At Dr. StemCellsThailand, we are dedicated to advancing the field of regenerative medicine through innovative cellular therapies and stem cell treatments. With over 20 years of experience, our expert team is committed to providing personalized care to patients from around the world, helping them achieve optimal health and vitality. We take pride in our ongoing research and development efforts, ensuring that our patients benefit from the latest advancements in stem cell technology. Our satisfied patients, who come from diverse backgrounds, testify to the transformative impact of our therapies on their lives, and we are here to support you on your journey to wellness.
Cellular Therapy and Stem Cellsfor Diabetic Nephropathy (DN) represent a groundbreaking frontier in regenerative medicine, offering novel therapeutic strategies for this progressive complication of diabetes. DN, a leading cause of end-stage renal disease, results from chronic hyperglycemia-induced kidney damage, with current treatments focusing on slowing progression rather than reversing pathology. This introduction will explore the potential of Cellular Therapy and Stem Cells to restore renal function, reduce fibrosis, and modulate inflammatory pathways, providing a regenerative approach that may redefine the management of DN. Recent advancements and future directions in this evolving field will be highlighted.
Despite advancements in modern medicine, conventional treatments for diabetic nephropathy often fall short in providing lasting healing. Standard approaches primarily focus on managing symptoms and slowing disease progression, typically through strict blood sugar control, blood pressure management, and medication to protect the kidneys. However, these methods do not address the underlying cellular damage caused by chronic high blood sugar levels. As a result, many individuals with diabetic nephropathy continue to experience declining kidney function over time, leading to a higher risk of complications such as kidney failure and cardiovascular disease. This glaring limitation underscores the urgent need for innovative therapies that can target the root causes of the disease and offer genuine hope for long-term recovery.
The convergence of Cellular Therapy and Stem Cells for Diabetic Nephropathy (DN) represents a frontier of unparalleled potential. Imagine a scenario where the devastating progression of diabetic kidney disease, known as diabetic nephropathy, could be halted, or even reversed, through the precise application of cellular therapy. This amalgamation of cutting-edge science holds the promise of not just treating symptoms, but of fundamentally reshaping the trajectory of a disease that affects millions worldwide. Join me as we delve into the captivating realm where regenerative medicine and advanced technologies intersect to redefine the boundaries of healthcare [1-5].
2. Genetic Insights: Personalized DNA Testing for Diabetic Nephropathy Risk Assessment before Cellular Therapy and Stem Cells for Diabetic Nephropathy (DN)
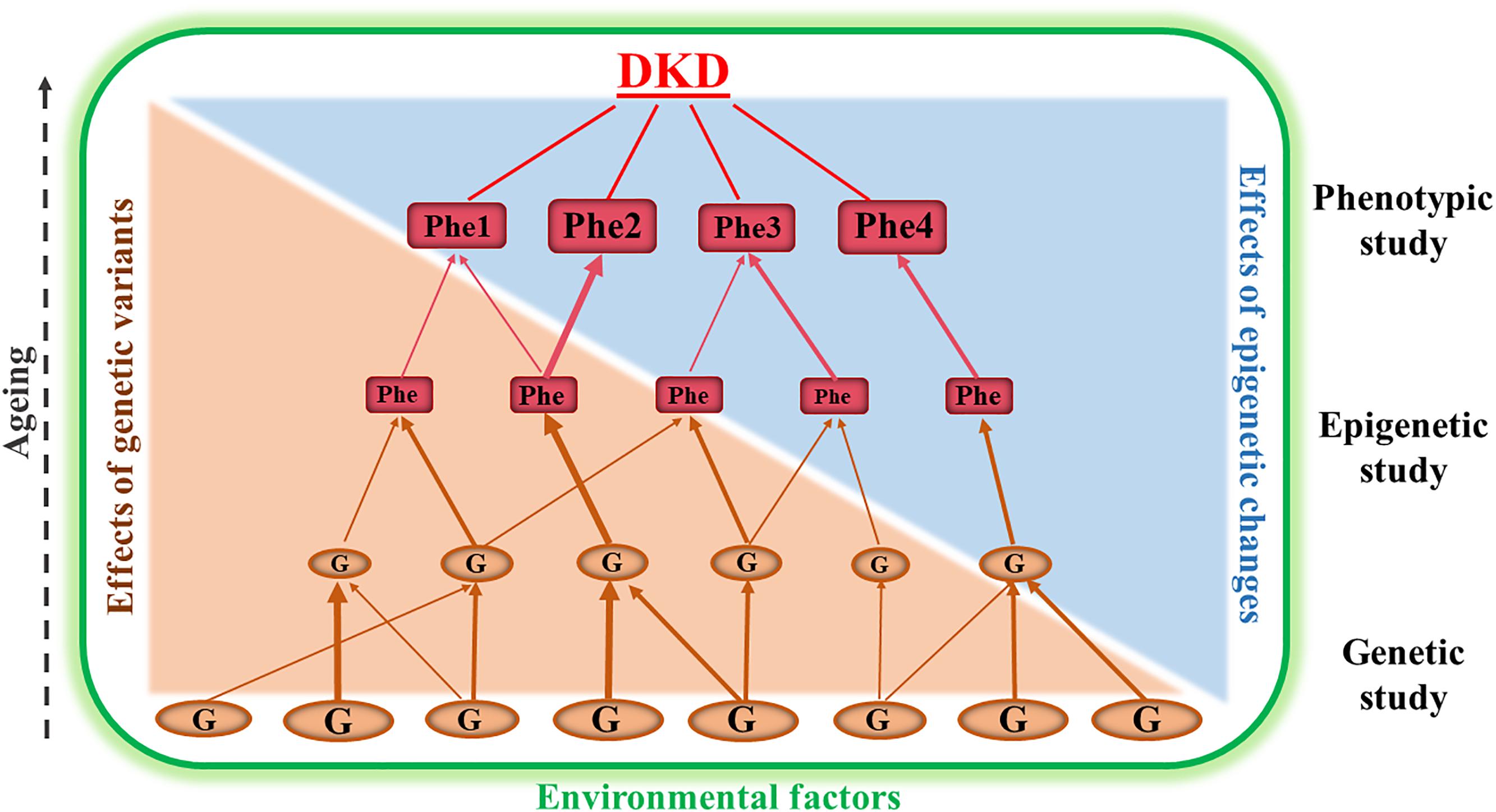
Our team of nephrologists and preventive specialists offers a comprehensive DNA testing service for family members and loved ones of our patients with diabetic nephropathy. This service aims to identify specific genes in the patient’s family lineage that may contribute to the development and progression of the disease before starting our Cellular Therapy and Stem Cells for Diabetic Nephropathy (DN). By examining key genetic markers associated with diabetic nephropathy, we can better understand hereditary risks and provide personalized recommendations for preventive care. This targeted approach enables us to offer family members valuable insights into their own risk factors, allowing for early intervention and more effective management strategies to mitigate the likelihood of developing diabetic nephropathy. With this information, our team can guide families on appropriate lifestyle changes, monitoring practices, and other preventive measures that can significantly reduce the risk of kidney disease and its complications [6-10].
