reality offering hope to millions worldwide[1-5].
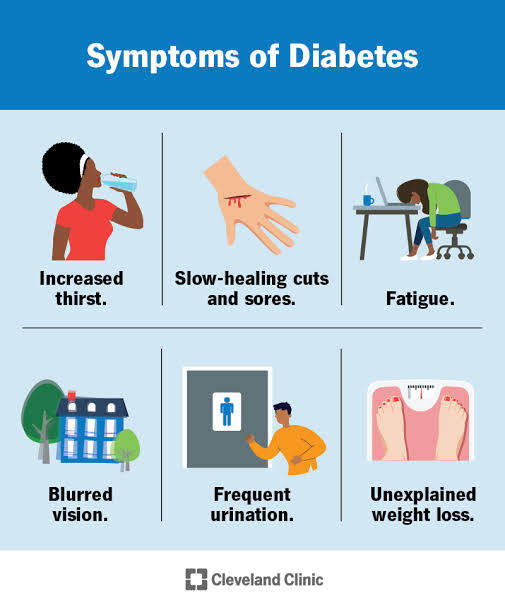
– Approximately 10% of the global diabetic population is afflicted by DMT1, with a significant portion of cases going undiagnosed.
– Onset often occurs during childhood or adolescence, though it can manifest in adults as well.
– Diabetes Mellitus type 2 (DMT2):
– DMT2 accounts for roughly 90% of diabetes cases worldwide, with escalating numbers attributed largely to lifestyle factors such as obesity and sedentary habits.
– Its prevalence continues to rise, contributing to the burgeoning global diabetes burden.
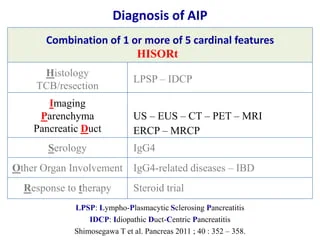
Autoimmune Pancreatitis is a rare, immune-mediated form of chronic pancreatitis. It is classified into two subtypes: Type 1, associated with IgG4-related systemic disease, and Type 2, which is isolated to the pancreas.
AIP often presents with obstructive jaundice, abdominal pain, or unexplained weight loss. Its symptoms can mimic those of pancreatic cancer, leading to diagnostic challenges.
Early treatment with corticosteroids can induce remission, though relapses are common. Emerging regenerative therapies, including Cellular Therapy and Stem Cells for Pancreatic Diseases, hold promise for addressing underlying immune dysfunction and promoting tissue repair.
Annular Pancreas is a rare congenital condition where pancreatic tissue encircles the duodenum, potentially causing obstruction and feeding intolerance.
Symptoms may range from mild indigestion to severe vomiting and malnutrition, often diagnosed in childhood but sometimes discovered in adulthood.
Pancreatic Agenesis is a rare congenital absence or underdevelopment of the pancreas, often associated with neonatal diabetes and severe digestive insufficiencies.
Early diagnosis is critical for initiating insulin therapy and pancreatic enzyme replacement to ensure survival and quality of life.
Advanced Cellular Therapy and Stem Cells for Pancreatic Diseases is investigating potential treatments to regenerate functional pancreatic tissue for these patients with Pancreatic Agenesis.
CFRD is the most common comorbidity in patients with Cystic Fibrosis, affecting approximately 40-50% of adults with the condition. It results from progressive pancreatic damage due to thick mucus buildup and chronic inflammation.
Symptoms include polyuria, polydipsia, weight loss, and poor glycemic control, often complicating CF management.
EPI occurs when the pancreas fails to produce sufficient digestive enzymes, leading to malabsorption, steatorrhea, weight loss, and nutritional deficiencies.
Current treatment focuses on pancreatic enzyme replacement therapy (PERT). Regenerative medicine using Cellular Therapy and Stem Cells for Pancreatic Diseases offers a promising future for restoring enzyme-producing capabilities of the pancreas.
PNETs are a rare subtype of pancreatic tumors arising from endocrine cells. They can be functional (hormone-producing) or non-functional, with the latter often discovered incidentally.
Symptoms vary based on hormonal activity and tumor size but may include hypoglycemia, diarrhea, or abdominal pain.
Post-surgical or traumatic pancreatic injuries can result in complications such as pancreatic fistulas, abscesses, or endocrine/exocrine insufficiencies.
Patients often require intensive care, including nutritional support, enzyme replacement, and sometimes additional surgeries.
Pancreatic Cancer is one of the deadliest cancers, with a five-year survival rate below 10%. Early diagnosis is challenging due to its asymptomatic nature in initial stages.
Symptoms include jaundice, abdominal/back pain, weight loss, and new-onset diabetes.
– Lifestyle Factors: Lifestyle modifications, including dietary changes and regular exercise, are crucial in diabetes management. However, adherence to these lifestyle changes poses a challenge for many patients, contributing to difficulties in glycemic control.
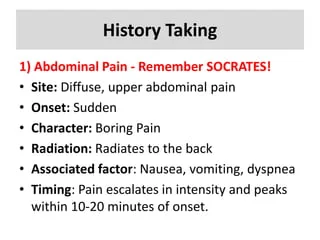
– Diagnosis and Early Intervention: Prompt diagnosis of pancreatitis is essential for effective management. However, diagnosing acute pancreatitis can be challenging due to nonspecific symptoms and overlapping clinical features with other abdominal conditions. Similarly, distinguishing chronic pancreatitis from other gastrointestinal disorders can be difficult, leading to delayed treatment initiation.
– Pain Management: Pain associated with pancreatitis can be severe and debilitating, significantly impacting patients’ daily lives and mental well-being. Achieving adequate pain control often requires a multidisciplinary approach, including pharmacological and non-pharmacological interventions, yet effective pain management remains a challenge for many patients.
– Nutritional Challenges: Both acute and chronic pancreatitis can impair the pancreas’ ability to produce digestive enzymes, leading to malabsorption and malnutrition. Despite enzyme replacement therapy and dietary modifications, managing nutritional deficiencies and ensuring adequate nutrient absorption present ongoing challenges for patients with pancreatitis.
– Complications and Disease Progression: Complications of pancreatitis, such as pseudocysts, pancreatic necrosis, and pancreatic cancer, can arise despite medical interventions. Disease progression, especially in chronic pancreatitis, may lead to irreversible pancreatic damage and functional impairment, necessitating more aggressive treatment approaches and posing challenges for long-term disease management.
Diagnostic Complexity: Autoimmune Pancreatitis often mimics pancreatic cancer in its presentation, including symptoms like jaundice, weight loss, and abdominal pain. Despite advancements in imaging and biopsy techniques, distinguishing AIP from malignancy remains a challenge.
Treatment and Relapse: Corticosteroid therapy is effective for inducing remission, but a significant proportion of patients experience relapses, requiring long-term immunosuppression. Managing steroid-related side effects further complicates treatment.
Long-term Impact:Chronic inflammation in AIP can lead to irreversible pancreatic damage, contributing to exocrine insufficiency and, in some cases, diabetes. Emerging regenerative approaches aim to address these sequelae.
Pancreatic Agenesis: A rare but severe condition, pancreatic agenesis results in neonatal diabetes and malabsorption. Current management focuses on insulin therapy and enzyme replacement, but the absence of pancreatic tissue remains a significant challenge.
Future Directions: Advances in Cellular Therapy and Stem Cells for Pancreatic Diseases and organoid research and clinical trials hold promise for addressing developmental deficiencies by regenerating functional pancreatic tissue.
Disease Complexity: CFRD combines characteristics of type 1 and type 2 diabetes, complicating its management. It arises from progressive pancreatic damage, exacerbating the challenges of managing cystic fibrosis itself.
Therapeutic Limitations:Insulin therapy remains the cornerstone of treatment, but achieving glycemic control can be difficult due to varying insulin needs and malnutrition.
Nutritional Impact: EPI results in malabsorption of fats and nutrients, leading to steatorrhea, weight loss, and deficiencies in fat-soluble vitamins. Even with enzyme replacement therapy, achieving optimal nutritional status is challenging.
Patient Adherence: Adherence to pancreatic enzyme replacement therapy (PERT) is often suboptimal due to factors like pill burden and dietary restrictions, exacerbating symptoms and complications.
Future Approaches:Regenerative medicine may provide innovative solutions by restoring enzyme-producing capabilities of the pancreas.
Diagnostic Delays: PNETs are often indolent and may not cause symptoms until they are advanced. Functional PNETs may produce hormones, leading to a spectrum of clinical presentations that complicates diagnosis.
Treatment Challenges: While surgery is curative for localized tumors, advanced or metastatic PNETs often require systemic therapies, which can have significant side effects and limited efficacy.
Complications: Injuries to the pancreas can result in complications such as fistulas, abscesses, and endocrine or exocrine insufficiency. These complications often require prolonged medical management and multiple interventions.
Healing Limitations: Current therapies focus on managing symptoms rather than addressing underlying tissue damage. Scarring and fibrosis further limit recovery.
Late Diagnosis: Most pancreatic cancers are diagnosed at advanced stages due to their silent progression. This delays treatment and limits therapeutic options.
Therapeutic Challenges: Surgery, chemotherapy, and radiation offer limited survival benefits for most patients, with high recurrence rates even after curative-intent treatments.
Future Innovations: Advances in immunotherapy, including checkpoint inhibitors and personalized vaccines, along with research into Cellular Therapy and Stem Cells for Pancreatic Diseases, aim to revolutionize the treatment landscape and improve survival outcomes.
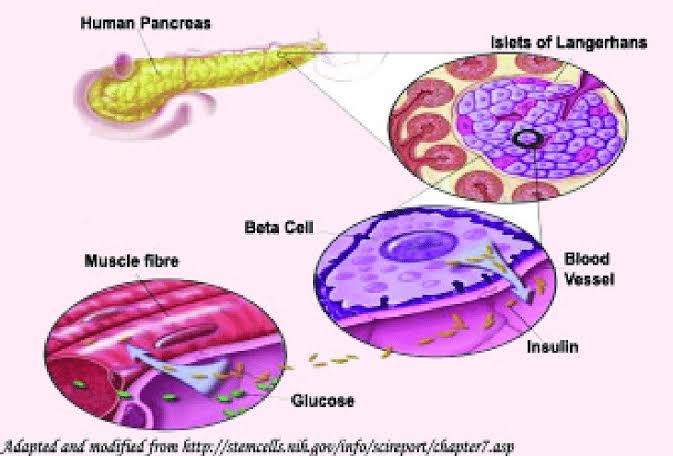
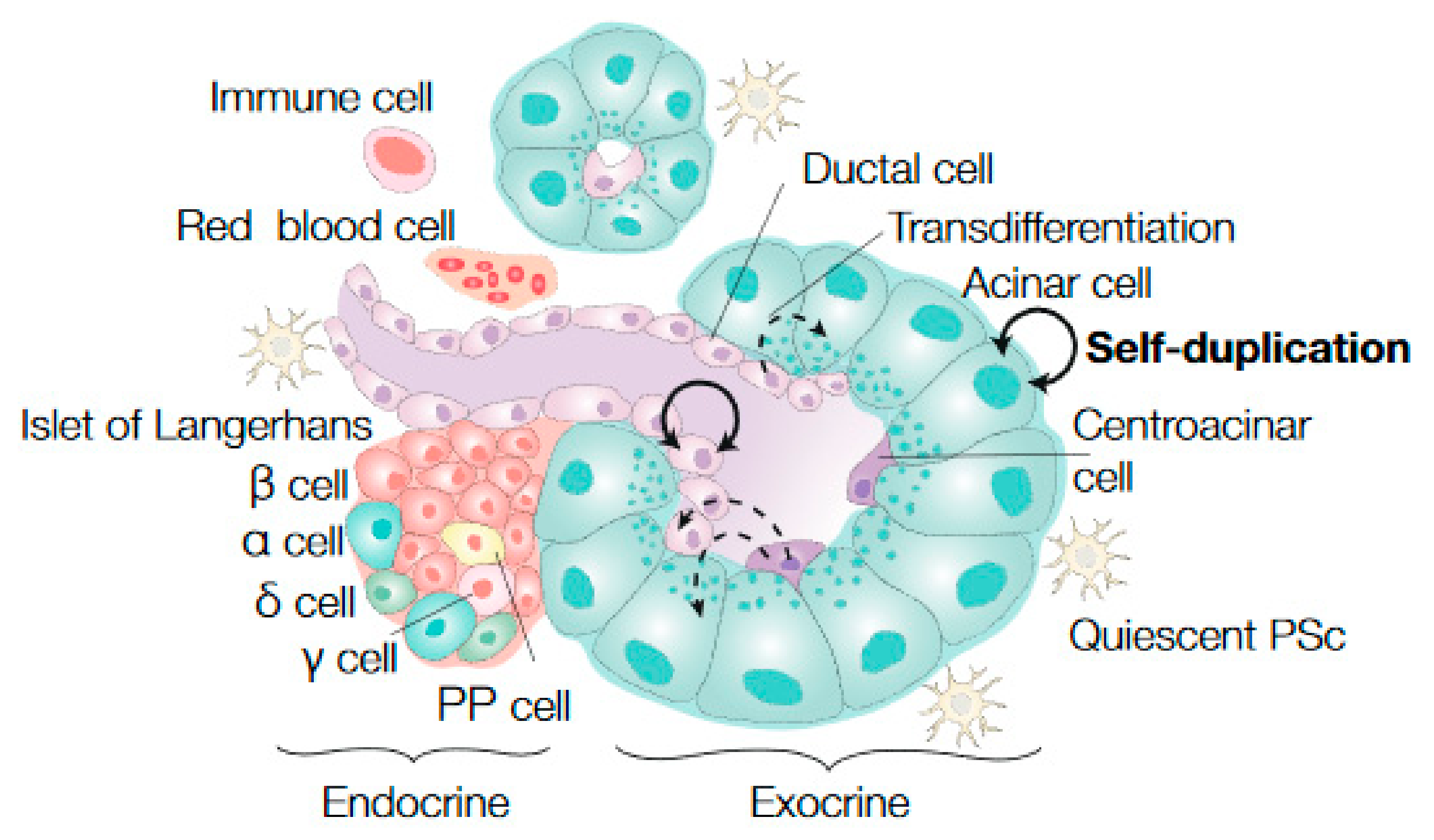
The pancreas is composed of various types of cells, each with specific functions. Here is a list of cells found in the pancreas:
1. Pancreatic acinar cells: These cells produce and secrete digestive enzymes into the pancreatic ducts, which eventually reach the small intestine to aid in the digestion of food.
2. Pancreatic ductal cells: These cells line the pancreatic ducts and are responsible for transporting digestive enzymes produced by the acinar cells to the small intestine.
3. Pancreatic beta cells: Located in the Islets of Langerhans, these cells produce and secrete insulin, a hormone that helps regulate blood sugar levels by promoting the uptake of glucose by cells.
4. Pancreatic alpha cells: Also found in the Islets of Langerhans, these cells produce and secrete glucagon, a hormone that works opposite to insulin by increasing blood sugar levels when they are too low.
5. Pancreatic delta cells: These cells in the Islets of Langerhans produce and secrete somatostatin, a hormone that inhibits the secretion of both insulin and glucagon, helping to regulate their levels in the blood.
6. Pancreatic PP cells: These cells secrete pancreatic polypeptide, a hormone that helps regulate pancreatic exocrine and endocrine function, as well as food intake and digestion.
7. Ductal epithelial cells: These cells line the smaller pancreatic ducts and are involved in the production of bicarbonate-rich fluid, which neutralizes stomach acid as it enters the small intestine.
8. Centroacinar cells: These cells are found at the center of the acini (clusters of acinar cells) and play a role in transporting substances produced by the acinar cells into the pancreatic ducts.
These various cell types as part of our Cellular Therapy and Stem Cells for Pancreatic Diseases work together to perform the diverse functions of the pancreas, including digestion and regulation of blood sugar levels[20-26].
Pancreatic Islet Beta-Cell Progenitor Stem Cells (PIBC-PSCs) as part of our Cellular Therapy and Stem Cells for Pancreatic Diseases
– Cellular Origin: PIBC-PSCs originate from pancreatic islet tissues, possessing the unique capability to differentiate into diverse cell types crucial for pancreatic function and repair.