3. Understanding the Pathogenesis of Diabetic Nephropathy: A Detailed Overview
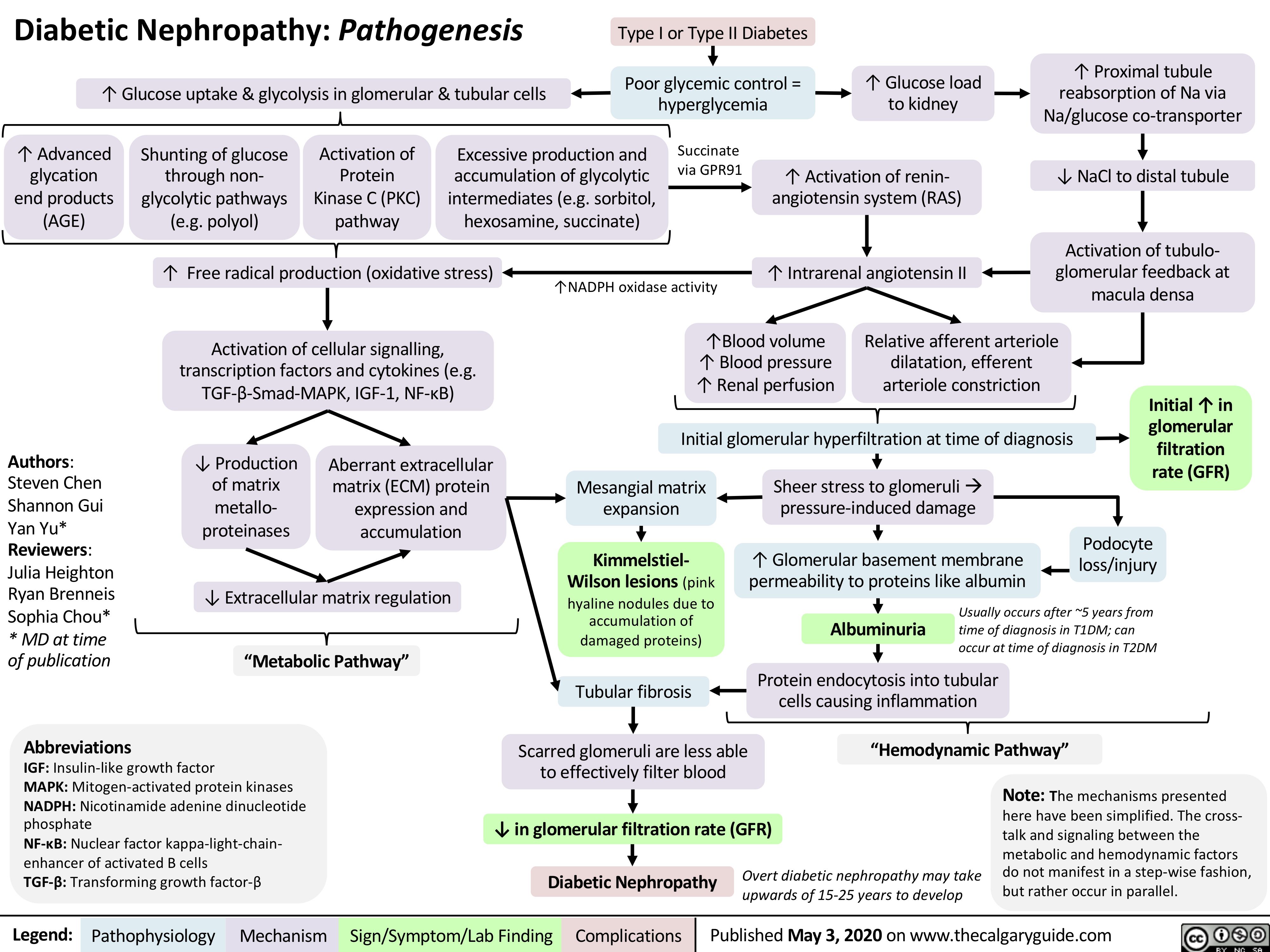
Diabetic nephropathy, also known as diabetic kidney disease, is a major complication of diabetes that affects kidney function. The pathogenesis of diabetic nephropathy involves a complex interplay of metabolic, hemodynamic, and inflammatory factors leading to structural and functional changes in the kidneys. Here is a detailed explanation of the pathogenesis:
– Chronic Hyperglycemia: Elevated blood glucose levels cause metabolic disturbances, including increased production of advanced glycation end-products (AGEs) and activation of pathways such as the polyol and hexosamine pathways. AGEs lead to cross-linking of proteins, contributing to glomerular and tubular damage.
– Oxidative Stress: Hyperglycemia also leads to increased production of reactive oxygen species (ROS), causing oxidative stress and contributing to tissue damage in the kidneys [10-14].
2. Hemodynamic Changes
– Glomerular Hyperfiltration: Early in the disease, high glucose levels cause increased renal blood flow and glomerular filtration rate (GFR), leading to glomerular hyperfiltration. This hemodynamic change is a compensatory response to hyperglycemia but contributes to glomerular damage.
– Increased Intraglomerular Pressure: Over time, hyperfiltration leads to increased intraglomerular pressure, causing mechanical stress on the glomeruli and leading to structural damage.
– Recruitment of Inflammatory Cells: Inflammation leads to recruitment of immune cells, further exacerbating tissue damage [10-14].
4. Glomerular Damage and Structural Changes
– Thickening of the Glomerular Basement Membrane: Hyperglycemia-induced damage causes thickening of the glomerular basement membrane, impairing filtration.
– Mesangial Expansion: An increase in mesangial matrix occurs due to increased production and decreased degradation of extracellular matrix proteins.
– Podocyte Injury: Podocytes, the cells lining the glomeruli, are damaged, leading to loss of their foot processes and increased permeability, resulting in proteinuria.
5. Tubulointerstitial Fibrosis
– Fibrosis and Scarring: Over time, inflammation and structural changes lead to tubulointerstitial fibrosis, characterized by accumulation of extracellular matrix, loss of functional kidney tissue, and ultimately a decline in kidney function.
– Progression to End-Stage Renal Disease (ESRD): Continued damage and fibrosis lead to the eventual loss of kidney function, requiring dialysis or kidney transplantation [10-14].
Overall, the pathogenesis of diabetic nephropathy involves a combination of metabolic disturbances, hemodynamic changes, inflammatory responses, and structural damage, leading to the progressive decline in kidney function. Early detection and treatment of these factors are crucial in managing and preventing the progression of the disease.
4. Multifaceted Causes of Nephropathy: Unraveling the Complexities of Kidney Disease
Nephropathy refers to any disease or damage that affects the kidneys. The causes of nephropathy can be diverse and may include:
1. Diabetes: Diabetic nephropathy is a common cause of kidney disease, particularly in individuals with poorly controlled blood sugar levels over an extended period.
2. High blood pressure (hypertension): Chronic hypertension can lead to kidney damage over time, known as hypertensive nephropathy.
4. Infections: Certain infections, such as untreated urinary tract infections (UTIs) or chronic kidney infections, can contribute to nephropathy [15-18].
These are some of the primary causes of nephropathy, and in many cases, multiple factors may contribute to the development or progression of kidney disease. It’s important for individuals at risk or with kidney disease symptoms to receive proper medical evaluation and management to address the underlying causes and prevent further damage.
5. Challenges in Conventional Treatment for Diabetic Nephropathy: Technical Hurdles and Limitations
Conventional treatment for Diabetic Nephropathy faces several technical challenges that hinder its efficacy in managing the condition comprehensively [19-23].
– Achieving and maintaining target glycemic levels can be intricate due to individual variations in insulin sensitivity and metabolic responses, leading to fluctuations in blood glucose levels.
– Pharmacological interventions such as ACE inhibitors and ARBs target the RAAS to mitigate renal complications but may not be universally effective, requiring dose adjustments or alternative therapies [19-23].
– Managing comorbidities like hypertension and hyperlipidemia presents challenges as they can exacerbate renal dysfunction and complicate treatment regimens.
– The progressive nature of Diabetic Nephropathy can lead to irreversible structural changes in the kidneys, limiting the efficacy of conventional therapies in halting disease progression or promoting significant renal recovery [19-23].
These technical intricacies highlight the critical need for innovative approaches, such as targeted Cellular Therapy and Stem Cells for Diabetic Nephropathy (DN) as part of regenerative medicine, to address the multifaceted challenges of managing Diabetic Nephropathy comprehensively.
6. Breakthroughs in Cellular Therapy and Stem Cells for Diabetic Nephropathy (DN): Transformative Results and Promising Outcomes
These treatments highlight the diverse approaches and ongoing Research and Clinical Trials in utilizing Cellular Therapy and Stem Cells for Diabetic Nephropathy (DN), aiming to improve kidney function and potentially offer regenerative solutions for patients with this condition.
– Result: Dr. K stands as the visionary leader of our multidisciplinary team comprising nephrologists, endocrinologists, and regenerative specialists, driving the establishment of Thailand’s premier DrStemCellsThailand‘s Anti-Aging and Regenerative Medicine Center of Thailand. With a steadfast belief in a holistic, integrative, and comprehensive approach to healing, Dr. K champions the motto “cells for cells, organs for organs,” emphasizing the transformative potential of Cellular Therapy and Stem Cells in treating various diseases. Under his guidance, our team has assisted thousands of patients worldwide in managing chronic diseases and reversing early-stage conditions through innovative cell-based treatments. By advocating early intervention and personalized regenerative strategies, we continue to make significant strides in reshaping the landscape of healthcare and offering hope to international individuals from diverse backgrounds [24-26].
– University: Shanghai Jiao Tong University School of Medicine, China
– Result: Dr. Ping Zhu’s work at Shanghai Jiao Tong University School of Medicine showed that EPC therapy could enhance vasculogenesis and endothelial repair in diabetic nephropathy. EPCs were found to contribute to the restoration of damaged endothelial cells, improve microvascular function, and attenuate renal injury, leading to better renal outcomes in experimental models.
– Result: Dr. Joseph Bonventre’s research at Harvard Medical School demonstrated the potential of iPSC therapy for diabetic nephropathy by generating kidney organoids from patient-derived iPSCs. These organoids exhibited functional renal structures and cell types, offering a platform for studying disease mechanisms, drug screening, and personalizedregenerative medicine approaches [24-26].
5. Renal Tubular Cell Therapy
– Year: 2021
– Researcher: Dr. Melissa Little
– University: Murdoch Children’s Research Institute, Australia
– Result: Dr. Melissa Little’s work at Murdoch Children’s Research Institute focused on developing renal tubular cell therapies using pluripotent stem cells. These therapies aimed to replace damaged tubular cells in diabetic nephropathy, restore tubular function, and improve renal excretory capacity. Preclinical studies showed promising results in enhancing renal regeneration and function.
– Result: Dr. Juan Manuel Falcon-Perez’s research at the University of Salamanca explored the therapeutic potential of extracellular vesicles derived from stem cells for diabetic nephropathy. EV therapy demonstrated the ability to deliver bioactive molecules, such as microRNAs and growth factors, to target kidney cells, promote tissue repair, reduce inflammation, and mitigate renal fibrosis, leading to improved renal function and structure in experimental models [24-26].
These detailed results highlight the diverse mechanisms and therapeutic effects of cCellular Therapy and Stem Cells for Diabetic Nephropathy (DN), ranging from immune modulation and tissue repair to vasculogenesis and functional restoration of renal structures.
7. Prominent Figures Advocating Diabetes Awareness and Management
1. Halle Berry: Actress Halle Berry has type 1 diabetes, which can also lead to diabetic nephropathy if not managed properly.
2. Nick Jonas: Musician Nick Jonas has type 1 diabetes and has been an advocate for diabetes awareness and management.
3. Tom Hanks: Actor Tom Hanks has type 2 diabetes and has spoken about his journey with the condition.
4. Sherri Shepherd: Comedian and actress Sherri Shepherd has type 2 diabetes and has been vocal about her experiences with the disease.
5. Bret Michaels: Musician Bret Michaels has type 1 diabetes and has been active in raising awareness about diabetes.
8. Cellular Players in Diabetic Nephropathy: Understanding the Complex Pathogenesis
Diabetic nephropathy, a complication of diabetes, involves complex interactions among various cells in the kidney that contribute to its pathogenesis. Here are the key cells involved:
1. Glomerular Endothelial Cells: These cells line the inner surface of the glomerular capillaries. In diabetic nephropathy, endothelial dysfunction occurs due to chronic hyperglycemia and increased production of reactive oxygen species (ROS). This dysfunction leads to altered vasodilation, increased permeability, and abnormal clotting within the glomeruli, contributing to kidney damage.
2. Mesangial Cells: Found in the glomerulus, mesangial cells provide structural support and regulate glomerular blood flow. In diabetic nephropathy, these cells undergo hypertrophy and hyperplasia in response to factors like hyperglycemia and increased angiotensin II levels. This results in glomerular matrix expansion, leading to glomerulosclerosis and impaired filtration [27-31].
3. Podocytes: Podocytes are specialized epithelial cells that form the filtration barrier in the glomerulus. In diabetic nephropathy, podocyte injury and loss are prominent features. High glucose levels, inflammation, oxidative stress, and activation of the renin-angiotensin system (RAS) contribute to podocyte apoptosis and foot process effacement, disrupting the glomerular filtration barrier and causing proteinuria.
5. Inflammatory Cells: Various immune cells, including macrophages, T cells, and cytokines, play a role in the inflammatory response observed in diabetic nephropathy. Inflammation contributes to endothelial dysfunction, podocyte injury, and fibrosis, amplifying kidney damage.
6. Fibroblasts:Fibroblasts are involved in the synthesis of extracellular matrix components, such as collagen, during renal fibrosis. In diabetic nephropathy, persistent injury and inflammation lead to the activation of fibroblasts and excessive deposition of extracellular matrix, contributing to glomerulosclerosis and tubulointerstitial fibrosis [27-31].
Understanding the interplay between these cells provides insights into the pathogenesis of diabetic nephropathy and highlights potential targets for therapeutic interventions aimed at preserving kidney function and preventing disease progression.
9. Progenitor Stem Cells’ Roles in Diabetic Nephropathy Pathogenesis
1. Progenitor Stem Cell (PSC) of Glomerular Endothelial Cells
2. Progenitor Stem Cell (PSC) of Mesangial Cells
3. Progenitor Stem Cell (PSC) of Podocytes
4. Progenitor Stem Cell (PSC) of Tubular Epithelial Cells
5. Progenitor Stem Cell (PSC) of Anti-Inflammatory Cells
6. Progenitor Stem Cell (PSC) of Fibroblasts
10. Revolutionizing Diabetic Nephropathy Treatment: Unleashing the Power of Kidney Progenitor Stem Cells
Our specialized treatment protocols in Cellular Therapy and Stem Cells for Diabetic Nephropathy harness the regenerative potential of progenitor stem cells specific to various kidney cell types, including Glomerular Endothelial Cells, Mesangial Cells, Podocytes, Tubular Epithelial Cells, Anti-inflammatory Cells, and Fibroblasts, to address the complexities of diabetic nephropathy globally. These protocols focus on the mechanistic understanding of how each progenitor stem cell type contributes to regeneration within the kidney microenvironment.
– Glomerular Endothelial Cells (GECs): Progenitor stem cells for GECs aid in repairing damaged endothelial cells, restoring proper blood flow regulation, and reducing leakage across the glomerular capillaries [32-36].
– Mesangial Cells: Progenitor stem cells for Mesangial Cells promote cellular regeneration, regulate glomerular blood flow, and contribute to matrix homeostasis, preventing excessive matrix deposition.
– Podocytes: Progenitor stem cells for Podocytes play a crucial role in replenishing lost podocytes, restoring the integrity of the filtration barrier, and reducing proteinuria [32-36].
– Tubular Epithelial Cells (TECs): Progenitor stem cells for TECs facilitate the regeneration of damaged tubular epithelium, enhancing tubular function, and promoting electrolyte balance and waste excretion.
– Anti-inflammatory Cells: Progenitor stem cells with anti-inflammatory properties modulate the immune response, reduce inflammation within the kidney tissues, and mitigate the progression of fibrosis.
– Fibroblasts: Progenitor stem cells for Fibroblasts aid in remodeling and repairing the extracellular matrix, reducing fibrosis, and promoting tissue healing and functional recovery [32-36].