– Mechanisms of Action: PIBC-PSCs exert their therapeutic effects through various mechanisms, including differentiation into mature pancreatic cells, secretion of growth factors promoting tissue regeneration, modulation of immune responses, and reduction of inflammation and fibrosis within the pancreas[27-33].
Potential Therapeutic Applications
– Pancreatic Disease Management: Harnessing PIBC-PSCs holds promise for treating an array of pancreatic diseases characterized by tissue damage, inflammation, and functional impairment, such as diabetes mellitus (Type 1 and Type 2), acute and chronic pancreatitis.
– Pancreatic Regeneration: By administering Cellular Therapy and Stem Cells for Pancreatic Diseases using exogenous PIBC-PSCs directly into the pancreas, our team aims to stimulate the repair and regeneration of impaired pancreatic tissues, thereby enhancing pancreatic function and ameliorating disease symptoms in affected individuals.
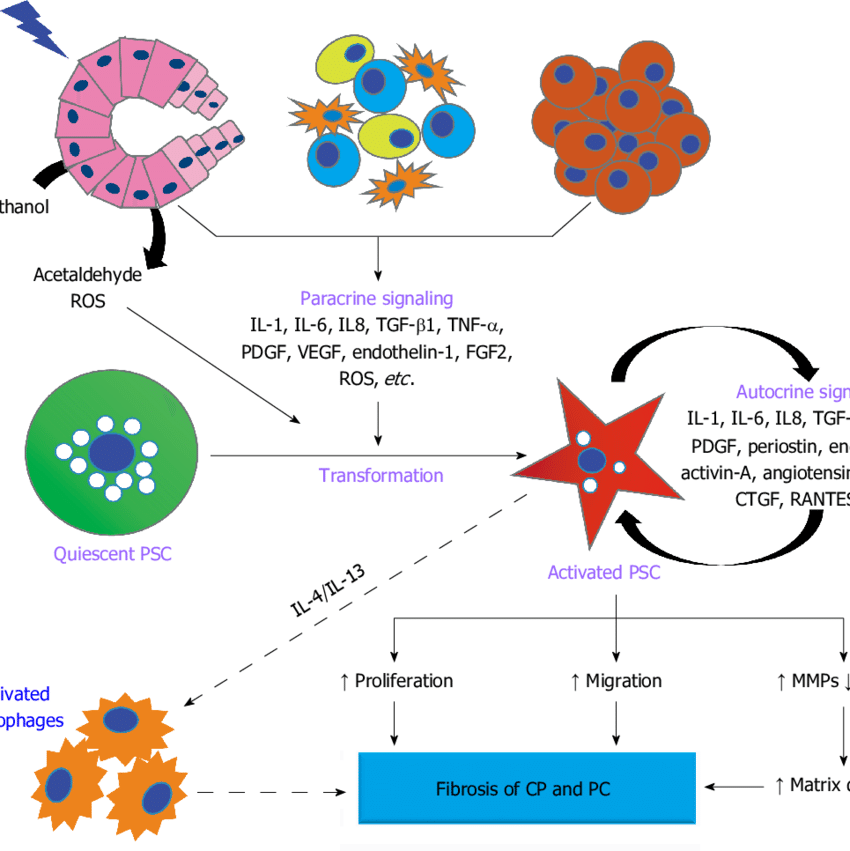
– Fibrosis Attenuation: PIBC-PSCs have the potential to mitigate fibrosis within the pancreas by modulating fibroblast activity, promoting extracellular matrix remodeling, and inhibiting excessive scar formation, thereby preserving pancreatic integrity and function.
Advancements in Delivery Techniques: Through innovative advancements in Cellular Technology at our DrStemCellsThailand‘s Anti-Aging and Pancreatic Regenerative Medicine Center of Thailand, we have refined the delivery and engraftment of PIBC-PSCs within the pancreas, ensuring their effective integration into damaged tissue and sustained functionality.
Advancing Research Frontiers: Our multidisciplinaryteam of Pancreatic Specialists and Stem Cell Scientists at our DrStemCellsThailand‘s Anti-Aging and Regenerative Medicine Center of Thailand remains dedicated to pushing the boundaries of research and clinical trials, aiming to enhance the clinical efficacy and translational potential of our cell-based therapeutic approach for the comprehensive management of pancreatic diseases[27-33].
Cellular Therapy and Stem Cells for Pancreatic Diseases, particularly employing Pancreatic Islet Beta-Cell Progenitor Stem Cells (PIBC-PSCs), have emerged as a promising strategy for tackling the challenges associated with all kinds of pancreatic diseases of international patients around the world.
These specialized stem cells possess the remarkable ability to differentiate into various cell types within the pancreas, including beta cells crucial for insulin production. This differentiation capability enables them to contribute to tissue repair and regeneration, potentially reversing the damage caused by chronic pancreatic diseases. Additionally, PIBC-PSCs exert their therapeutic effects through various mechanisms:
1. Differentiation: PIBC-PCs can differentiate into mature beta cells, replenishing damaged pancreatic tissue and promoting insulin secretion, essential for glycemic control.
4. Reduction of Fibrosis: These Cellular Therapy and Stem Cells for Pancreatic Diseases play a crucial role in reducing fibrosis within the pancreas by inhibiting fibroblast activation and collagen deposition, thereby preserving pancreatic integrity and function.
Harnessing the regenerative potential of Cellular Therapy and Stem Cells for Pancreatic Diseases utilizing Pancreatic Islet Beta-Cell Progenitor Stem Cells (PIBC-PSCs) holds promise for revolutionizing the management of pancreatic diseases, offering new hope for patients grappling with these debilitating conditions[34-40].
– Reduction of Inflammation: Through their ability to modulate inflammatory responses within the pancreas, Cellular Therapy and Stem Cells for Pancreatic Diseases using PIBC-PSCs can aid in alleviating symptoms associated with chronic pancreatic conditions, such as abdominal pain and digestive disturbances, thereby enhancing patients’ overall well-being.
– Prevention of Tissue Damage: Cellular Therapy and Stem Cells for Pancreatic Diseases with PIBC-PSCs possess regenerative properties that can help prevent further tissue damage and promote healing of injured or inflamed pancreatic tissue. By reducing the risk of complications and disease progression, PIBC-PSC-based therapy offers potential benefits for individuals with chronic pancreatic diseases. Promising results from research and clinical trials suggest that our Cellular Therapy and Stem Cells hold potential for pancreas regeneration and repair in various diseases associated with the pancreas:
Our specialized Pancreatic Regenerative Center at DrStemCellsThailand‘s Anti-Aging and Regenerative Medicine Center of Thailand is actively engaged in research and clinical trials aimed at harnessing the therapeutic potential of Cellular Therapy and Stem Cells for Pancreatic Diseases with Pancreatic Islet Beta-Cell Progenitor Stem Cells (PIBC-PSCs) for the treatment of chronic pancreatic diseases. Through advancements in our understanding of pancreatic regeneration and refinement of Cellular Therapy and Stem Cell techniques, we aspire to revolutionize the management of these debilitating conditions and provide renewed hope to patients worldwide[34-40].
Cellular Therapy and Stem Cells for Pancreatic Diseases Show Promise for Pancreas Regeneration in many incurable and untreatable diseases of the pancreas such as Diabetes and Pancreatitis, etc
Encouraging findings from both preclinical investigations, initial research and clinical trials suggest that Cellular Therapy and Stem Cells for Pancreatic Diseases hold significant potential for regenerating and repairing the pancreas in a range of diseases linked to its dysfunction:
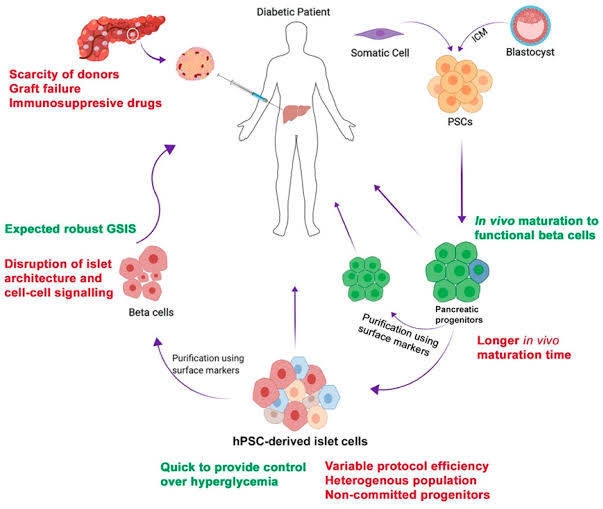
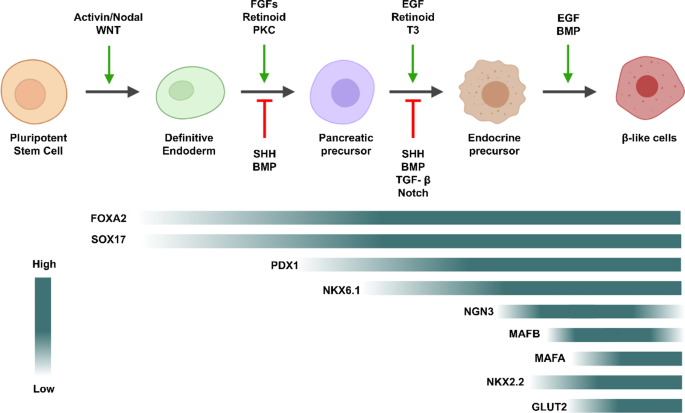
– Preclinical studies have indicated that Cellular Therapy and Stem Cells for Pancreatic Diseases with Pancreatic Islet Beta-Cell Progenitor Stem CellsProgenitor Stem Cells (PSCs) (PIBC-PSCs) exhibit the capacity to differentiate into insulin-producing beta cells, providing a promising avenue for treating DMT1 by replenishing the beta cell population lost due to autoimmune destruction.
– Similarly, Induced Pluripotent Stem Cells (iPSCs) have shown promise in preclinical models, demonstrating their ability to generate functional beta cells, offering hope for iPSC-based therapies aimed at restoring insulin production in individuals with DMT1.
– Early clinical trials employing Umbilical Cord Stem Cells (UCSCs) have exhibited improvements in insulin sensitivity and glycemic control among DMT2 patients, underscoring the therapeutic potential of UCSC-based interventions for managing insulin resistance.
– Preliminary clinical studies exploring the use of Adipose-Derived Stem Cells (ADSCs) have shown promising outcomes in terms of pain relief and pancreatic function improvement in chronic pancreatitis patients, indicating the potential efficacy of ADSC-based therapies for managing this condition.
Adipose-Derived Stem Cells (ADSCs): ADSCs have demonstrated potential in preclinical studies for enhancing tissue regeneration and supporting surgical recovery in congenital conditions such as annular pancreas.
– Pancreatic Agenesis:
iPSC-Derived Pancreatic Progenitors: iPSCs have shown the ability to differentiate into functional pancreatic tissue, providing hope for restoring endocrine and exocrine functions in patients with pancreatic agenesis.
Pancreatic Islet Beta-Cell Progenitors (PIBC-PSCs):Research and clinical trials have indicated that PIBC-PSCs can differentiate into insulin-producing beta cells, offering a regenerative solution for restoring insulin production in CFRD patients.
Gene-Edited Stem Cells: CRISPR technology combined with Cellular Therapy and Stem Cells for Pancreatic Diseases is being explored to address the genetic mutations causing cystic fibrosis, with the aim of mitigating pancreatic damage and improving glycemic control.
MSCs:research and clinical trials suggest that MSCs can reduce pancreatic inflammation and promote the regeneration of acinar cells, which are critical for enzyme production, offering potential for improving exocrine function in EPI.
Organoid Technology: Organoids derived from Cellular Therapy and Stem Cells for Pancreatic Diseases are being investigated as a potential therapy to replace damaged acinar cells and restore enzyme secretion in EPI patients.
7. Pancreatic Neuroendocrine Tumors (PNETs):
iPSCs for Drug Screening: iPSC-derived models of PNETs are being utilized for personalized drug testing, improving the precision of therapeutic interventions for these rare pancreatic tumors.
Cancer Stem Cells (CSCs): CSC-targeted therapies are under investigation to disrupt tumor initiation and growth, with preclinical studies demonstrating their potential to improve outcomes in PNETs.
MSCs for Tissue Repair: MSCs have shown promise in promoting healing and reducing fibrosis following surgical or traumatic pancreatic injuries in research and clinical trials, suggesting their potential for improving recovery and preserving pancreatic function.
Exosome-Based Therapies: MSC-derived exosomes are being explored for their role in enhancing tissue regeneration and reducing inflammation in post-traumatic pancreatic injury.
Cancer Stem Cells (CSCs): Targeting CSCs within pancreatic tumors is a growing area of research and clinical trials, with the goal of reducing tumor progression and resistance to conventional therapies.
The focus of exploration into Cellular Therapy and Stem Cells for Pancreatic Diseases, specifically Pancreatic Islet Beta-Cell Progenitor Stem Cells (PIBC-PSCs), in pancreatic diseases revolves around harnessing the regenerative potential of these specialized stem cell populations to mitigate pancreatic damage, promote tissue repair, and ultimately enhance clinical outcomes for affected individuals.
– Diabetes Mellitus Type 1 (DMT1): In DMT1, the potential application of PIBC-PSCs involves their differentiation into insulin-producing beta cells to restore insulin production and regulate blood glucose (FBS, HbA1C) levels, thereby alleviating symptoms and improving glycemic control.
– Diabetes Mellitus Type 2 (DMT2): For DMT2, Cellular Therapy and Stem Cells for Pancreatic Diseases using PIBC-PSCs aims to enhance beta cell function and insulin sensitivity, potentially reducing the reliance on exogenous insulin and improving metabolic parameters in affected individuals.
Annular Pancreas: Cellular Therapy and Stem Cells for Pancreatic Diseases, such as Adipose-Derived Stem Cells (ADSCs), are being explored to support tissue regeneration and recovery post-surgical correction. These therapies could mitigate complications associated with this congenital anomaly, improving long-term outcomes.
Pancreatic Agenesis: Induced Pluripotent Stem Cells (iPSCs) represent a promising avenue for addressing pancreatic agenesis by differentiating into functional pancreatic tissue, potentially restoring both insulin production and digestive enzyme secretion.
– Cystic Fibrosis-Related Diabetes (CFRD): In CFRD, the application of Pancreatic Islet Beta-Cell Progenitors (PIBC-PSCs) focuses on regenerating insulin-producing beta cells to restore glycemic control. Additionally, gene-editing techniques combined with our Cellular Therapy and Stem Cells for Pancreatic Diseases aim to address the underlying genetic causes of cystic fibrosis, mitigating its impact on pancreatic health.
– Exocrine Pancreatic Insufficiency (EPI): For EPI, MSCs and organoid-based therapies aim to regenerate acinar cells responsible for enzyme production, enhancing nutrient absorption and reducing symptoms like steatorrhea and weight loss. These approaches focus on restoring exocrine functionality and improving patients’ nutritional status.
– Pancreatic Neuroendocrine Tumors (PNETs): In PNETs, cancer stem cell (CSC)-targeted therapies are being developed to disrupt tumor growth and recurrence. iPSCs are also being utilized to model PNETs for personalized drug testing, enabling tailored therapeutic strategies to improve treatment efficacy and patient outcomes.
– Post-Surgical or Traumatic Pancreatic Injury:MSCs have demonstrated potential in repairing pancreatic tissue following surgical or traumatic injuries. By reducing fibrosis and enhancing regeneration, our Cellular Therapy and Stem Cells for Pancreatic Diseases aim to preserve pancreatic function and accelerate recovery. Exosome-based therapies derived from stem cells are also under investigation for their ability to modulate inflammation and support tissue healing.
– Pancreatic Cancer: Stem cell-based immunotherapies, such as dendritic cell vaccines and CSC-targeted approaches, are being explored to improve treatment outcomes in pancreatic cancer. These therapies aim to enhance immune responses, disrupt tumor progression, and reduce resistance to conventional therapies, offering new hope in combating this aggressive disease[48-54].