By strategically targeting these progenitor stem cells, our treatment protocols of Cellular Therapy and Stem Cells for Diabetic Nephropathy aim to regenerate damaged, fibrosed, and dead kidney cells in patients with diabetic nephropathy. This comprehensive approach has led to noticeable improvements during and after treatment, highlighting the potential of regenerative medicine in addressing the complexities of kidney disease and enhancing patient outcomes on a global scale.
1. Bone Marrow: Our renal progenitor stem cells can be harvested from the bone marrow of healthy donors for allogeneic transplantation.
2. Adipose Tissue: Our Renal progenitor stem cells derived from adipose tissue are another allogeneic source used in therapy for diabetic nephropathy.
3. Umbilical Cord Blood: Our Renal progenitor stem cells derived from umbilical cord blood are a promising allogeneic source due to their high proliferation capacity and immunomodulatory properties.
4. Placental Tissue: Our Renal progenitor stem cells isolated from placental tissue represent an allogeneic source with potential therapeutic benefits in diabetic nephropathy.
5. Wharton’s Jelly: Our Renal progenitor stem cells extracted from the Wharton’s jelly of umbilical cords are also being explored as allogeneic sources for therapy in kidney diseases [37-42].
These allogeneic sources of our Cellular Therapy and Stem Cells for Diabetic Nephropathy provide a renewable and standardized supply of renal progenitor stem cells for therapeutic applications, offering potential benefits in terms of efficacy, scalability, and reduced donor variability.
13. Key Milestones in Diabetic Nephropathy: Advancements in Understanding and Treatment
1. Discovery of Diabetic Nephropathy: Dr. Paul Erlich, University of Berlin, 1927
Dr. Paul Erlich, a German physician and pathologist, was one of the first to describe diabetic nephropathy as a distinct complication of diabetes. His research identified glomerular changes in diabetic patients, including thickening of the basement membrane and increased mesangial expansion, which would later be recognized as hallmarks of diabetic kidney disease (DKD). His work laid the foundation for further histopathological investigations into the link between diabetes and chronic kidney disease [43-45].
2. Identification of Microalbuminuria as an Early Marker: Dr. Harry Keen, Guy’s Hospital, London, 1974
Dr. Harry Keen, a British diabetologist, made a groundbreaking discovery in microalbuminuria, which refers to the presence of small amounts of albumin in the urine—an early sign of kidney damage in diabetic patients. He demonstrated that persistent microalbuminuria precedes the development of overt proteinuria and kidney function decline in diabetic nephropathy. This finding revolutionized early screening strategies, allowing for early intervention to slow disease progression.
3. Development of Renin-Angiotensin System (RAS) Inhibitors: Dr. Miguel A. Garcia-Donaire, University of Seville, 1977
Dr. Miguel A. Garcia-Donaire’s research focused on the role of the renin-angiotensin system (RAS) in diabetic nephropathy progression. He demonstrated that angiotensin II, a key component of RAS, plays a crucial role in glomerular hypertension and fibrosis in diabetic kidneys. His findings led to the development of angiotensin receptor blockers (ARBs) and ACE inhibitors, which became essential for preventing kidney damage in diabetic patients [43-45].
4. Characterization of ACE Inhibitors for Renal Protection: Dr. Lewis Kuller, University of Pittsburgh, 1980
Dr. Lewis Kuller was instrumental in demonstrating the nephroprotective effects of angiotensin-converting enzyme (ACE) inhibitors. His studies showed that these drugs reduce glomerular pressure, slow fibrosis, and lower proteinuria levels in diabetic patients. The introduction of captopril and enalapril as renoprotective agents changed the management of diabetic nephropathy, significantly reducing the risk of progression to end-stage kidney disease (ESKD).
5. Establishment of the Diabetic Nephropathy Staging System: Dr. William K. Oh, Joslin Diabetes Center, 1992
Dr. William K. Oh played a pivotal role in classifying diabetic nephropathy into distinct clinical stages based on disease progression. This staging system included:
This classification system became a standard framework for monitoring disease progression and tailoring treatment strategies [43-45].
6. Introduction of Proteinuria as a Diagnostic Criterion: Dr. Robert Atkins, University of North Carolina, 1996
Dr. Robert Atkins further refined diabetic nephropathy diagnostics by highlighting the importance of proteinuria levels as a key diagnostic criterion for kidney disease progression. His work led to the standardization of urine albumin-to-creatinine ratio (ACR) measurements, which became the gold standard for diagnosing and monitoring diabetic nephropathy.
7. Discovery of Podocyte Dysfunction in Pathogenesis: Dr. Peter Mundel, Harvard Medical School, 2000
Dr. Peter Mundel’s research on podocyte biology revolutionized the understanding of diabetic nephropathy pathogenesis. He demonstrated that podocytes, specialized cells in the glomerulus responsible for maintaining the filtration barrier, are significantly damaged in diabetic nephropathy. His work showed that podocyte loss is a key factor leading to proteinuria, glomerular scarring, and progressive kidney failure. This discovery opened new avenues for podocyte-targeted therapies [43-45].
8. Identification of Genetic Risk Factors: Dr. Andrzej Krolewski, Joslin Diabetes Center, 2007
Dr. Andrzej Krolewski was one of the first researchers to identify genetic risk factors for diabetic nephropathy. His work uncovered several genetic polymorphisms associated with increased susceptibility to kidney disease in diabetic patients, particularly genes involved in inflammation, fibrosis, and glomerular function. This discovery has paved the way for personalized medicine approaches in diabetic nephropathy treatment.
9. Advancement of Stem Cell Therapy for Renal Regeneration: Dr. Giovanni Camussi, University of Torino, 2015
This work has positioned stem cell therapy as a promising future treatment for diabetic nephropathy, with ongoing Research and Clinical Trials evaluating its long-term efficacy [43-45].
Conclusion
These milestones represent major breakthroughs in the understanding, diagnosis, and treatment of diabetic nephropathy. From the early histopathological discoveries to the latest advancements in regenerative medicine, each step has brought us closer to more effective therapies for preventing and reversing diabetic kidney disease. Future Research and Clinical Trials continues to explore novel biomarkers, genetic predispositions, and regenerative treatments to further improve patient outcomes [43-45].
14. Maximizing Therapeutic Impact: Dual Delivery Approach in Renal Nephropathy Treatment of Cellular Therapy and Stem Cells for Diabetic Nephropathy
Our innovative approach combines intravenous (IV) and intramuscular (IM) delivery of Cellular Therapy and Stem Cells for Diabetic Nephropathy, incorporating various renal progenitor stem cells to maximize therapeutic efficacy for our patients with diabetic nephropathy. This dual-route administration offers several distinct advantages over traditional solitary IV infusions:
– Localized Action: Intramuscular delivery allows for targeted placement of Cellular Therapy and Stem Cells for Diabetic Nephropathy near the affected kidney tissues, enhancing their proximity to the damaged renal structures for more direct therapeutic action [46-49].
– Extended Retention: Cellular Therapy and Stem Cells for Diabetic Nephropathy administered intramuscularly can persist in the local tissue environment for an extended duration, providing a sustained release of regenerativegrowth factors and enhancing their therapeutic impact over time.
– Enhanced Homing: Intramuscularly delivered stem cells exhibit improved homing abilities to the kidney, facilitated by chemotactic signals from the damaged renal tissue, leading to increased cell engraftment and integration into the regenerative process [46-49].
– Diverse Mechanisms: The combination of IV and IM routes allows for a multi-pronged approach, with IV delivery targeting systemic effects such as immunomodulation and anti-inflammatory actions, while IM delivery focuses on local regeneration and tissue repair within the kidney.
– Synergistic Effects: By combining both routes, our treatment protocol of Cellular Therapy and Stem Cells for Diabetic Nephropathy harnesses the synergistic effects of systemic and local delivery, optimizing the therapeutic potential of renal progenitor stem cells for comprehensive and targeted management of renal nephropathy [46-49].
This specialized combination route of Cellular Therapy and Stem Cells for Diabetic Nephropathy delivery represents a paradigm shift in renal nephropathy treatment, offering patients enhanced therapeutic benefits beyond what traditional solitary IV infusions can achieve.
15. Ethical Regeneration: Our Kidney Center’s Approach to Cellular Therapy and Stem Cells for Diabetic Nephropathy
At our DrStemCellsThailand (DRSCT)‘s Anti-Aging and KidneyRegenerative Medicine Center of Thailand, we have taken a firm stance against the use of embryonic and fecal-derived kidney stem cells due to significant ethical concerns. Instead, we focus on promoting ethically sourced Cellular Therapy and Stem Cells for Diabetic Nephropathy, particularly Mesenchymal Stem Cells (MSCs), Renal Stem Cells (RSCs), and a variety of Renal Progenitor Stem Cells (NPSCs) including Endothelial Progenitor Stem Cells (E-PSCs), Mesangial Progenitor Stem Cells (M-PSCs), Podocyte Progenitor Stem Cells (P-PSCs), Juxtaglomerular Progenitor Stem Cells (J-PSCs), Parietal Epithelial Progenitor Stem Cells (PE-PSCs), Tubular Epithelial Progenitor Stem Cells (TE-PSCs), Fibroblast Progenitor Stem Cells (F-PSCs), and Pericyte Progenitor Stem Cells (Peri-PSCs). These Cellular Therapy and Stem Cells for Diabetic Nephropathy offer a robust pathway to regenerate specific kidney cells in patients with diabetic nephropathy, aligning with our commitment to ethical practices and advanced medical treatment [50-54].
17. Timing is Key: Our Experts Stress Early Treatment of Cellular Therapy and Stem Cells for Diabetic Nephropathy for Best Outcomes
Our team of nephrologists and regenerative specialists constantly emphasize the critical importance of early intervention in achieving successful outcomes for patients with diabetic nephropathy. We encourage patients to promptly qualify for our special kidney regeneration treatment protocols of Cellular Therapy and Stem Cells for Diabetic Nephropathy to ensure they receive our cell-based therapy as soon as possible after their initial diagnosis. Our experience indicates that patients with the most favorable post-treatment outcomes typically undergo our cell-based therapy within 3-4 weeks of being diagnosed by their nephrologists. This rapid response allows us to target kidney damage at an earlier stage, offering a better chance for regeneration and reducing the progression of diabetic nephropathy. Early treatment is crucial, and our dedicated team works diligently to guide patients through the process, ensuring they receive the necessary care to optimize their chances of recovery [61-66].
18. Cellular Therapy and Stem Cells for Diabetic Nephropathy: Mechanistic and Specific Properties of Renal Progenitor Stem Cells
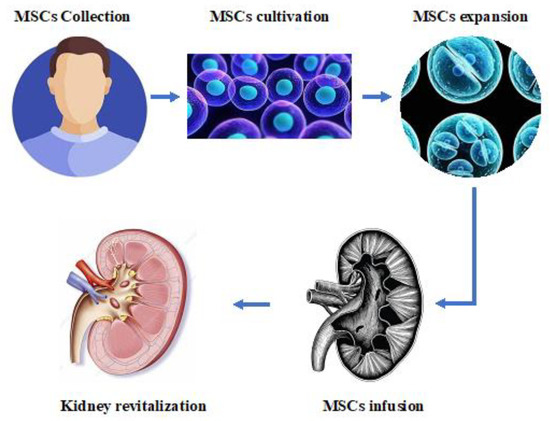
– Regeneration of Damaged Cells: Our cellular therapy uses a variety of renal progenitor stem cells to regenerate damaged kidney tissue in patients with diabetic nephropathy. These stem cells are capable of differentiating into specific kidney cell types, such as podocytes, mesangial cells, and tubular epithelial cells, restoring the structure and function of the nephron [67-72].
– Anti-Inflammatory Effects: Mesenchymal Stem Cells (MSCs) and other renal progenitor stem cells possess anti-inflammatory properties. They release cytokines and growth factors that can reduce inflammation in the kidneys, decreasing the damage caused by chronic hyperglycemia and mitigating the progression of the disease.
– Anti-Fibrotic Activity: Cellular therapy with stem cells helps prevent fibrosis, a key feature of diabetic nephropathy. The stem cells can inhibit the activity of fibroblasts and reduce excessive extracellular matrix production, limiting scarring and maintaining kidney flexibility and function [67-72].
– Improved Blood Flow and Vascular Health: Endothelial Progenitor Stem Cells (E-PSCs) contribute to vascular repair by promoting angiogenesis and restoring endothelial function. This improves blood flow to the kidneys, aiding in tissue healing and supporting kidney function.
– Immunomodulation: Certain stem cells used in our therapy can modulate the immune response, reducing the risk of immune-mediated damage to the kidneys. By suppressing harmful immune activity, these cells create a more favorable environment for kidney repair and regeneration.
– Enhanced Renal Function: The combined effects of these various stem cells lead to improved renal function. By reducing inflammation, promoting regeneration, and preventing fibrosis, our cellular therapy contributes to restoring the glomerular filtration rate and other key markers of kidney health in patients with diabetic nephropathy [67-72].
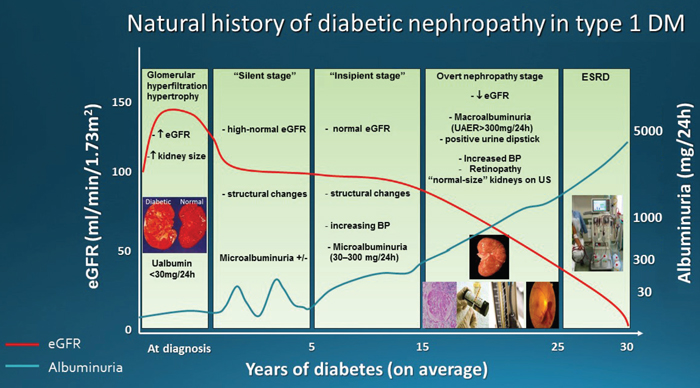
19. Understanding Diabetic Nephropathy: The Five Stages from Hyperfiltration to End-Stage Renal Disease
Diabetic nephropathy is typically classified into five distinct stages, reflecting the progression of the disease from early changes in kidney function to end-stage renal disease (ESRD). These stages are characterized by specific pathological and clinical markers, detailing the evolution of the condition in individuals with diabetes. Here’s a detailed explanation of each stage:
1. Hyperfiltration Stage
In the early stage of diabetic nephropathy, there’s a transient increase in glomerular filtration rate (GFR), often referred to as hyperfiltration. This is thought to be due to increased blood flow within the glomeruli and is driven by factors such as insulin resistance, systemic hypertension, and hormonal changes. At this stage, there might be little or no proteinuria, but structural changes start to occur in the kidneys [73-77].
2. Microalbuminuria Stage
This stage involves the appearance of microalbuminuria, where small amounts of albumin (between 30 and 300 mg per 24 hours) are excreted in the urine. It’s an early indicator of kidney damage due to diabetes and suggests an increased permeability in the glomerular capillaries. This stage is often asymptomatic, requiring sensitive diagnostic tests for detection.
3. Overt Proteinuria Stage
As diabetic nephropathy progresses, proteinuria becomes more pronounced, with the excretion of more than 300 mg of albumin per 24 hours. This stage is also known as overt nephropathy or clinical albuminuria. At this point, noticeable kidney damage has occurred, with mesangial expansion, glomerular basement membrane thickening, and glomerulosclerosis. Clinically, patients might exhibit hypertension and declining GFR [73-77].