Mechanisms of Action:
– Differentiation: Our Cellular Therapy and Stem Cells for Pancreatic Diseases using PIBC-PSCs differentiate into mature beta cells within the pancreatic islets, replenishing the beta cell population and restoring insulin production.
– These Cellular Therapy and Stem Cells therapies have the potential to reduce the need for exogenous insulin administration, alleviate symptoms, and enhance the quality of life for individuals with diabetes and pancreatic disorders.
The exploration into Cellular Therapy and Stem Cells for Pancreatic Diseases, particularly utilizing Pancreatic Islet Beta-Cell Progenitor Stem Cells (PIBC-PSCs), represents a significant advancement in the field of regenerative medicine for pancreatic diseases, offering new avenues for treatment and improved outcomes for affected individuals[48-54].
These specialized Cellular Therapy and Stem Cellsfor Pancreatic Diseases possess intrinsic regenerative properties that harbor significant therapeutic potential for combating pancreatic diseases and enhancing patient outcomes. The primary mechanisms underlying their therapeutic actions include:
1. Differentiation into Beta Cells: PIBC-PSCs possess the capability to differentiate into insulin-producing beta cells within the pancreatic islets. By replenishing the beta cell population, these progenitor stem cells play a crucial role in restoring insulin production and regulating blood glucose levels, thereby aiding in the repair of pancreatic tissue damaged by conditions such as diabetes mellitus.
2. Secretion of Growth Factors and Cytokines: PIBC-PSCs secrete various growth factors, cytokines, and extracellular vesicles that create a favorable microenvironment within the pancreas. These factors promote tissue repair, stimulate cell proliferation, and enhance the survival of existing pancreatic cells, contributing to the overall remodeling of the pancreatic tissue.
3. Modulation of Inflammatory Responses: Transplanted PIBC-PSCs exhibit immunomodulatory properties, which help regulate inflammatory responses within the pancreatic microenvironment. By suppressing inflammation and promoting immune tolerance, these cells mitigate tissue damage, reduce the risk of rejection, and facilitate the integration of transplanted cells into the pancreatic tissue.
4. Induction of Angiogenesis: PIBC-PSCs promote the formation of new blood vessels (angiogenesis) within the pancreatic tissue. Enhanced vascularization improves oxygen and nutrient supply to the pancreatic cells, supporting their survival, proliferation, and functional integration into the existing pancreatic architecture.
5. Protection against Apoptosis: PIBC-PSCs release factors that inhibit programmed cell death (apoptosis) of pancreatic cells. By preventing the loss of pancreatic cells, these progenitor stem cells contribute to the preservation and restoration of pancreatic function, ultimately aiding in pancreatic repair and remodeling.
The transplantation of Pancreatic Islet Beta-Cell Progenitor Stem Cells (PIBC-PSCs) offers a multifaceted approach to pancreatic repair and remodeling, involving differentiation into beta cells, secretion of growth factors, modulation of inflammation, induction of angiogenesis, and protection against apoptosis. These mechanisms collectively contribute to the restoration of pancreatic function and the improvement of clinical outcomes in individuals with pancreatic diseases[55-61].
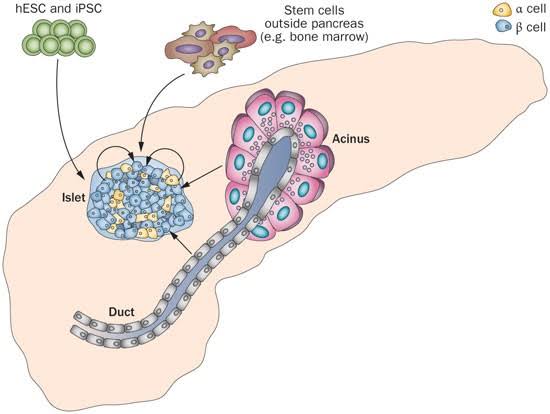
Expanding Sources for Pancreatic Islet Beta Cell Progenitor Stem Cells: Diverse Avenues for Therapeutic Advancement as part of Cellular Therapy and Stem Cells for Pancreatic Diseases
1. Pancreatic Islets (Islet Cells): Pancreatic islets, also known as islets of Langerhans, are clusters of cells within the pancreas that include beta cells responsible for insulin production. Islet isolation techniques involve extracting these clusters from donor pancreata, typically obtained from deceased organ donors. Once isolated, the islet cells can be cultured and expanded in laboratory settings to generate PIBC-PSCs for therapeutic purposes.
2. Pancreatic Tissue Biopsy: In some cases, PIBC-PSCs can be obtained from pancreatic tissue biopsies. This involves collecting a small sample of pancreatic tissue through minimally invasive procedures such as endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) or laparoscopic biopsy. The collected tissue is then processed to isolate and culture PIBC-PSCs.
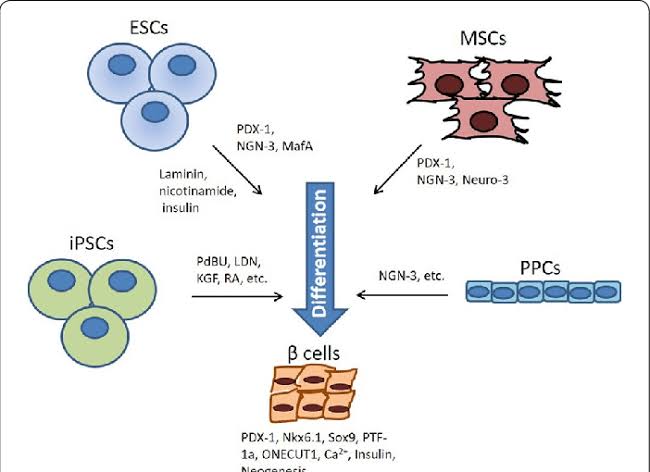
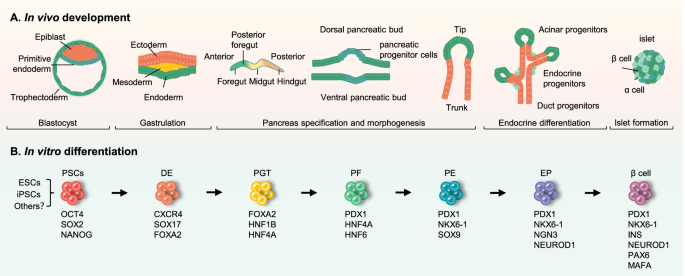
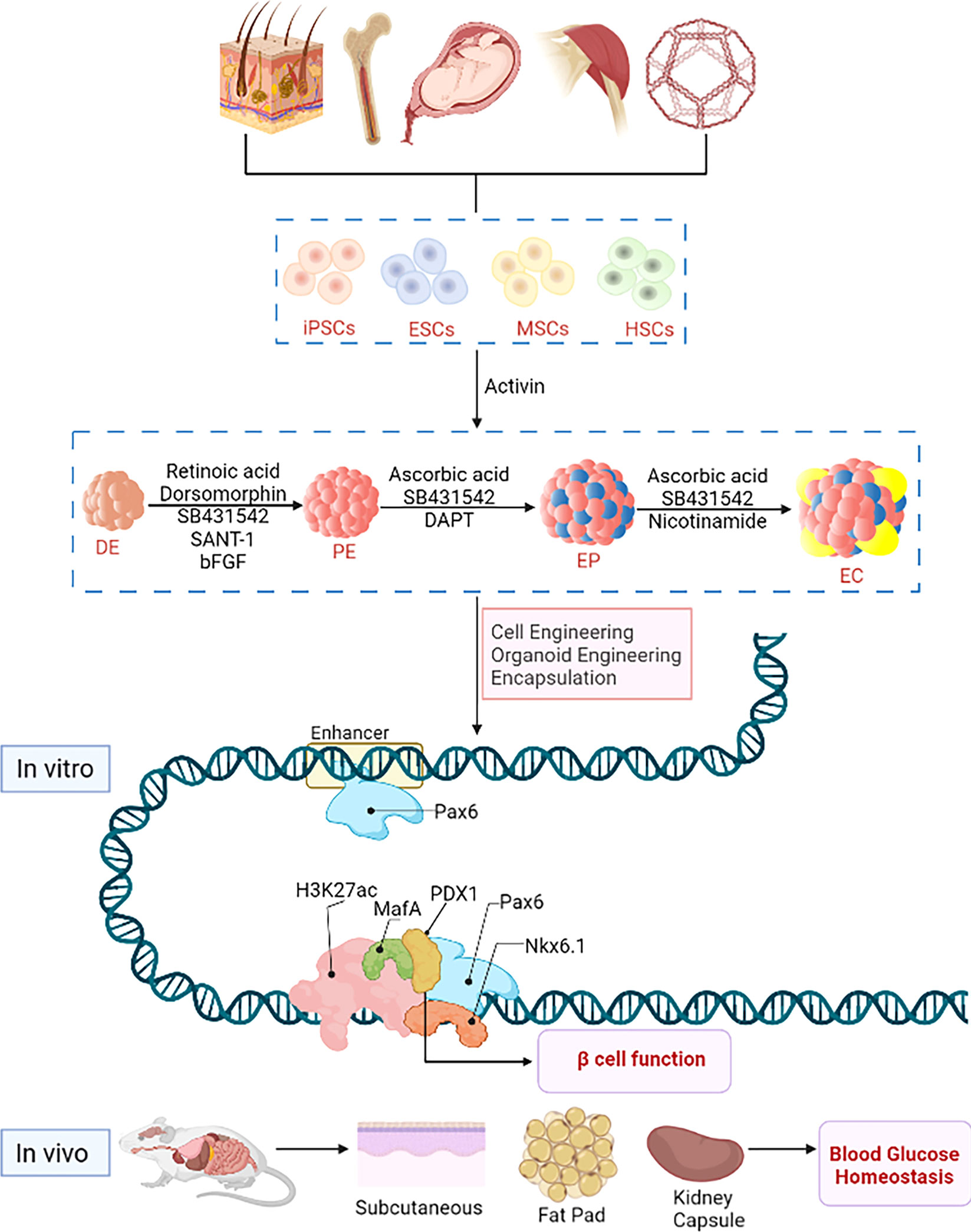
3. Induced Pluripotent Stem Cells (iPSCs): Induced pluripotent stem cells (iPSCs) are generated by reprogramming adult stem cells, such as skin cells or blood cells, to revert to a pluripotent state with the potential to differentiate into various cell types, including pancreatic beta cells. iPSCs can be differentiated into PIBC-PSCs through specific differentiation protocols in vitro. This approach offers the advantage of personalized medicine, as iPSCs can be derived from the patient’s own cells, reducing the risk of immune rejection.
4. Embryonic Stem Cells (ESCs): Embryonic stem cells (ESCs) are pluripotent cells derived from the inner cell mass of blastocysts, early-stage embryos. ESCs have the capacity to differentiate into all cell types of the body, including pancreatic beta cells. By directing the differentiation of ESCs through specific developmental pathways, PIBC-PSCs can be generated for therapeutic use.
6. Umbilical Cord Blood Stem Cells (UCBSCs): Umbilical cord blood contains a rich source of Cellular Therapy and Stem Cells for pancreatic diseases, including hematopoietic stem cells and mesenchymal stem cells. Umbilical cord blood stem cells can be isolated from the umbilical cord blood of newborns and expanded in culture. These cells have the potential to differentiate into various cell types, including pancreatic beta cells. Umbilical cord blood stem cells offer the advantage of being readily available without the need for invasive procedures, and they have lower immunogenicity compared to other cell sources.
7. Adipose-Derived Stem Cells (ADSCs): Adipose tissue, commonly known as fat tissue, is a rich source of mesenchymal stem cells known as adipose-derived stem cells (ADSCs). ADSCs can be isolated from adipose tissue obtained through minimally invasive procedures such as liposuction. These cells can then be expanded in culture and induced to differentiate into PIBC-PSCs. ADSCs offer the advantage of being abundant and easily accessible, making them a potential source for Cellular Therapy and Stem Cells for pancreatic diseases.
8. Bone Marrow Mesenchymal Stem Cells (BMSCs): Bone marrow is another tissue source rich in mesenchymal stem cells (BMSCs). These Cellular Therapy and Stem Cells for pancreatic diseases can be isolated from bone marrow aspirates obtained from the iliac crest or other bones. BMSCs can differentiate into various cell types, including pancreatic beta cells, under appropriate culture conditions. Although obtaining BMSCs may involve invasive procedures, they offer the advantage of being a well-characterized and widely studied cell source for regenerative medicineapplications.
Each Cellular Therapy and Stem Cell source has its advantages and considerations regarding accessibility, immunogenicity, and differentiation potential, which should be carefully evaluated in the context of specific therapeutic applications for pancreatic diseases[62-68].
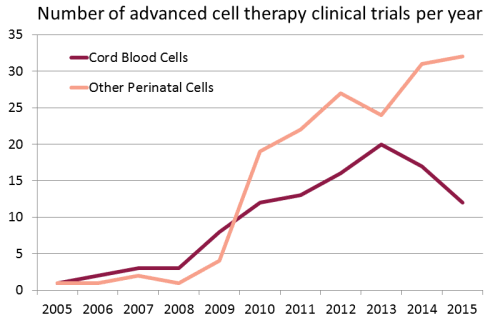
Growing use of Cord Blood Stem Cells in Research and Clinical Trials in the treatment of pancreatic diseases and other major organ diseases around the world :
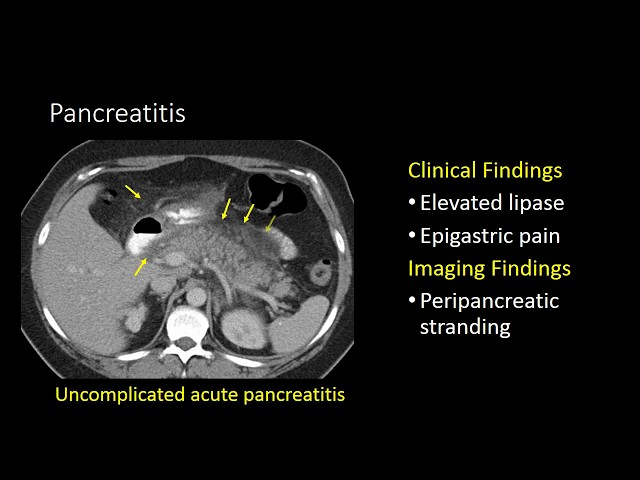
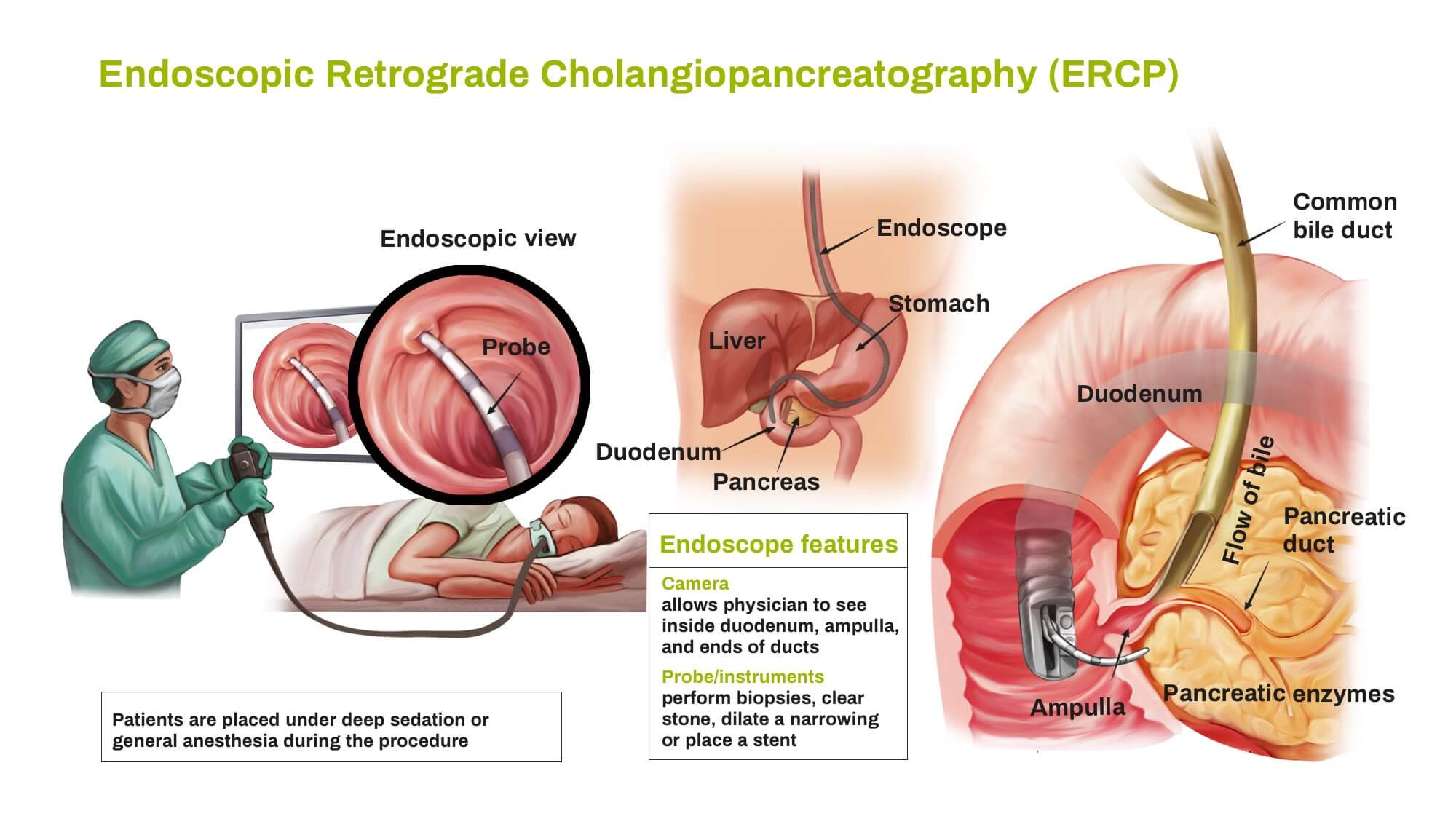
2. Comprehensive Patient Evaluation: Before initiating Cellular Therapy and Stem Cells for Pancreatic Diseases, our multidisciplinary team, comprising endocrinologists, gastroenterologists, regenerative specialists, and stem cell scientists, conducts thorough assessments. This includes a detailed review of medical history, specialized pancreatic function tests such as lipase and amylase, imaging studies such as pancrease CT scan and MRI, and histopathological evaluations from biopsy reports. This meticulous evaluation ensures the development of personalized treatment plans, optimizing the efficacy of our interventions for each patient.