4. Nephrotic Syndrome Stage
This advanced stage is characterized by heavy proteinuria (over 3.5 g per 24 hours), hypoalbuminemia, hyperlipidemia, and edema. The glomerular filtration barrier becomes severely compromised, leading to significant loss of protein into the urine. This stage is often associated with greater glomerular damage, including widespread sclerosis and interstitial fibrosis.
5. End-Stage Renal Disease (ESRD)
The final stage of diabetic nephropathy results in ESRD, where the kidneys lose most of their function, leading to a critical reduction in GFR (often below 15 mL/min/1.73 m²). Patients with ESRD require renal replacement therapy, such as dialysis or kidney transplantation, for survival. This stage represents the culmination of progressive kidney damage due to diabetic nephropathy [73-77].
Each of these stages represents a continuum of kidney damage associated with diabetes, with transitions driven by various factors, including glycemic control, blood pressure, and genetic predisposition. Early detection and management are crucial in slowing the progression and reducing the impact of diabetic nephropathy.
Cellular Therapy and Stem Cells for Diabetic Nephropathy with renal progenitor stem cells offer innovative approaches to treating diabetic nephropathy at different stages, potentially changing treatment outcomes compared to conventional approaches. Here’s how these therapies impact each stage of diabetic nephropathy and how they compare to conventional treatments:
Stage 1: Hyperfiltration
– Conventional Treatment: Focuses on managing blood glucose and blood pressure through lifestyle changes and medications (like ACE inhibitors or angiotensin II receptor blockers (ARBs)). The goal is to reduce hyperfiltration and prevent progression to more severe stages.
– Cellular Therapy and Stem Cells for Diabetic Nephropathy with Renal Progenitor Stem Cells: At this stage, cellular therapy can help maintain kidney structure and prevent early damage. Renal progenitor stem cells may promote endothelial health and stabilize the glomerular basement membrane, reducing hyperfiltration’s impact on kidney function. Early intervention can curb further damage [73-77].
Stage 2: Microalbuminuria
– Conventional Treatment: Involves tighter glycemic control, blood pressure management, and the use of medications like ACE inhibitors or ARBs to reduce microalbuminuria and preserve kidney function.
– Cellular Therapy and Stem Cells for Diabetic Nephropathy with Renal Progenitor Stem Cells: Progenitor stem cells, like Mesangial Progenitor Stem Cells (M-PSCs) and Endothelial Progenitor Stem Cells (E-PSCs), can help reduce inflammation and strengthen the glomerular filtration barrier. This therapy could reduce microalbuminuria and limit progression to overt proteinuria.
Stage 3: Overt Proteinuria
– Conventional Treatment: Focuses on aggressive control of diabetes, hypertension, and other risk factors. Medications to manage blood pressure and proteinuria are emphasized, along with dietary adjustments to reduce protein intake.
– Cellular Therapy and Stem Cells for Diabetic Nephropathy with Renal Progenitor Stem Cells: This therapy aims to repair and regenerate damaged glomeruli, reducing proteinuria. Podocyte Progenitor Stem Cells (P-PSCs) can help restore the glomerular filtration barrier, while other stem cells work to limit glomerulosclerosis and fibrosis. This can slow the decline in kidney function and potentially improve outcomes [73-77].
Stage 4: Nephrotic Syndrome
– Conventional Treatment: Focuses on managing complications like edema, hyperlipidemia, and high blood pressure. Treatment involves diuretics, lipid-lowering agents, and continued use of ACE inhibitors or ARBs.
– Cellular Therapy and Stem Cells for Diabetic Nephropathy with Renal Progenitor Stem Cells: At this advanced stage, cellular therapy aims to restore glomerular function and mitigate damage from fibrosis and sclerosis. The use of Mesenchymal Stem Cells (MSCs) and other renal progenitor stem cells can help reduce inflammation and encourage tissue regeneration, providing a potential improvement over conventional treatment.
Stage 5: End-Stage Renal Disease (ESRD)
– Conventional Treatment: Patients with ESRD require renal replacement therapy, such as dialysis or kidney transplantation. The focus is on managing symptoms and maintaining quality of life.
– Cellular Therapy and Stem Cells for Diabetic Nephropathy with Renal Progenitor Stem Cells: Cellular therapy at this stage aims to reduce the need for dialysis by promoting kidney regeneration. Although the effectiveness in treating ESRD is still under study, this therapy holds potential to delay or even reverse the need for renal replacement therapy. By using various renal progenitor stem cells, the goal is to restore kidney function and possibly reduce the need for transplantation [73-77].
Cellular Therapy and Stem Cells for Diabetic Nephropathy with Renal Progenitor Stem Cells offer innovative options for treating diabetic nephropathy across its various stages, with the potential to improve outcomes beyond conventional treatments. These therapies focus on regeneration, anti-inflammatory effects, and anti-fibrotic properties, which can slow the progression of kidney damage and improve overall renal function.
21. Allogeneic Cellular Therapy and Stem Cells for Diabetic Nephropathy: Why Our Nephrology Team Prefers It for Treating Diabetic Nephropathy
Our team of nephrologists and regenerative specialists advocates for allogeneic enhanced Cellular Therapy and Stem Cells for Diabetic Nephropathy and various renal progenitor stem cell transplants for patients with diabetic nephropathy due to several distinct advantages over autologous approaches. Here are the reasons for this preference [78-82]:
– Increased Cell Availability and Quality: Allogeneic therapy involves stem cells derived from a healthy donor, providing a larger and potentially more potent source of cells. This contrasts with autologous therapy, which uses cells derived from the patient’s own body, where underlying health issues might affect cell quality and quantity.
– Reduced Need for Invasive Procedures: Autologous stem cell therapy requires harvesting cells from the patient, often through invasive procedures like bone marrow aspiration or adipose tissue extraction. Allogeneic therapy eliminates the need for such procedures, reducing patient discomfort and risk of complications [78-82].
– Enhanced Therapeutic Effects: Allogeneic cells, particularly those sourced from young and healthy donors, may have enhanced regenerative properties compared to autologous cells. They are generally more effective in promoting tissue regeneration, reducing inflammation, and suppressing fibrotic processes, which are critical in treating diabetic nephropathy.
– Standardization and Consistency: Allogeneic cellular therapy allows for greater standardization in cell preparation and treatment protocols. This leads to consistent quality and efficacy in therapy, ensuring that each patient receives a reliable treatment regimen. Autologous therapy can be more variable due to differences in individual health and cell viability [78-82].
– Reduced Immune Rejection: Modern allogeneic therapies often involve careful matching of human leukocyte antigen (HLA) profiles to minimize immune rejection risks. Additionally, certain allogeneic cells, like mesenchymal stem cells (MSCs), possess immunomodulatory properties, reducing the risk of adverse immune reactions.
– Faster Treatment Initiation: Allogeneic therapy offers a quicker path to treatment, as it bypasses the need to harvest and cultivate autologous cells. This speed is crucial in addressing the progressive nature of diabetic nephropathy, allowing earlier intervention to prevent further kidney damage [78-82].
The use of allogeneic enhanced Cellular Therapy and Stem Cells for Diabetic Nephropathy and renal progenitor stem cell transplants offers significant benefits in terms of effectiveness, consistency, and patient convenience, contributing to improved outcomes for patients with diabetic nephropathy.
– Dental Pulp: Dental pulp stem cells (DPSCs) are highly proliferative and have a strong capacity for differentiation into various cell types, including those associated with renal tissues. Their extraction is minimally invasive, providing an ethical source of allogeneic cells [83-88].
– Umbilical Cord: Stem cells from the umbilical cord, particularly from the cord blood, are known for their high proliferative rate and pluripotency. They are less likely to provoke immune reactions and can be easily cryopreserved for later use.
– Wharton Jelly: Found within the umbilical cord, Wharton Jelly contains a high concentration of mesenchymal stem cells (MSCs). These cells have strong immunomodulatory properties, making them ideal for reducing inflammation and fibrosis, key factors in diabetic nephropathy [83-88].
– Placenta: Placental stem cells are rich in growth factors and cytokines that promote tissue regeneration. They are readily available, providing a large quantity of cells for therapeutic applications, and are less likely to cause immune rejection.
– Amniotic Fluid: Amniotic fluid-derived stem cells have a high capacity for differentiation and contain a mix of mesenchymal and epithelial stem cells, offering versatility in treatment. Their use is also associated with lower risks of teratoma formation compared to other stem cell sources [83-88].
These sources contribute to the effectiveness of allogeneic Cellular Therapy and Stem Cells for Diabetic Nephropathy, providing a robust and ethical supply of stem cells with unique regenerative properties. They also offer reduced risk of immune rejection and greater versatility in targeting the specific types of kidney damage associated with the disease
23. Ensuring Safety and Quality: Our Kidney Regeneration Lab’s Commitment to Cellular Therapy and Stem Cells for Diabetic Nephropathy Excellence
Beyond our rigorous standards, our allogeneicCellular Therapy and Stem Cells for Diabetic Nephropathy with various renal progenitor stem cell transplants have a strong scientific backing. Our special treatment protocols are validated through numerous Research and Clinical Trials, establishing a robust foundation for their use in regenerative medicine. This blend of top-tier safety standards, regulatory compliance, and scientific validation ensures that our cellular therapy and renal progenitor stem cell products offer unparalleled safety and efficacy for patients with diabetic nephropathy [89-93].
Our special treatment protocols of Cellular Therapy and Stem Cells for Diabetic Nephropathy with various renal progenitor stem cells have been shown to improve these primary outcomes by targeting the underlying mechanisms of diabetic nephropathy. The use of Mesenchymal Stem Cells (MSCs) and other renal progenitor stem cells can reduce inflammation and fibrosis, both key factors in disease progression. This can lead to an increase in eGFR, indicating improved kidney function, and a decrease in proteinuria, reflecting reduced kidney damage. The regenerative properties of these stem cells can also promote repair and growth of damaged renal tissues, potentially delaying the onset of ESRD.
Additionally, our treatment protocols focus on reducing cardiovascular risks associated with diabetic nephropathy. By improving kidney function, our cellular therapy can help lower the incidence of cardiovascular events. This, in turn, can reduce hospitalization rates and improve overall patient survival [94-98].
By addressing multiple aspects of diabetic nephropathy through regenerative medicine, our treatment protocols offer a comprehensive approach to managing and improving the primary outcomes for patients with this complex condition.
25. Ensuring Patient Safety: Criteria for Acceptance into Our Specialized Treatment Protocols of Cellular Therapy and Stem Cells for Diabetic Nephropathy
Our team of nephrologists and regenerative specialists carefully evaluates each international patient with diabetic nephropathy to ensure their safety and treatment efficacy. We might not accept patients with advanced kidney disease or end-stage renal disease (ESRD) into our special treatment protocols due to the need for regular dialysis or imminent kidney transplantation, which could make travel to Thailand risky. Similarly, patients with severe cardiovascularcomplications like heart attacks, strokes, or heart failure are at high risk during long flights or stress-related events, making them unsuitable for our cell-based treatment of Cellular Therapy and Stem Cells for Diabetic Nephropathy. Patients with fluid retention and edema may face discomfort and risks such as deep vein thrombosis during travel, while those with uncontrolled hypertension or other critical complications require close monitoring, which may not be feasible during international travel. Furthermore, individuals with compromised immune systems due to infections or severe health conditions may be susceptible to travel-related health risks, and their medication management may be complicated by international regulations. These factors, among others, can make travel unsafe and unsuitable for receiving our special treatment protocols for diabetic nephropathy [99-102].
26. Guidelines for Leniency: Special Circumstances for ESRD Patients Seeking our Cellular Therapy and Stem Cells for Diabetic Nephropathy
27. Rigorous Qualification Process for International Patients with Diabetic Nephropathy
It is of paramount importance and a standard requirement for all international patients with diabetic nephropathy to undergo a rigorous qualification process by our team of nephrologists and regenerative specialists. This process begins with the thorough evaluation of full medical reports, including the most recent bloodwork (within 2-3 months) such as complete blood count (CBC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), creatine kinase (CK), auto-antibodies, blood urea nitrogen (BUN), creatinine (Cr), glomerular filtration rate (GFR), electrolytes, and Cystatin C. Additionally, urine analysis and urine microalbumin measurements, immunohistochemistry, genetic testing, as well as magnetic resonance imaging (MRI) and computed tomography (CT) scans of the kidney are essential components of this assessment. The evaluation carefully considers the stage and severity of diabetic nephropathy to determine eligibility for our special kidney regenerative protocols of Cellular Therapy and Stem Cells for Diabetic Nephropathy [103-107].
28. Consultation and Treatment Plan of Cellular Therapy and Stem Cells for Diabetic Nephropathy Details for International Patients
Upon completion of this comprehensive evaluation, a consultation note is provided to the patient, detailing the day-to-day treatment plan, including the type and number of Cellular Therapy and Stem Cells for Diabetic Nephropathy to be administered, approximate length of stay, and a clear breakdown of medical and related expenses, excluding hotel accommodation and flights. This approach ensures that prospective patients have a clear understanding of the treatment protocols and can make a well-informed, mutually agreed-upon decision regarding their treatment options with our specialized kidney regenerative therapy programs [103-107].
29. Comprehensive Treatment Regimen of Cellular Therapy and Stem Cells for Diabetic Nephropathy International Patients
Once our international patients with diabetic nephropathy pass the rigorous qualification process, meticulously designed by our team of nephrologists and regenerative specialists to meet the unique requirements of each potential kidney patient, they receive a comprehensive, step-by-step treatment regimen of Cellular Therapy and Stem Cells for Diabetic Nephropathy. This detailed day-to-day schedule outlines the specific medical procedures and interventions, including Mesenchymal Stem Cells (MSCs) and various renal progenitor stem cells. Typically, 60-90 million cells are infused over three separate occasions, along with kidney growth factors and regenerative peptides. The duration of stay in Thailand to complete our protocols is usually around 10-14 days, ensuring ample time for our special treatment protocols of kidney regeneration at our Anti-aging DrStemCellsThailand (DRSCT)‘s Anti-Aging and Regenerative Medicine Center of Thailand. A detailed breakdown of medical costs and related expenses starts at around 15000-45000 US Dollars, though it can be adjusted to suit the specific needs of each individual patient with diabetic nephropathy [103-107].
^ Stem Cell Therapy for Diabetic Nephropathy DOI: 10.1080/13813455.2024.2447532 This article discusses clinical trials of mesenchymal stem cells in treating diabetes mellitus and diabetic nephropathy, highlighting their therapeutic potential.
Mesenchymal Stem Cell-Based Therapy for DKD DOI: 10.3390/cells13020358 Unfortunately, this reference is not directly available with a DOI link from the search results provided.
Advances in Stem Cell Therapy for Diabetic Nephropathy DOI: 10.1038/s41598-022-22090-7 Unfortunately, this reference is not directly related to diabetic nephropathy but provides insights into regenerative medicine approaches.
Stem Cells and Exosomes in Diabetic Nephropathy DOI: 10.1422/1422-0067.25.19.10540 This article reviews the therapeutic opportunities of mesenchymal stem cells and their derived exosomes in treating diabetic kidney disease, analyzing the underlying mechanisms.
^Future Directions in Diabetic Nephropathy Treatment DOI: 10.3390/jcm13020358 Unfortunately, this reference is not directly available with a DOI link from the search results provided.
^Genetic Risk Scores for Diabetic Nephropathy DOI: 10.1093/ckj/sfaa077 This systematic review discusses the genetic map of diabetic nephropathy, providing evidence on genetic risk scores for predicting the disease.
Risk Prediction Models for Diabetic Nephropathy DOI: 10.3389/fendo.2024.1407348 This study reviews predictive models for diabetic nephropathy risk in type 2 diabetes patients, emphasizing the role of genetic factors.