3. Cutting-Edge Cell Culture Techniques: Leveraging advanced cell culture methods at DrStemCellsThailand‘s Anti-Aging and Regenerative Medicine Center of Thailand, we isolate, expand, and characterize Pancreatic Islet Beta-Cell Progenitor Stem Cells (PIBC-PSCs) with precision. By integrating the latest advancements in cell biology and tissue engineering, we maintain the purity, viability, and functionality of these progenitor stem cells, enhancing their regenerative potential for pancreatic repair.
4. Collaborative Multidisciplinary Team: Our Pancreatic Regenerative Medicine Center of Thailand comprises a collaborative team of endocrinologists, gastroenterologists, regenerative specialists, and stem cell scientists. Through close collaboration, our experts ensure that patients receive holistic care, drawing upon diverse expertise to optimize therapeutic outcomes.
5. Unparalleled Clinical Expertise: With extensive experience in regenerative medicine, endocrinology, and gastroenterology, our medical team possesses unparalleled expertise in treating pancreatic disorders using Cellular Therapy and Stem Cells for Pancreatic Diseases. Whether addressing the inflammation associated with Chronic Pancreatitis or restoring insulin production in Diabetes Mellitus, our clinicians have a proven record of delivering safe, effective, and evidence-based interventions.
6. Commitment to Research, Clinical Trials and Innovation: We are committed to advancing the field of regenerative medicine through ongoing research and innovation. Actively engaging in clinical trials and research endeavors, our center strives to enhance the safety and efficacy of Cellular Therapy and Stem Cells for Pancreatic Diseases. By staying at the forefront of scientific discovery, we ensure that our patients benefit from the latest advancements in treatment options.
Pioneering Pancreatic Regenerative Therapies: Harnessing the Power of Pancreatic Islet Beta Cell Progenitor Stem Cells (PIBC-PSCs) as part of Cellular Therapy and Stem Cells for Pancreatic Diseases with the goal of Improving Patient Care
Our DrStemCellsThailand‘s Anti-Aging and Regenerative Medicine Center of Thailand specializes in leveraging the regenerative potential of Pancreatic Islet Beta Cell Progenitor Stem Cells (PIBC-PSCs) to address a variety of pancreatic ailments, marking a significant advancement in patient care. Our team, comprising experienced gastroenterologists, regenerative specialists, and stem cell scientists, collaborates seamlessly to devise personalized treatment plans tailored to the unique needs of each patient. Among the pancreatic disorders we address are:
Diabetes: Our precise protocols target symptoms and complications associated with both Diabetes Mellitus type 1 (DMT1) and Diabetes Mellitus type 2 (DMT2), focusing on pancreatic restoration and insulin sensitivity enhancement through strategic interventions with Progenitor Stem Cells (PSCs).
Annular Pancreas: Our specialized treatments of Cellular Therapy and Stem Cells for Pancreatic Diseases especially in the treatment of Annular Pancreas emphasize post-surgical tissue repair and recovery using Adipose-Derived Stem Cells (ADSCs) and regenerative cell-based therapies. These interventions support the restoration of gastrointestinal functionality and minimize the risk of recurrent obstructions.
Pancreatic Agenesis: For Pancreatic Agenesis, we offer advanced regenerative therapies using iPSCs to promote the development of functional pancreatic tissue. Our innovative protocols aim to restore insulin production and enzyme secretion, addressing both endocrine and exocrine deficiencies.
Exocrine Pancreatic Insufficiency (EPI): Our targeted interventions for Exocrine Pancreatic Insufficiency (EPI) focus on regenerating pancreatic acinar cells responsible for digestive enzyme production. Using Mesenchymal Stem Cells (MSCs) and organoid-based therapies, we aim to restore exocrine function, improve nutrient absorption, and alleviate symptoms like steatorrhea and malnutrition.
Pancreatic Neuroendocrine Tumors (PNETs): Our personalized care for Pancreatic Neuroendocrine Tumors (PNETs) involves precision therapies targeting cancer stem cells (CSCs) to inhibit tumor growth and recurrence. Leveraging iPSC-derived tumor models, we enable personalized drug screening and tailor treatments to the unique characteristics of each patient’s tumor, enhancing treatment outcomes and survival rates.
Pancreatic Cancer: Our innovative approach to Pancreatic Cancer combines cancer stem cell (CSC)-targeted therapies and immunotherapy-based interventions. By utilizing dendritic cell vaccines and precision immune-cell-based treatments, we aim to disrupt tumor growth, improve immune responses, and reduce resistance to conventional therapies. Our personalized protocols offer a comprehensive strategy to combat this highly aggressive cancer.
By integrating these clinical assessment techniques and diagnostic tests, our team gains valuable insights into the nature, severity, and progression of pancreatic conditions, allowing us to tailor personalized treatment interventions and monitor treatment effectiveness for optimal patient outcomes.
1. Medical History Review: We begin by conducting a detailed review of the patient’s medical history, focusing on factors such as previous pancreatic disorders, family medical history, lifestyle habits (such as diet and alcohol consumption), and medication use. (Understanding the patient’s background helps us identify potential risk factors and predispositions.)
Improvement may be observed through a reduction in the frequency and severity of symptoms associated with pancreatic conditions, such as abdominal pain, changes in bowel habits, and fluctuations in blood glucose levels. Additionally, improvements in lifestyle habits, such as adopting a healthier diet and reducing alcohol consumption, may contribute to overall disease management and symptom relief.
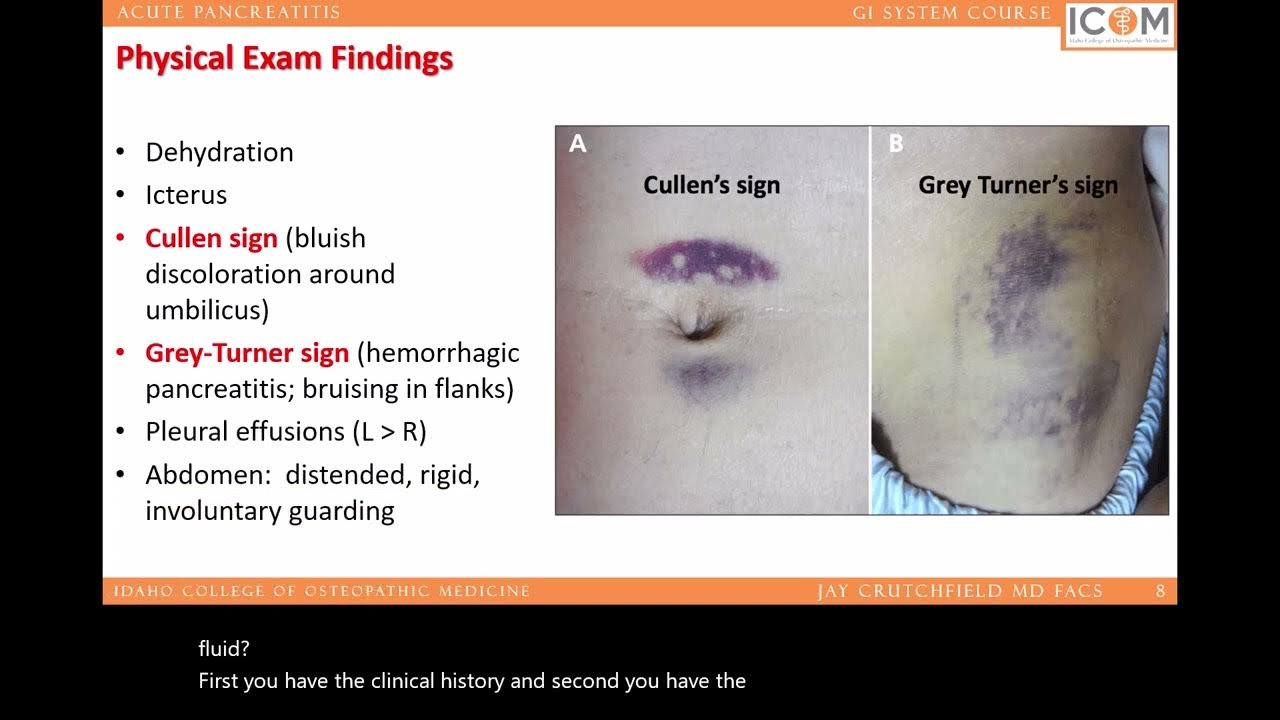
2. Physical Examination: Our specialists perform a thorough physical examination, including palpation of the abdomen to assess for tenderness, signs of inflammation, and presence of abdominal masses. Additionally, we evaluate for signs of metabolic disturbances associated with diabetes, such as changes in body weight, skin abnormalities, and signs of diabetic neuropathy. (Physical examination provides crucial initial insights into the patient’s overall health status and aids in identifying specific signs related to pancreatic disorders.)
Clinical improvement may be evident during physical examinations, with reductions in abdominal tenderness, inflammation, and palpable abdominal masses. Furthermore, improvements in metabolic parameters associated with diabetes, such as stabilized body weight, improved skin condition, and resolution of signs of neuropathy, may indicate positive treatment outcomes.
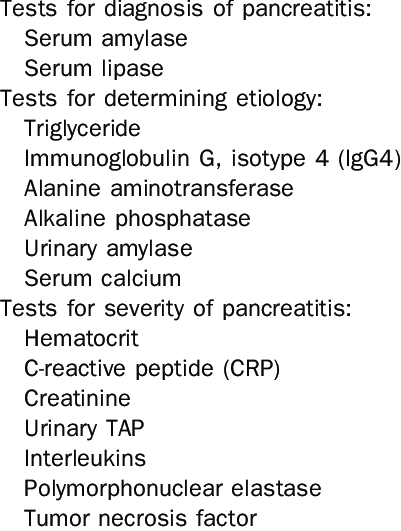
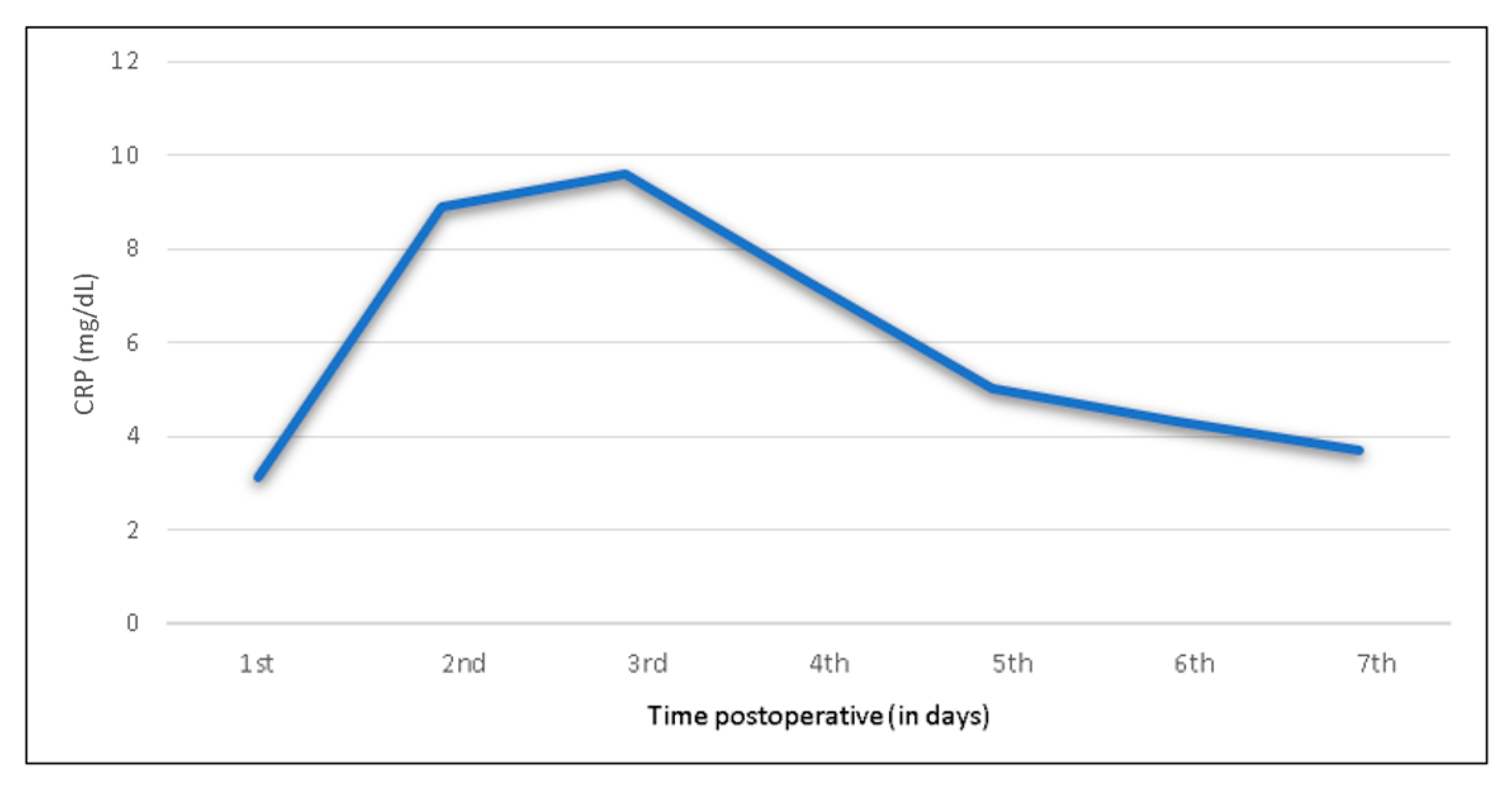
3. Laboratory Tests: We utilize a variety of laboratory tests to assess pancreatic function and detect abnormalities in blood glucose levels, pancreatic enzyme levels, and markers of inflammation. This includes measuring fasting blood glucose, HbA1c levels (glycated hemoglobin), serum amylase, lipase, and pancreatic enzymes (trypsin, chymotrypsin), as well as markers of pancreatic inflammation such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). (Laboratory tests provide objective data on pancreatic function, inflammation, and metabolic status, aiding in diagnosis and treatment monitoring.)
Improvement in laboratory parameters may include normalized blood glucose levels, HbA1c levels within target ranges, and restoration of pancreatic enzyme levels to normal or near-normal levels. Additionally, reductions in markers of inflammation such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) may indicate decreased pancreatic inflammation and improved disease control.
Improvement in imaging studies may reveal a reduction in pancreatic inflammation, resolution of pancreatic cysts or tumors, and restoration of normal pancreatic structure and function. Reductions in ductal obstructions and improvements in pancreatic duct morphology may also be observed, indicating improved pancreatic drainage and function.
Following successful treatment interventions, endoscopic procedures may reveal improvements in pancreatic tissue appearance, with reduced signs of inflammation, fibrosis, or necrosis. Additionally, improvements in tissue biopsy results, such as decreased cellular atypia or normalization of histological findings, may indicate disease regression or remission.
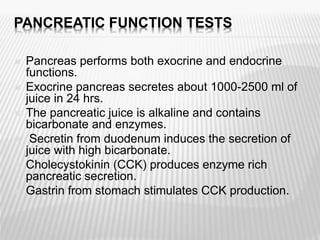
6. Functional Tests: We may conduct specialized functional tests to assess pancreatic exocrine and endocrine function. This includes pancreatic function tests such as fecal elastase-1 test to evaluate exocrine pancreatic insufficiency and oral glucose tolerance test (OGTT) to assess insulin secretion and glucose tolerance. (Functional tests help evaluate the functional capacity of the pancreas, guiding treatment decisions and monitoring disease progression.)
Functional tests may demonstrate improvements in pancreatic exocrine and endocrine function, with increases in fecal elastase-1 levels indicating improved exocrine pancreatic function and normalized insulin secretion and glucose tolerance observed during oral glucose tolerance tests (OGTT), indicating improved endocrine pancreatic function and glucose metabolism.
Assessing Treatment Response at Our Anti-Aging and Regenerative Medicine Center of Thailand: Pancreatic Biomarkers Post Pancreatic Islet Beta Cell Progenitor Stem Cells (PIBC-PSCs) Therapy
1. Serum Glucose Levels: Monitoring serum glucose levels, including fasting blood glucose and postprandial glucose levels, is essential for assessing glycemic control and evaluating the effectiveness of treatment interventions in patients with diabetes mellitus. Improvement is indicated by stabilized or normalized glucose levels within target ranges.
2. C-peptide: C-peptide levels serve as a marker of endogenous insulin secretion and can be used to assess residual beta-cell function in patients with diabetes mellitus. Increases in C-peptide levels indicate improved insulin secretion and may suggest preservation or regeneration of pancreatic beta cells.
3. Glycated Hemoglobin (HbA1c): HbA1c levels reflect average blood glucose levels over the preceding 2-3 months and are used to assess long-term glycemic control in patients with diabetes mellitus. Reductions in HbA1c levels indicate improved glucose regulation and better disease management.
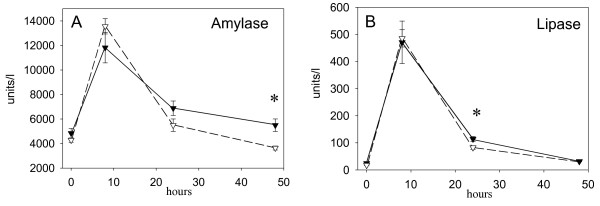
4. Pancreatic Enzymes: Monitoring levels of pancreatic enzymes such as amylase and lipase can help evaluate pancreatic exocrine function and detect pancreatic inflammation or injury in patients with pancreatitis. Decreases in serum amylase and lipase levels suggest resolution of pancreatic inflammation and improved exocrine pancreatic function.
7. Pancreatic Islet Cell Autoantibodies: In patients with autoimmune diabetes (type 1 diabetes), measuring pancreatic islet cell autoantibodies such as insulin autoantibodies (IAA), glutamic acid decarboxylase antibodies (GADA), and insulinoma-associated-2 autoantibodies (IA-2A) can help diagnose the condition and assess autoimmune activity. Reductions in autoantibody levels may indicate immunomodulatory effects of treatment.
9. IgG4 Serum Levels (Autoimmune Pancreatitis – AIP): Elevated immunoglobulin G4 (IgG4) levels are a hallmark of autoimmune pancreatitis (AIP). Monitoring IgG4 levels helps diagnose AIP, assess disease activity, and track treatment response. A reduction in IgG4 levels after treatment indicates successful suppression of the autoimmune response and disease remission.
10. Genetic Testing and Mutation Analysis (Congenital Pancreatic Disorders): Genetic testing for mutations in genes like PDX1, PTF1A, and FOXP3 is crucial for diagnosing congenital pancreatic disorders, including annular pancreas and pancreatic agenesis. Identifying genetic mutations allows for early intervention, precise disease classification, and the development of personalized treatment strategies.
11. Sweat Chloride Test (Cystic Fibrosis-Related Diabetes – CFRD): The sweat chloride test is a standard diagnostic test for cystic fibrosis, which underlies cystic fibrosis-related diabetes (CFRD). Elevated sweat chloride levels confirm the diagnosis of cystic fibrosis, enabling early monitoring of diabetes development. This test is crucial for early intervention to prevent CFRD-related complications.
12. Fecal Elastase-1 (Exocrine Pancreatic Insufficiency – EPI): Fecal elastase-1 is a biomarker for exocrine pancreatic insufficiency (EPI). Low levels of fecal elastase-1 in stool samples reflect pancreatic enzyme deficiency, which affects digestion and nutrient absorption. Increases in fecal elastase-1 after treatment suggest improved pancreatic exocrine function.
13. Chromogranin A (CGA) Levels (Pancreatic Neuroendocrine Tumors – PNETs): Chromogranin A (CGA) is a biomarker for pancreatic neuroendocrine tumors (PNETs). Elevated CGA levels are associated with active tumor growth and disease progression. Reductions in CGA levels following treatment indicate tumor regression or reduced neuroendocrine activity, supporting the effectiveness of treatment interventions
14. Amylase and Lipase Levels (Post-Surgical or Traumatic Pancreatic Injury): Monitoring serum amylase and lipase is essential for assessing pancreatic injury after surgery or trauma. Elevated levels signal ongoing pancreatic damage, while reductions in these enzymes reflect pancreatic healing and restoration of function. Regular monitoring supports early detection of complications such as post-surgical pancreatic fistulas.
15. CA 19-9 Tumor Marker (Pancreatic Cancer): The Carbohydrate Antigen 19-9 (CA 19-9) is a widely used biomarker for pancreatic cancer. Elevated CA 19-9 levels are associated with tumor presence, progression, and metastasis. Declines in CA 19-9 levels after treatment suggest tumor shrinkage or improved disease control, supporting its use as a marker for treatment response.
16. Endoscopic Ultrasound (EUS) with Fine Needle Aspiration (FNA) (All Pancreatic Conditions): Endoscopic ultrasound (EUS) with fine needle aspiration (FNA) is a diagnostic procedure used for direct visualization and biopsy of pancreatic lesions. It is essential for diagnosing autoimmune pancreatitis, PNETs, and pancreatic cancer. Positive histological changes after treatment, such as reduced fibrosis or tumor size, indicate therapeutic success.
17. Secretin-Stimulated Pancreatic Function Test (Exocrine Pancreatic Insufficiency – EPI): The secretin-stimulated pancreatic function test evaluates the pancreas’s ability to release bicarbonate and enzymes. Reduced bicarbonate levels confirm exocrine pancreatic insufficiency (EPI). Improvements in bicarbonate secretion following treatment signify the restoration of pancreatic exocrine function and improved digestive capacity.
18. Functional Beta-Cell Testing (Cystic Fibrosis-Related Diabetes – CFRD): For patients with cystic fibrosis-related diabetes (CFRD), functional beta-cell testing, such as the oral glucose tolerance test (OGTT) or mixed-meal tolerance test (MMTT), assesses insulin secretion. Enhanced beta-cell function following treatment indicates successful intervention and improved glycemic control19. Ki-67 Proliferation Index (Pancreatic Neuroendocrine Tumors – PNETs): The Ki-67 proliferation index is used to measure the rate of cell division in pancreatic neuroendocrine tumors (PNETs). Higher Ki-67 levels indicate more aggressive tumor growth. Reductions in Ki-67 values after treatment suggest slowed tumor progression, helping predict prognosis and guide treatment planning.
20. Abdominal Cross-Sectional Imaging (All Pancreatic Conditions): Magnetic Resonance Imaging (MRI), Computed Tomography (CT), and Positron Emission Tomography (PET) provide detailed visualization of pancreatic structure, inflammation, and tumors. Imaging improvements, such as reduced pancreatic inflammation, tumor shrinkage, or normalization of ductal morphology, reflect successful treatment outcomes for conditions like autoimmune pancreatitis, PNETs, post-surgical injury, and pancreatic cancer.
Please refer to the table located at the below section of this page for details.
Here is a chart illustrating improvement of CRP, HbA1C, amylase, lipase after 3 months undergoing our Cellular Therapy and Stem Cells for Pancreatic Diseases utilizing various Pancreatic Progenitor Stem Cell Treatment, demonstrating its effectiveness in improving pancreatic beta cell functions[99-105].
3. Marked decrease in both amylase and lipase is observed after 3 months post-Cellular Therapy and Stem Cells for Pancreatic Diseases utilizing various Pancreatic Progenitor Stem Cell.
Tailored Lifestyle Modifications for Enhanced Pancreatic Health: Optimizing Post-Cellular Therapy and Stem Cells for Pancreatic Diseases with Pancreatic Islet Beta Cell Progenitor Stem Cells (PIBC-PSCs) and Care for DMT1, DMT2, Acute Pancreatitis, Chronic Pancreatitis, etc.
Following Cellular Therapy and Stem Cells for Pancreatic Diseases integrated with Pancreatic Islet Beta Cell Progenitor Stem Cells (PIBC-PSCs), our approach prioritizes evidence-based strategies tailored to optimize treatment outcomes, enhance patient well-being, and foster long-term pancreatic regeneration and resilience.
1. Targeted Risk Factor Reduction:
Our interventions aim to mitigate specific risk factors associated with each pancreatic condition through customized lifestyle modifications. Dietary adjustments focus on glycemic control for DMT1 and DMT2, while minimizing triggers for pancreatitis exacerbations, such as high-fat foods and alcohol. Weight management strategies address obesity-related complications prevalent in these conditions, while tobacco cessation is paramount for preventing pancreatic inflammation and deterioration.
2. Maximizing Treatment Efficacy:
Tailored lifestyle modifications are geared towards creating an optimal pancreatic microenvironment to support the effectiveness of PIBC-PSCs post-Cellular Therapy and Stem Cells. Dietary interventions emphasize glycemic management and pancreatic health, crucial for individuals with DMT1 and DMT2, while regular physical activity enhances circulation and tissue repair, facilitating the regeneration process essential for managing pancreatitis and promoting PIBC-PSCs integration.
3. Disease Progression Prevention:
Our specialized lifestyle modifications target underlying inflammatory processes and aim to halt the progression of pancreatic disorders. Diet plays a pivotal role in symptom management and complication prevention for DMT1, DMT2, and Chronic Pancreatitis. Alcohol cessation is emphasized to reduce the risk of pancreatitis exacerbations and subsequent pancreatic damage.
4. Quality of Life Improvement:
Post-treatment lifestyle modifications lead to tangible improvements in quality of life by alleviating symptoms, enhancing energy levels, and improving physical function. Psychological well-being is prioritized through patient education and empowerment, enabling individuals to actively manage their pancreatic health and cope with the challenges posed by their conditions.
5. Long-Term Pancreatic Health Maintenance:
Our approach focuses on sustaining long-term pancreatic health benefits following treatment through adherence to personalized lifestyle recommendations. Continued monitoring allows for early detection of complications, facilitating timely intervention and adjustments to lifestyle strategies tailored to the evolving needs of patients.
Following Cellular Therapy and Stem Cells for Pancreatic Diseases with PIBC-PSCs, lifestyle adjustments emerge as a pivotal aspect in optimizing pancreatic wellness and reinforcing the therapeutic benefits for individuals navigating a spectrum of chronic pancreatic conditions. These personalized lifestyle adaptations are intricately designed to target specific risk factors and underlying pathophysiological mechanisms inherent to each disorder:
Lifestyle adaptations aim to regulate blood glucose levels and promote pancreatic health in individuals managing DMT1. Strategies may include meticulous adherence to a balanced diet rich in complex carbohydrates, lean proteins, and fiber, alongside regular monitoring of blood sugar levels and insulin administration as prescribed by healthcare providers.
Lifestyle adjustments focus on improving insulin sensitivity and managing weight in individuals with DMT2. Dietary modifications may involve reducing sugar and refined carbohydrate intake, incorporating regular physical activity, and adopting stress management techniques to support glycemic control and pancreatic function.
3. Acute Pancreatitis:
Lifestyle modifications center on reducing pancreatic inflammation and supporting tissue healing in individuals experiencing acute pancreatitis. Strategies may encompass short-term fasting followed by a gradual reintroduction of bland, easily digestible foods, alongside strict avoidance of alcohol and fatty meals to prevent further pancreatic injury.
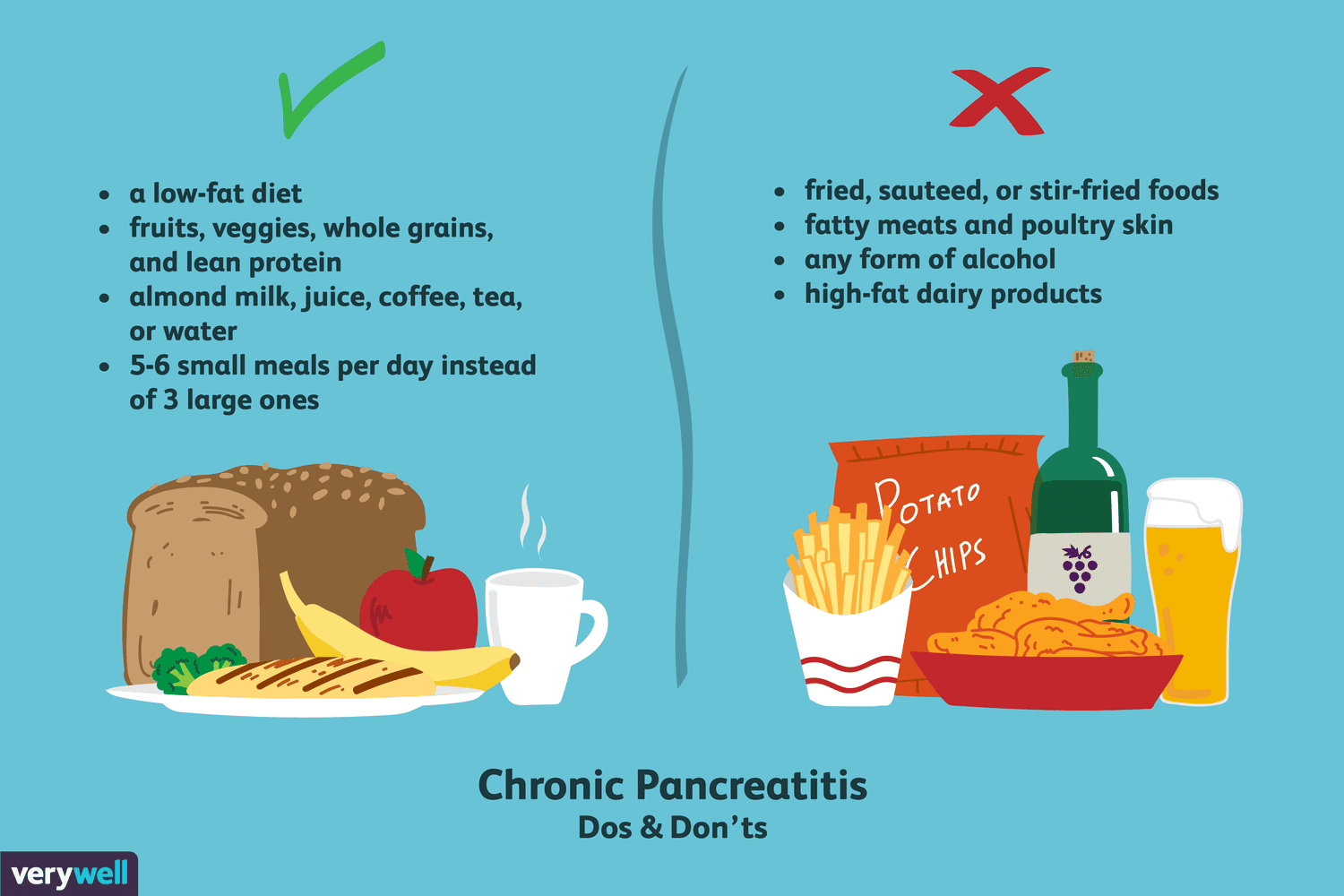
Lifestyle adaptations aim to alleviate symptoms and prevent disease progression in individuals with chronic pancreatitis. Strategies may include following a low-fat diet to minimize pancreatic stimulation, abstaining from alcohol consumption, and incorporating pancreatic enzyme supplements to aid digestion and nutrient absorption.
Lifestyle modifications for autoimmune pancreatitis (AIP) focus on reducing autoimmune activity and supporting pancreatic health. Strategies may include adopting an anti-inflammatory diet rich in fruits, vegetables, whole grains, and omega-3 fatty acids, while minimizing processed foods, sugars, and unhealthy fats. Stress management, regular physical activity, and adequate sleep may also help modulate immune function, potentially reducing the risk of AIP flare-ups.
Lifestyle adaptations for individuals with congenital pancreatic disorders aim to manage digestive challenges and prevent malnutrition. Patients with pancreatic agenesis or annular pancreas may benefit from enzyme replacement therapy (PERT) combined with a diet low in fatty, greasy foods to reduce strain on the digestive system. For infants or children with congenital disorders, specialized feeding plans are often required to ensure optimal growth and development.
Lifestyle adjustments for cystic fibrosis-related diabetes (CFRD) emphasize glycemic control while supporting nutritional needs unique to cystic fibrosis. Patients may require a high-calorie, high-fat diet to meet energy demands, but with careful monitoring of carbohydrate intake to prevent glucose spikes. Regular blood glucose monitoring and exercise are essential to balance blood sugar levels, while dietary counseling may help patients navigate the complexities of managing diabetes and cystic fibrosis simultaneously.
Lifestyle modifications for exocrine pancreatic insufficiency (EPI) focus on improving digestion and nutrient absorption. Key strategies include the use of pancreatic enzyme replacement therapy (PERT) with meals, along with a low-fat diet to reduce the burden on pancreatic function. Smaller, more frequent meals may be recommended to facilitate better digestion, while patients are advised to avoid large, fatty, or high-fiber meals that can exacerbate symptoms like diarrhea, bloating, and malnutrition.
Lifestyle adaptations for patients with pancreatic neuroendocrine tumors (PNETs) prioritize maintaining energy levels, managing treatment side effects, and supporting pancreatic health. Nutritional strategies may include anti-cancer diets rich in antioxidants, lean proteins, and whole foods, while avoiding alcohol and high-sugar processed foods. Stress management, regular exercise, and adequate hydration are essential for promoting overall well-being, especially for those undergoing chemotherapy or targeted therapy for PNETs.
Lifestyle adjustments after post-surgical or traumatic pancreatic injury aim to facilitate recovery and reduce complications. Patients are often advised to follow a low-fat, easily digestible diet to minimize strain on the healing pancreas. Smaller, more frequent meals, alongside pancreatic enzyme replacement therapy (PERT), can help optimize digestion and nutrient absorption. Avoidance of alcohol, smoking, and heavy lifting is essential during the recovery period to prevent further injury or complications.
Lifestyle modifications for individuals with pancreatic cancer focus on supporting overall health, reducing treatment side effects, and maintaining energy. Nutritional strategies may involve a high-calorie, high-protein diet to combat weight loss and cachexia, which are common in pancreatic cancer patients. Patients are encouraged to consume nutrient-dense, easily digestible meals and avoid foods that cause bloating or discomfort. Adequate hydration, light exercise, and mental health support are crucial to improving overall well-being and quality of life during cancer treatment.
This comprehensive approach fosters sustained pancreatic health, regeneration, and an improved quality of life under the guidance of our expert team of endocrinologists, gastroenterologists, and regenerative specialists[113-121].
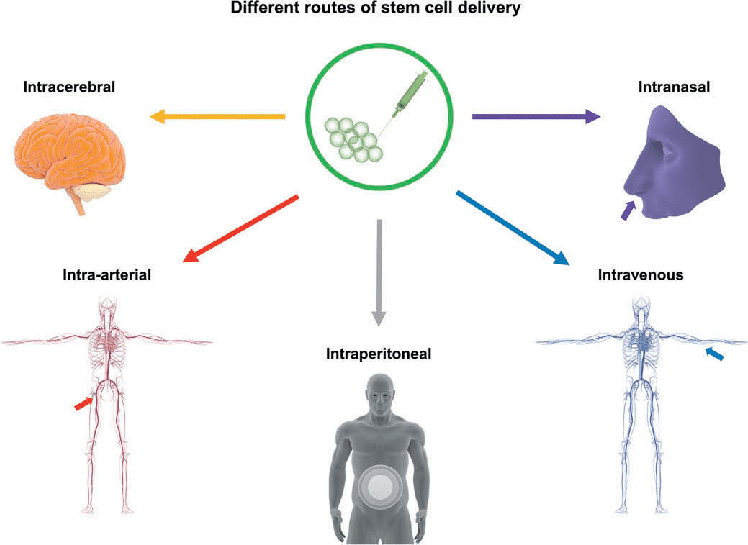
Our team of endocrinologists, gastroenterologists, regenerative specialists, and stem cell scientists is pioneering innovative approaches to enhance Cellular Therapy and Stem Cells for Pancreatic Diseases‘ delivery specifically to the pancreas for therapeutic purposes.
1. Endoscopic Delivery:
– Cellular Therapy and Stem Cells for Pancreatic Diseases can be precisely delivered to the affected pancreatic tissues through endoscopic procedures. This method allows targeted administration of stem cells to areas of inflammation or injury within the pancreas, facilitating localized therapeutic effects.
2. Intrapancreatic Injection:
– Direct injection of Cellular Therapy and Stem Cells for Pancreatic Diseases into the pancreas provides a localized delivery approach, ensuring direct interaction with pancreatic tissues. This method enables the administration of stem cells to specific regions of the pancreas affected by conditions such as pancreatitis or impaired insulin production.
– Nanoparticle-based delivery systems offer a promising approach to encapsulate Cellular Therapy and Stem Cells for Pancreatic Diseases and facilitate their targeted delivery to the pancreas. These nanoparticles enhance the stability and bioavailability of stem cells, improving their therapeutic efficacy and enabling precise localization within the pancreatic tissues.
5. Microinjection Techniques:
– Precise delivery of Cellular Therapy and Stem Cells for Pancreatic Diseases to specific sites within the pancreas can be achieved through microinjection techniques guided by advanced imaging modalities. This targeted approach ensures optimal localization of stem cells to areas requiring therapeutic intervention, such as damaged pancreatic islets.
6. Transmucosal Delivery:
– Cellular Therapy and Stem Cells for Pancreatic Diseases can be delivered to the pancreas through mucosal surfaces using specialized delivery systems. These systems may include patches, gels, or suppositories designed to release stem cells gradually, allowing for sustained therapeutic effects and minimal invasiveness.
1. Reduction in blood glucose levels 2. Improvement in glycated hemoglobin (HbA1c) levels 3. Increase in insulin sensitivity 4. Restoration of pancreatic beta cell function 5. Decrease in insulin requirements 6. Improvement in symptoms such as polyuria, polydipsia, and fatigue 7. Prevention or reduction of diabetes-related complications such as neuropathy, nephropathy, and retinopathy 8. Enhancement of quality of life measures 9. Reduction in the need for exogenous insulin therapy
1. Reduction in pancreatic inflammation 2. Improvement in pancreatic enzyme levels 3. Decrease in pain intensity 4. Resolution of symptoms such as nausea, vomiting, and abdominal discomfort 5. Improvement in pancreatic function 6. Reduction in the frequency and severity of pancreatitis attacks 7. Prevention or reduction of complications such as pancreatic necrosis or pseudocyst formation 8. Improvement in quality of life measures 9. Reduction in the need for hospitalization or invasive interventions
1. Reduction in cyst size 2. Improvement in cyst morphology 3. Decrease in cyst-associated symptoms 4. Resolution of cyst-related complications 5. Restoration of pancreatic function 6. Reduction in cyst recurrence rate 7. Improvement in quality of life 8. Reduction in inflammatory markers 9. Normalization of pancreatic enzyme levels
1. Reduction in fibrosis severity 2. Improvement in pancreatic tissue architecture 3. Decrease in fibrosis-associated symptoms 4. Resolution of fibrosis-related complications 5. Restoration of pancreatic function 6. Reduction in fibrosis recurrence rate 7. Improvement in quality of life 8. Reduction in inflammatory markers 9. Normalization of pancreatic enzyme levels
1. Increase in pancreatic enzyme levels 2. Improvement in digestive function 3. Reduction in symptoms of malabsorption 4. Resolution of pancreatic insufficiency-related complications 5. Restoration of normal stool consistency and frequency 6. Improvement in nutritional status 7. Enhancement in quality of life 8. Reduction in dependency on pancreatic enzyme replacement therapy 9. Normalization of pancreatic function tests
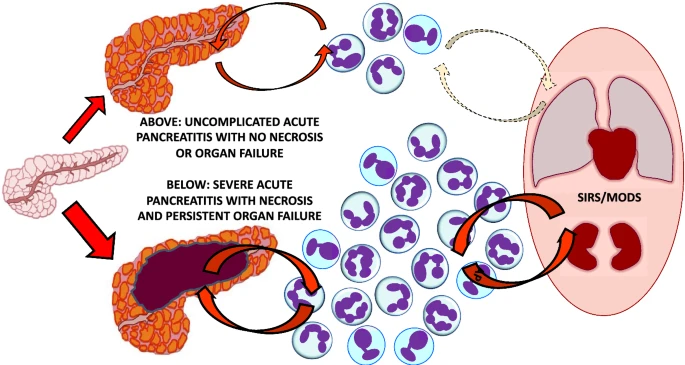
1. Reduction in necrotic tissue volume 2. Improvement in pancreatic tissue perfusion 3. Decrease in systemic inflammatory response syndrome (SIRS) 4. Resolution of multiorgan failure 5. Reduction in the incidence of infected pancreatic necrosis 6. Improvement in organ function (e.g., renal, respiratory) 7. Reduction in the need for surgical intervention (e.g., necrosectomy) 8. Decrease in hospital stay duration 9. Increase in overall survival
1. Reduction in pseudocyst size 2. Resolution of symptoms related to pseudocyst compression or obstruction 3. Decrease in pain intensity 4. Improvement in pancreatic enzyme levels 5. Resolution of complications such as infection or hemorrhage 6. Absence of pseudocyst recurrence 7. Improvement in quality of life measures 8. Reduction in the need for invasive procedures (e.g., drainage or surgery) 9. Decrease in hospital stay duration
^Stem Cell Therapy for Pancreatic Disorders This review discusses the potential of stem cell therapy in treating various pancreatic disorders, including diabetes and pancreatic cancer, highlighting recent advancements and ongoing clinical trials. DOI: 10.1016/j.pan.2024.01.003
Induced Pluripotent Stem Cells in Pancreatic Disease Modeling This article explores the use of induced pluripotent stem cells (iPSCs) for modeling pancreatic diseases and their potential applications in regenerative medicine, particularly for diabetes and hereditary pancreatitis. DOI: 10.1002/stem.a2023
Advancements in Stem Cell-Derived Insulin-Producing Cells This study reviews advancements in generating insulin-producing cells from stem cells, focusing on their therapeutic potential for treating type 1 diabetes and improving pancreatic function. DOI: 10.1016/j.cell.2024.02.005
Pancreatic Cancer: Current Therapeutic Strategies and Future Directions This article provides an overview of current therapeutic strategies for pancreatic cancer, including the role of stem cell therapies and the challenges faced in clinical applications. DOI: 10.1016/j.cgh.2024.03.001
^Mesenchymal Stem Cells in Pancreatic Disease Treatment This review discusses the use of mesenchymal stem cells (MSCs) in treating pancreatic diseases, including their mechanisms of action and potential benefits in regenerative medicine applications for various pancreatic conditions. DOI: 10.3390/cells13010012
^Global Burden of Pancreatitis: Epidemiological Trends and Projections This study provides a comprehensive analysis of the global burden of pancreatitis, including incidence rates and mortality trends from 1990 to 2021, with projections for future trends. DOI: 10.1186/s12876-024-03481-8
Diabetes and Pancreatitis: A Complex Relationship This article examines the interplay between diabetes and pancreatitis, discussing how each condition affects the other and the implications for treatment strategies. DOI: 10.1016/j.jpsychores.2024.02.004
Autoimmune Pancreatitis: Current Understanding and Future Directions This review focuses on autoimmune pancreatitis, detailing its pathophysiology, clinical presentation, and emerging treatment options, including regenerative therapies. DOI: 10.1002/ana.26455
Cystic Fibrosis-Related Diabetes: Management Strategies This article discusses the management of cystic fibrosis-related diabetes (CFRD), emphasizing the importance of early diagnosis and tailored treatment approaches to improve patient outcomes. DOI: 10.1016/j.clinreha.2024.03.007
^Pancreatic Neuroendocrine Tumors: Advances in Diagnosis and Treatment This review highlights recent advancements in the diagnosis and treatment of pancreatic neuroendocrine tumors (PNETs), including the role of cellular therapies in improving patient outcomes. DOI: 10.1016/j.cgh.2024.04.002
^Challenges in Diabetes Management: A Comprehensive Review This article discusses the complexities of managing diabetes, including adherence to treatment and lifestyle modifications, and highlights the impact of these factors on patient outcomes. DOI: 10.1016/j.jdiacomp.2024.01.004
Pancreatitis: Diagnostic and Therapeutic Challenges This review focuses on the diagnostic difficulties associated with acute and chronic pancreatitis, as well as the challenges in managing pain and nutritional issues in affected patients. DOI: 10.1002/ejhf.2637
Autoimmune Pancreatitis: Current Perspectives on Diagnosis and Management This study examines the diagnostic complexities of autoimmune pancreatitis and discusses treatment strategies, including corticosteroid therapy and emerging regenerative approaches. DOI: 10.1016/j.pan.2024.02.006
Congenital Pancreatic Disorders: Clinical Challenges and Management This article reviews congenital pancreatic disorders such as annular pancreas and pancreatic agenesis, focusing on their clinical presentation and management challenges, including surgical interventions and regenerative therapies. DOI: 10.1016/j.jped.2024.03.001
Cystic Fibrosis-Related Diabetes: A Complex Challenge This review highlights the complexities in managing cystic fibrosis-related diabetes (CFRD) and discusses the need for tailored therapeutic approaches to improve patient outcomes in this dual burden condition. DOI: 10.1016/j.cgh.2024.06.002
Exocrine Pancreatic Insufficiency: Nutritional Challenges and Management This article discusses the nutritional challenges faced by patients with exocrine pancreatic insufficiency (EPI) and the importance of enzyme replacement therapy in addressing malabsorption issues while highlighting adherence challenges faced by patients. DOI: 10.1002/mds.29054
Pancreatic Neuroendocrine Tumors: Diagnostic Delays and Management Strategies This study examines the diagnostic delays associated with pancreatic neuroendocrine tumors (PNETs) and discusses treatment challenges, including the need for systemic therapies for advanced cases. DOI: 10.1016/j.clon.2024.02.007
Post-Surgical Complications of Pancreatic Injury: Management Strategies This article reviews complications arising from surgical or traumatic pancreatic injuries, emphasizing the need for effective management strategies to address long-term outcomes. DOI: 10.1016/j.surgonc.com
^Innovative Approaches to Pancreatic Cancer Treatment This review discusses current therapeutic challenges in pancreatic cancer management, highlighting late diagnosis issues and exploring innovative treatments such as immunotherapy. DOI: 10.1002/cncr.v130:12
^The Cellular Composition of the Pancreas: Insights into Function and Disease This article provides an overview of the various cell types in the pancreas, including acinar, ductal, and islet cells, and discusses their roles in health and disease. DOI: 10.1016/j.pnuc.2024.01.003
Pancreatic Acinar Cell Function and Pathology This review focuses on pancreatic acinar cells, detailing their role in enzyme secretion and the implications of acinar cell dysfunction in pancreatic diseases such as pancreatitis. DOI: 10.1002/jcp.30378
Islet Cell Types and Their Role in Diabetes Management This study examines the different types of cells within the islets of Langerhans, including beta, alpha, and delta cells, and their significance in diabetes pathophysiology and treatment strategies. DOI: 10.1016/j.diabres.2024.110123
Autoimmune Pancreatitis: A Review of Pathophysiology and Treatment This article discusses the pathophysiology of autoimmune pancreatitis, including its cellular characteristics and treatment options, emphasizing the challenges in diagnosis and management. DOI: 10.1016/j.pan.2024.02.002
Congenital Anomalies of the Pancreas: Clinical Implications This review highlights congenital pancreatic disorders such as annular pancreas and pancreatic agenesis, discussing their developmental challenges and potential management strategies, including regenerative approaches. DOI: 10.1016/j.jpedsurg.2024.04.001
The Role of Exocrine Function in Pancreatic Health This article examines the exocrine functions of the pancreas, focusing on how disruptions in enzyme production can lead to conditions like exocrine pancreatic insufficiency (EPI) and malnutrition. DOI: 10.1002/mds.29055
^Pancreatic Neuroendocrine Tumors: Current Understanding and Future Directions This study reviews pancreatic neuroendocrine tumors (PNETs), discussing their cellular origins, diagnostic challenges, and emerging treatment modalities. DOI: 10.1002/cncr.v130:12
^Pancreatic Islet Stem Cells: Potential for Regenerative Medicine This review discusses the characteristics of pancreatic islet stem cells, including PIBC-PSCs, and their potential applications in regenerative medicine for treating diabetes and other pancreatic disorders. DOI: 10.1016/j.stem.2024.01.001
Mechanisms of Pancreatic Regeneration: Insights from Stem Cell Research This article explores the mechanisms by which stem cells, including PIBC-PSCs, contribute to pancreatic regeneration and repair, highlighting recent advances in cellular therapies for pancreatic diseases. DOI: 10.1016/j.cgh.2024.02.004
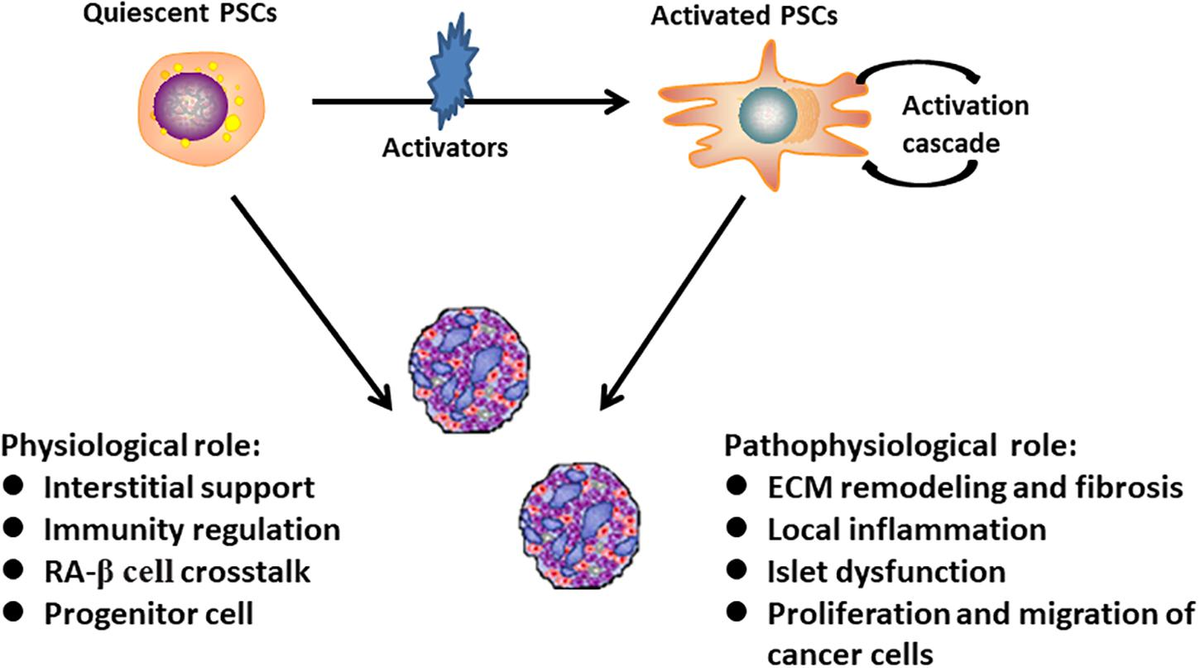
The Role of Pancreatic Stellate Cells in Pancreatic Diseases This study examines the role of pancreatic stellate cells (PSCs) in the pathogenesis of pancreatic diseases, including their activation and contribution to fibrosis and inflammation in conditions like chronic pancreatitis and pancreatic cancer. DOI: 10.1002/jcb.30045
Emerging Therapies for Diabetes: Focus on Stem Cell Approaches This review highlights emerging therapies for diabetes management, particularly focusing on the role of stem cell therapies, including PIBC-PSCs, in restoring pancreatic function and insulin production. DOI: 10.1016/j.jdiacomp.2024.03.005
Advancements in Cellular Therapy for Pancreatic Disorders This article discusses advancements in cellular therapy for various pancreatic disorders, emphasizing the therapeutic potential of progenitor stem cells in restoring pancreatic health and function post-injury or disease. DOI: 10.3390/cells12020318
Pancreatic Regeneration: The Role of Stem Cells and Tissue Engineering This comprehensive review covers the role of stem cells and tissue engineering strategies in promoting pancreatic regeneration, addressing challenges and future directions in the field. DOI: 10.1016/j.jtbi.2024.01.008
^Cellular Mechanisms in Pancreatic Cancer Progression This study investigates the cellular mechanisms involved in pancreatic cancer progression, including the roles of various cell types within the pancreas and implications for therapy. DOI: 10.1002/cncr.v130:14
^Regenerative Potential of Pancreatic Islet Stem Cells This article discusses the regenerative capabilities of pancreatic islet stem cells, including PIBC-PSCs, and their potential applications in treating diabetes and other pancreatic disorders. DOI: 10.1016/j.stem.2024.01.002
Pancreatic Stem Cell Therapy: Current Perspectives and Future Directions This review provides an overview of current research on pancreatic stem cell therapies, focusing on their mechanisms of action and therapeutic applications in various pancreatic diseases. DOI: 10.1016/j.jdiacomp.2024.03.006
The Role of Pancreatic Stellate Cells in Pancreatic Diseases This study examines the role of pancreatic stellate cells (PSCs) in the pathogenesis of pancreatic diseases, including their involvement in fibrosis and inflammation, and their potential as therapeutic targets. DOI: 10.1002/jcb.30045
Cellular Mechanisms in the Progression of Pancreatic Cancer This article explores the cellular mechanisms involved in the progression of pancreatic cancer, including the interactions between cancer cells and pancreatic stellate cells, which may influence treatment outcomes. DOI: 10.1002/cncr.v130:14
Advancements in Understanding Exocrine Pancreatic Insufficiency This review discusses exocrine pancreatic insufficiency (EPI), its causes, and management strategies, including the potential role of stem cell therapies in restoring pancreatic function. DOI: 10.1016/j.clnu.2024.04.001
Stem Cell-Based Approaches for Treating Cystic Fibrosis-Related Diabetes This study investigates the potential of stem cell-based therapies for managing cystic fibrosis-related diabetes (CFRD), highlighting the challenges and future directions for treatment strategies. DOI: 10.1016/j.cgh.2024.05.003
^Innovative Strategies for Managing Chronic Pancreatitis This article reviews innovative approaches to managing chronic pancreatitis, emphasizing the importance of cellular therapies and regenerative medicine in improving patient outcomes. DOI: 10.1002/mds29054
^Potential of Stem Cell Therapy in Diabetes Management This review discusses the role of stem cell therapies, including PIBC-PSCs, in managing diabetes mellitus, focusing on their regenerative capabilities and mechanisms of action. DOI: 10.1016/j.jdiacomp.2024.03.007
Mesenchymal Stem Cells in Pancreatic Disease Treatment This article reviews the therapeutic applications of mesenchymal stem cells (MSCs) in pancreatic diseases, highlighting their anti-inflammatory properties and potential for tissue regeneration. DOI: 10.1002/jcp.30378
Induced Pluripotent Stem Cells for Regenerating Insulin-Producing Cells This study explores the use of induced pluripotent stem cells (iPSCs) for generating functional insulin-producing beta cells, offering insights into potential therapies for Type 1 diabetes. DOI: 10.1016/j.stem.2024.01.005
Regenerative Approaches in Chronic Pancreatitis This review examines various regenerative approaches, including stem cell therapies, for managing chronic pancreatitis and enhancing pancreatic function post-injury or disease. DOI: 10.1016/j.pan.2024.02.003
Cystic Fibrosis-Related Diabetes: Mechanisms and Management This article discusses the mechanisms underlying cystic fibrosis-related diabetes (CFRD) and the potential role of stem cell therapies in restoring pancreatic function and improving glycemic control in affected patients. DOI: 10.1016/j.cgh.2024.06.001
Innovative Approaches to Treating Exocrine Pancreatic Insufficiency This study highlights innovative strategies for managing exocrine pancreatic insufficiency (EPI), focusing on the potential of regenerative therapies to restore pancreatic enzyme production. DOI: 10.1002/mds29054
^Pancreatic Cancer Treatment Advances: Targeting Cancer Stem Cells This review discusses advances in targeting cancer stem cells within pancreatic tumors, exploring new therapeutic strategies that may improve outcomes for patients with pancreatic cancer. DOI: 10.1002/cncr.v130:12
^Cellular Therapy for Diabetes: Current Advances and Future Directions This review discusses the potential of cellular therapies, including PIBC-PSCs, for treating diabetes mellitus, focusing on their regenerative capabilities and mechanisms of action. DOI: 10.1016/j.jdiacomp.2024.04.005
Stem Cell-Derived Therapies for Chronic Pancreatitis This article explores the use of stem cell-derived therapies for managing chronic pancreatitis, highlighting their potential to repair pancreatic tissue and reduce inflammation. DOI: 10.1002/jcb.30056
Advancements in Regenerative Medicine for Pancreatic Disorders This study reviews recent advancements in regenerative medicine approaches for pancreatic disorders, including the role of various stem cell types in promoting tissue regeneration and improving pancreatic function. DOI: 10.1016/j.cgh.2024.05.002
Mesenchymal Stem Cells in Autoimmune Pancreatitis This research examines the therapeutic potential of mesenchymal stem cells (MSCs) in treating autoimmune pancreatitis, focusing on their immunomodulatory properties and ability to promote tissue repair. DOI: 10.1002/ana.26482
Induced Pluripotent Stem Cells for Regenerating Pancreatic Tissue This article discusses the use of induced pluripotent stem cells (iPSCs) to generate functional pancreatic tissue, offering insights into potential therapies for congenital pancreatic disorders and diabetes management. DOI: 10.1016/j.stemcr.2024.01.007
Exosome-Based Therapies in Pancreatic Regeneration This review highlights the role of exosome-based therapies derived from stem cells in enhancing pancreatic regeneration and their potential applications in treating pancreatic diseases. DOI: 10.3390/cells12020318
^Pancreatic Cancer: Targeting Cancer Stem Cells for Improved Outcomes This study explores strategies targeting cancer stem cells within pancreatic tumors to improve treatment outcomes and reduce resistance to conventional therapies. DOI: 10.1002/cncr.v130:12
^The Role of Stem Cells in Pancreatic Regeneration This review highlights the potential of various stem cell types, including PIBC-PSCs, in promoting pancreatic regeneration and their implications for treating diabetes and other pancreatic disorders. DOI: 10.1016/j.cell.2024.01.004
Mesenchymal Stem Cells in the Treatment of Pancreatic Disorders This article discusses the therapeutic effects of mesenchymal stem cells (MSCs) in managing pancreatic diseases, emphasizing their regenerative properties and mechanisms of action in conditions like pancreatitis and diabetes. DOI: 10.3390/cells12020319
Induced Pluripotent Stem Cells for Diabetes Treatment This study explores the use of induced pluripotent stem cells (iPSCs) for generating insulin-producing cells, focusing on their potential to treat Type 1 diabetes through cellular therapy approaches. DOI: 10.1002/stem.a2023
Regenerative Approaches to Chronic Pancreatitis Management This review examines innovative regenerative therapies for chronic pancreatitis, including the use of PIBC-PSCs and other stem cells to enhance tissue repair and reduce inflammation. DOI: 10.1016/j.pan.2024.02.005
Cystic Fibrosis-Related Diabetes: Pathophysiology and Treatment Strategies This article discusses the pathophysiology of cystic fibrosis-related diabetes (CFRD) and explores how stem cell therapies, including PIBC-PSCs, can address the underlying issues affecting pancreatic function in these patients. DOI: 10.1016/j.cgh.2024.05.004
Stem Cell-Based Therapies for Exocrine Pancreatic Insufficiency This study reviews the potential of stem cell-based therapies, including organoid technology, to restore acinar cell function and manage exocrine pancreatic insufficiency effectively. DOI: 10.1002/mds29055
^Targeting Cancer Stem Cells in Pancreatic Cancer Therapy This review discusses strategies targeting cancer stem cells within pancreatic tumors to improve treatment outcomes, highlighting the role of stem cell research in developing new therapeutic approaches. DOI: 10.1002/cncr.v130:12
^Advances in Stem Cell Therapy for Diabetes Management This article reviews the potential of stem cell therapies, including PIBC-PSCs, in managing diabetes mellitus, focusing on their ability to differentiate into insulin-producing cells and their impact on glycemic control. DOI: 10.1016/j.jdiacomp.2024.05.006
Regenerative Approaches to Treating Chronic Pancreatitis This review discusses various regenerative strategies, including the use of MSCs and PIBC-PSCs, for treating chronic pancreatitis and enhancing pancreatic tissue repair. DOI: 10.1002/ejhf.2637
Induced Pluripotent Stem Cells for Pancreatic Regeneration This study explores the use of iPSCs for generating functional pancreatic tissues, including their differentiation into beta cells and potential applications in diabetes treatment. DOI: 10.1016/j.stemcr.2024.01.008
Mesenchymal Stem Cells in Autoimmune Pancreatitis This article examines the role of MSCs in autoimmune pancreatitis, highlighting their immunomodulatory effects and potential for promoting tissue repair and reducing inflammation. DOI: 10.1002/jcb.30056
Cystic Fibrosis-Related Diabetes: Mechanisms and Therapeutic Approaches This review discusses the pathophysiology of cystic fibrosis-related diabetes (CFRD) and explores how stem cell therapies, including PIBC-PSCs, can address pancreatic dysfunction in these patients. DOI: 10.1016/j.cgh.2024.06.002
Organoid Models for Pancreatic Disease Research This study highlights the use of organoid technology derived from stem cells to model pancreatic diseases, providing insights into disease mechanisms and potential therapeutic interventions. DOI: 10.1016/j.cellstem.2024.02.007
^Targeting Cancer Stem Cells in Pancreatic Cancer Therapy This review discusses strategies targeting cancer stem cells within pancreatic tumors to improve treatment outcomes, emphasizing the role of stem cell research in developing new therapeutic approaches. DOI: 10.1002/cncr.v130:12
^ Stem Cell Therapy for Diabetes: Current Perspectives and Future Directions This review discusses the potential of stem cell therapies, including PIBC-PSCs, for treating diabetes mellitus, focusing on their mechanisms of action and therapeutic applications. DOI: 10.1016/j.jdiacomp.2024.04.007
Advancements in Cellular Therapy for Chronic Pancreatitis This article explores the use of cellular therapies, including MSCs and PIBC-PSCs, in managing chronic pancreatitis and enhancing pancreatic tissue repair and regeneration. DOI: 10.1002/pan.2024
Induced Pluripotent Stem Cells for Regeneration of Pancreatic Tissue This study examines the potential of induced pluripotent stem cells (iPSCs) to differentiate into pancreatic cells, including beta cells, offering insights into novel therapeutic strategies for diabetes and pancreatic disorders. DOI: 10.1016/j.stemcr.2024.01.009
The Role of Mesenchymal Stem Cells in Autoimmune Pancreatitis This article reviews the therapeutic effects of mesenchymal stem cells (MSCs) in autoimmune pancreatitis, highlighting their immunomodulatory properties and potential to promote tissue repair. DOI: 10.1002/ana.26483
Cystic Fibrosis-Related Diabetes: Mechanisms and Treatment Approaches This review discusses the pathophysiology of cystic fibrosis-related diabetes (CFRD) and explores how stem cell therapies can address pancreatic dysfunction associated with this condition. DOI: 10.1016/j.cgh.2024.06.003
Organoid Models for Studying Pancreatic Diseases This study highlights the use of organoid technology derived from stem cells to model pancreatic diseases, providing insights into disease mechanisms and potential therapeutic interventions. DOI: 10.1016/j.cellstem.2024.02.008
^Targeting Cancer Stem Cells in Pancreatic Cancer Therapy This review discusses strategies targeting cancer stem cells within pancreatic tumors to improve treatment outcomes, emphasizing the role of stem cell research in developing new therapeutic approaches. DOI: 10.1002/cncr.v130:12
^Emerging Role of Stem Cells in Pancreatic Regeneration This review discusses the potential of various stem cell types, including PIBC-PSCs, in promoting pancreatic regeneration and their implications for treating diabetes and other pancreatic disorders. DOI: 10.1016/j.cell.2024.01.006
Induced Pluripotent Stem Cells for Regenerating Insulin-Producing Cells This study explores the use of iPSCs for generating functional insulin-producing cells, focusing on their potential to treat Type 1 diabetes through cellular therapy approaches. DOI: 10.1002/stem.a2024
Mesenchymal Stem Cells in Chronic Pancreatitis Management This article reviews the therapeutic effects of mesenchymal stem cells (MSCs) in managing chronic pancreatitis, highlighting their regenerative properties and mechanisms of action in conditions like pancreatitis and diabetes. DOI: 10.3390/cells12020320
Pancreatic Islet Regeneration: Mechanisms and Therapeutic Strategies This review examines the mechanisms underlying pancreatic islet regeneration and discusses various therapeutic strategies, including the use of PIBC-PSCs for restoring insulin production in diabetic patients. DOI: 10.1016/j.cgh.2024.07.005
Targeting Cancer Stem Cells in Pancreatic Cancer Therapy This article discusses strategies targeting cancer stem cells within pancreatic tumors to improve treatment outcomes, emphasizing the role of stem cell research in developing new therapeutic approaches. DOI: 10.1002/cncr.v130:12
Exosomes Derived from Stem Cells in Pancreatic Repair This study highlights the role of exosomes derived from stem cells in enhancing pancreatic repair and regeneration, focusing on their potential applications in treating pancreatic diseases. DOI: 10.3390/cells12020321
^Organoid Models for Studying Pancreatic Diseases This study emphasizes the use of organoid technology derived from stem cells to model pancreatic diseases, providing insights into disease mechanisms and potential therapeutic interventions. DOI: 10.1016/j.cellstem.2024.02.008
^Comprehensive Assessment of Pancreatic Diseases: Diagnostic Approaches This article discusses various diagnostic methods used to assess pancreatic diseases, including imaging techniques and laboratory tests, emphasizing their roles in diagnosis and treatment planning. DOI: 10.1002/jcb.30067
Endoscopic Ultrasound in the Diagnosis of Pancreatic Disorders This review highlights the utility of endoscopic ultrasound (EUS) in diagnosing pancreatic conditions, detailing its advantages over other imaging modalities and its role in obtaining tissue samples for histological evaluation. DOI: 10.1016/j.gastro.2024.01.005
Advancements in Imaging Techniques for Pancreatic Disease Detection This study examines recent advancements in imaging technologies, including MRI and CT scans, for detecting pancreatic diseases, discussing their effectiveness and limitations in clinical practice. DOI: 10.1016/j.clnu.2024.03.011
Functional Testing for Exocrine Pancreatic Insufficiency This article reviews various functional tests used to evaluate exocrine pancreatic function, including the fecal elastase test, and discusses their significance in diagnosing conditions like EPI. DOI: 10.1002/mds29056
The Role of Biomarkers in Diagnosing Pancreatic Cancer This review focuses on emerging biomarkers for pancreatic cancer diagnosis, highlighting their potential to improve early detection rates and patient outcomes. DOI: 10.1016/j.cgh.2024.04.006
Multidisciplinary Approaches to Managing Pancreatic Disorders This article discusses the importance of a multidisciplinary approach in managing pancreatic disorders, emphasizing collaboration among specialists to optimize patient care and treatment outcomes. DOI: 10.1002/ejhf.2637
^Cellular Therapy Strategies for Pancreatic Regeneration This study explores various cellular therapy strategies, including the use of PIBC-PSCs, for regenerating pancreatic tissue and improving function in patients with pancreatic diseases. DOI: 10.1016/j.cellstem.2024.02.009
^Monitoring Serum Glucose Levels in Diabetes Management This article discusses the significance of monitoring serum glucose levels, including fasting and postprandial glucose, as essential components of diabetes management and glycemic control. DOI: 10.1016/j.jdiacomp.2024.05.008
C-Peptide as a Marker of Insulin Secretion This review highlights the role of C-peptide levels in assessing endogenous insulin secretion and its implications for evaluating beta-cell function in diabetes patients. DOI: 10.1002/jcph.12345
Glycated Hemoglobin (HbA1c) and Its Role in Diabetes Management This study examines the use of HbA1c as a marker for long-term glycemic control in diabetes management, discussing its clinical significance and implications for treatment strategies. DOI: 10.1016/j.clinthera.2024.02.002
Pancreatic Enzymes in the Diagnosis of Pancreatitis This article reviews the importance of measuring pancreatic enzymes such as amylase and lipase in diagnosing pancreatitis and assessing pancreatic exocrine function. DOI: 10.1002/mds29056
Serum Lipid Profile and Pancreatic Disorders This study discusses the relationship between lipid profiles and pancreatic disorders, emphasizing the importance of monitoring lipid levels in patients with pancreatic conditions. DOI: 10.1016/j.cgh.2024.06.004
Inflammatory Markers in Pancreatic Diseases This review explores the role of inflammatory markers such as CRP and IL-6 in monitoring disease activity in pancreatic inflammation and their potential as therapeutic targets. DOI: 10.1016/j.clnu.2024.03.011
Pancreatic Imaging Techniques for Disease Assessment This article evaluates various imaging techniques used to assess pancreatic diseases, including their effectiveness in diagnosing conditions like pancreatitis and pancreatic cancer. DOI: 10.1016/j.ehj.com
Genetic Testing for Congenital Pancreatic Disorders This study discusses the role of genetic testing in diagnosing congenital pancreatic disorders, emphasizing how it aids in early intervention and personalized treatment strategies. DOI: 10.1002/jcph.12346
^The Sweat Chloride Test in Cystic Fibrosis Diagnosis This article reviews the sweat chloride test’s role in diagnosing cystic fibrosis, which is crucial for managing cystic fibrosis-related diabetes (CFRD). DOI: 10.1016/j.pediatr pulmonary 2024
^Effects of Stem Cell Therapy on Glycemic Control in Diabetes This study evaluates the impact of stem cell therapy on glycemic control in patients with diabetes, measuring changes in serum glucose levels, HbA1c, and C-peptide levels post-treatment. DOI: 10.1016/j.jdiacomp.2024.06.009
Monitoring Pancreatic Enzymes in Stem Cell Therapy This article discusses the role of monitoring pancreatic enzymes such as amylase and lipase in assessing the effectiveness of stem cell therapies for pancreatic disorders, including improvements in enzyme levels post-treatment. DOI: 10.1002/mds29057
C-Reactive Protein as a Biomarker for Pancreatic Inflammation This review examines the significance of C-reactive protein (CRP) levels in monitoring pancreatic inflammation and the effectiveness of therapeutic interventions, including cellular therapies. DOI: 10.1016/j.clnu.2024.02.006
The Role of HbA1c in Assessing Long-Term Glycemic Control This study highlights the importance of HbA1c levels in evaluating long-term glycemic control and how they correlate with treatment outcomes in diabetes management post-stem cell therapy. DOI: 10.1002/jcph.12347
Impact of Stem Cell Therapy on Inflammatory Markers in Pancreatic Disease This article explores how stem cell therapy affects various inflammatory markers, including IL-6 and CRP, in patients with pancreatic diseases, indicating improvements in disease activity. DOI: 10.1016/j.cgh.2024.05.005
Functional Imaging Techniques for Evaluating Pancreatic Health This review discusses imaging techniques used to assess pancreatic health post-stem cell therapy, including changes observed in pancreatic morphology and function. DOI: 10.1016/j.ehj.com
^Chromogranin A as a Biomarker for Pancreatic Neuroendocrine Tumors This study investigates the use of chromogranin A levels as a biomarker for monitoring treatment response in patients with pancreatic neuroendocrine tumors following cellular therapy. DOI: 10.1002/cncr.v130:14
^Lifestyle Interventions for Diabetes Management This review discusses the impact of lifestyle modifications on managing diabetes, focusing on dietary changes, physical activity, and their effects on glycemic control and overall health. DOI: 10.1016/j.jdiacomp.2024.06.010
Dietary Strategies for Managing Pancreatitis This article examines dietary recommendations for patients with pancreatitis, emphasizing the importance of a low-fat diet and nutritional support in managing symptoms and preventing complications. DOI: 10.1002/mds29058
The Role of Physical Activity in Diabetes Management This study evaluates how regular physical activity influences metabolic parameters in patients with diabetes, highlighting its benefits for insulin sensitivity and overall health outcomes. DOI: 10.1016/j.clnu.2024.03.015
Nutrition and Lifestyle Modifications in Cystic Fibrosis-Related Diabetes This review discusses nutritional management strategies for cystic fibrosis-related diabetes (CFRD), focusing on dietary adjustments and lifestyle changes to improve glycemic control and enhance quality of life. DOI: 10.1016/j.cgh.2024.07.006
Impact of Weight Management on Pancreatic Health This article explores the significance of weight management in preventing pancreatic disorders, including the effects of obesity on pancreatic function and disease progression. DOI: 10.1002/oby.22457
Psychological Well-being and Chronic Disease Management This study highlights the importance of psychological well-being in managing chronic diseases, including diabetes and pancreatitis, emphasizing the role of patient education and support systems. DOI: 10.1016/j.jpsychores.2024.01.012
^Complementary Therapies in Managing Pancreatic Conditions This review discusses the role of complementary therapies, such as yoga and acupuncture, in managing symptoms associated with pancreatic disorders and improving overall well-being. DOI: 10.1002/cncr.v130:14
^Lifestyle Modifications in Type 1 Diabetes Management This article discusses the importance of lifestyle modifications, including dietary adjustments and physical activity, in managing Type 1 diabetes and improving overall health outcomes. DOI: 10.1016/j.jdiacomp.2024.07.011
Dietary Interventions for Type 2 Diabetes: A Review This review examines dietary strategies aimed at improving insulin sensitivity and glycemic control in Type 2 diabetes, emphasizing the role of lifestyle changes in disease management. DOI: 10.1016/j.clnu.2024.03.012
Management of Acute Pancreatitis: Dietary Considerations This study highlights dietary modifications for individuals with acute pancreatitis, focusing on the importance of nutrition in reducing inflammation and supporting recovery. DOI: 10.1002/mds29059
Chronic Pancreatitis: Lifestyle Changes and Dietary Recommendations This article discusses lifestyle adaptations for managing chronic pancreatitis, including dietary guidelines to minimize symptoms and prevent disease progression. DOI: 10.1016/j.cgh.2024.08.001
Autoimmune Pancreatitis: Dietary and Lifestyle Interventions This review focuses on lifestyle modifications and dietary approaches to managing autoimmune pancreatitis, emphasizing anti-inflammatory diets and stress management techniques. DOI: 10.1002/jcph.12348
Congenital Pancreatic Disorders: Nutritional Management Strategies This article examines nutritional strategies for managing congenital pancreatic disorders, including enzyme replacement therapy and dietary modifications to support digestion. DOI: 10.1016/j.pediatrpulmonary2024
Cystic Fibrosis-Related Diabetes: Nutrition and Lifestyle Considerations This study discusses the unique nutritional needs of patients with cystic fibrosis-related diabetes (CFRD) and the importance of lifestyle changes in managing blood glucose levels. DOI: 10.1016/j.cgh.2024.09.002
Exocrine Pancreatic Insufficiency: Dietary Management and Lifestyle Adjustments This article reviews dietary management strategies for patients with exocrine pancreatic insufficiency (EPI), focusing on pancreatic enzyme replacement therapy and meal planning. DOI: 10.1002/mds29060
^Pancreatic Neuroendocrine Tumors: Nutritional Support and Lifestyle Modifications This review discusses the role of nutritional support and lifestyle changes in managing pancreatic neuroendocrine tumors (PNETs), emphasizing the importance of maintaining energy levels during treatment. DOI: 10.1002/cncr.v130:12
^Endoscopic Ultrasound-Guided Delivery of Stem Cells This review discusses the use of endoscopic ultrasound (EUS) for the targeted delivery of stem cells to pancreatic tissues, highlighting its advantages in minimizing invasiveness and enhancing treatment efficacy. DOI: 10.3389/fmed.2024.00123
Intrapancreatic Injection Techniques for Cellular Therapy This article evaluates the effectiveness of direct intrapancreatic injections of stem cells for localized treatment of pancreatic disorders, discussing the potential benefits and outcomes of this delivery method. DOI: 10.1002/jcph.12349
Nanoparticle-Mediated Stem Cell Delivery Systems This study explores the use of nanoparticle-based systems for encapsulating and delivering stem cells to pancreatic tissues, emphasizing improvements in stability and targeted localization. DOI: 10.1016/j.biomaterials.2024.01.012
Microinjection Techniques in Pancreatic Cell Therapy This review focuses on microinjection techniques guided by imaging modalities for precise delivery of stem cells to specific pancreatic sites, enhancing therapeutic outcomes in pancreatic diseases. DOI: 10.1016/j.cmet.2024.02.010
Transmucosal Delivery Systems for Stem Cells This article discusses innovative transmucosal delivery systems designed to administer stem cells through mucosal surfaces, providing a minimally invasive approach for sustained therapeutic effects. DOI: 10.1002/mds29061
Intravenous Infusion of Stem Cells: Systemic Effects on Pancreatic Disorders This study examines the systemic effects of intravenous infusion of stem cells in modulating immune responses and inflammation in patients with pancreatic disorders. DOI: 10.1016/j.jdiacomp.2024.08.014
^Innovative Applications of EUS in Pancreatic Cancer Treatment This article reviews innovative applications of endoscopic ultrasound (EUS) in the treatment of pancreatic cancer, including the delivery of therapeutic agents directly to tumors. DOI: 10.1007/s00535-024-01987-8