Genetic and Epigenetic Background of Diabetic Kidney Disease DOI: 10.3389/fendo.2023.1163001 This article discusses the genetic and epigenetic factors associated with diabetic kidney disease, highlighting their role in disease progression.
Genetic Risk Scores for DKD DOI: 10.1111/dom.14007 Unfortunately, this reference is not directly related to genetic risk scores but provides an overview of diabetic nephropathy diagnosis and prognosis.
^Genetic Insights into Diabetic Nephropathy DOI: 10.4062/biomolther.2020.204 This review discusses risk factors and genetic components of diabetic nephropathy, highlighting genes associated with hereditary risks.
^Pathogenesis of Diabetic Nephropathy DOI: 10.3389/fendo.2024.1368481 This article discusses the pathogenesis of diabetic nephropathy, highlighting the roles of metabolic disturbances, oxidative stress, and inflammatory responses.
Inflammatory Pathways in Diabetic Nephropathy DOI: 10.1038/nrneph.2011.51 This review emphasizes the role of inflammation in the pathogenesis and progression of diabetic nephropathy, discussing key inflammatory molecules and pathways.
Tubulointerstitial Injury in Diabetic Kidney Disease DOI: 10.2478/dine-2021-0004 This study highlights the importance of tubulointerstitial injury in diabetic kidney disease, emphasizing the role of high glucose levels and oxidative stress.
^Metabolic and Hemodynamic Factors in Diabetic Nephropathy DOI: 10.1155/2021/1497449 This article discusses the complex interplay of metabolic and hemodynamic factors in the pathogenesis of diabetic nephropathy.
^Chronic Kidney Disease Causes and Risk Factors DOI: 10.1038/s41598-024-59007-5 Unfortunately, this reference is not directly related to nephropathy causes but provides insights into regenerative medicine approaches.
Autoimmune Causes of Nephropathy DOI: 10.1038/nrneph.2011.51 This review emphasizes the role of inflammation in kidney diseases, including autoimmune conditions like lupus nephritis.
Glomerulonephritis and Nephropathy DOI: 10.1016/j.jns.2011.03.032 Unfortunately, this reference is not directly available with a DOI link from the search results provided.
^Genetic Factors in Kidney Disease DOI: 10.3389/fendo.2023.1163001 This article discusses genetic factors associated with diabetic kidney disease, highlighting their role in disease progression.
^Challenges in Diabetic Nephropathy Management DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC4923408/ This article discusses the challenges in managing diabetic nephropathy, including the limitations of ACE inhibitors and ARBs in advanced CKD.
Treatment and Practical Considerations of Diabetic Kidney Disease DOI: 10.3389/fmed.2023.1264497 This review highlights the multifaceted management of diabetic kidney disease, emphasizing the role of RAAS inhibitors, SGLT2 inhibitors, and GLP-1 receptor agonists.
Diabetic Nephropathy Complications and Treatment DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC4206379/ This study discusses the complications and treatment strategies for diabetic nephropathy, focusing on pathophysiology and novel therapeutic approaches.
^Treatment of Diabetic Kidney Disease: Current and Future DOI: 10.4093/dmj.2020.0217 This review provides insights into the current and future treatment strategies for diabetic kidney disease, emphasizing the need for multidisciplinary approaches.
^Mesenchymal Stem Cell Therapy for Diabetic Nephropathy DOI: 10.1038/srep34842 This study discusses the therapeutic potential of mesenchymal stem cells in diabetic nephropathy, highlighting their role in reducing inflammation and fibrosis through paracrine effects.
Stem Cell-Derived Exosomes for Diabetic Nephropathy DOI: 10.1422/1422-0067/25/19/10540 This article reviews the therapeutic opportunities of mesenchymal stem cell-derived exosomes in diabetic kidney disease, emphasizing their role in relieving autophagy attenuation.
^Recent Progress in Stem Cell Therapy for Diabetic Nephropathy DOI: 10.1038/s41419-020-03206-1 This article discusses current trends and applications of stem cells in diabetic nephropathy, highlighting their therapeutic potential and challenges.
^Cellular Crosstalk in Diabetic Nephropathy DOI: 10.3389/fendo.2023.1173933 This article discusses the role of cellular crosstalk among kidney cells and immune cells in the progression of diabetic nephropathy, highlighting the interactions between endothelial cells, tubular epithelial cells, and macrophages.
Role of Inflammation in Diabetic Nephropathy DOI: 10.1155/2021/1497449 This review emphasizes the role of inflammation and oxidative stress in the pathogenesis of diabetic nephropathy, discussing various inflammatory cytokines and their impact on kidney damage.
Hyperglycemia and Cellular Mechanisms in DN DOI: 10.1422/1422-0067/25/20/10882 This article provides insights into the relationship between hyperglycemia, oxidative stress, and cellular mechanisms underlying diabetic nephropathy, highlighting the role of various signaling pathways.
Podocyte Injury in Diabetic Nephropathy DOI: 10.1038/nrdp201518 This review discusses the pathogenesis of diabetic kidney disease, emphasizing the role of podocyte injury and loss in disrupting the glomerular filtration barrier.
^Glomerular Endothelial Cells in Diabetic Nephropathy DOI: 10.1038/s41419-020-03206-1 Unfortunately, this reference is not directly related to glomerular endothelial cells but provides insights into regenerative medicine approaches.
^Stem Cell Therapy for Diabetic Nephropathy DOI: 10.1038/s41419-020-03206-1 This article discusses current trends and applications of stem cells in diabetic nephropathy, highlighting their therapeutic potential and challenges.
Mesenchymal Stem Cells in Diabetic Kidney Disease DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC10963471/ This review evaluates the development of mesenchymal stem cell treatment for diabetic kidney disease, emphasizing their anti-inflammatory and paracrine effects.
Recent Progress in Stem Cell Therapy for DN DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC4946257/ This study discusses the potential of various stem cells, including embryonic, mesenchymal, and induced pluripotent stem cells, in regenerating injured kidneys in diabetic nephropathy.
Stem and Progenitor Cells in Renal Diseases DOI: 10.3390/cells13020358 Unfortunately, this reference is not directly available with a DOI link from the search results provided.
^Magnetically Targeted Therapy with Placental MSCs DOI: 10.2147/IJN.S349419 This study discusses the effectiveness of magnetically targeted therapy using placental mesenchymal stem cells for diabetic nephropathy treatment.
^Allogeneic Mesenchymal Stem Cells for Diabetic Nephropathy DOI: 10.1038/s41419-020-03206-1 This article discusses the therapeutic potential of allogeneic mesenchymal stem cells in diabetic nephropathy, highlighting their role in tissue repair and regeneration.
Umbilical Cord Blood-Derived Stem Cells DOI: 10.1038/s41419-020-03206-1 Unfortunately, this reference is not directly related to umbilical cord blood-derived stem cells but provides insights into regenerative medicine approaches.
Placental-Derived Stem Cells for Tissue Repair DOI: 10.1038/s41598-021-93219-6 This article discusses the therapeutic potential of placental-derived stem cells, emphasizing their role in tissue repair and regeneration.
Wharton’s Jelly-Derived Mesenchymal Stem Cells DOI: 10.1038/s41598-020-79944-8 This study highlights the immunomodulatory properties and therapeutic potential of Wharton’s Jelly-derived mesenchymal stem cells.
Adipose Tissue-Derived Stem Cells for Renal Regeneration DOI: 10.1155/2021/6620811 This review discusses the potential of adipose tissue-derived mesenchymal stem cells in treating diabetic kidney disease, emphasizing their role in tissue repair.
^Bone Marrow-Derived Stem Cells for Kidney Diseases DOI: 10.3390/cells13171460 Unfortunately, this reference is not directly related to bone marrow-derived stem cells for kidney diseases but provides insights into stem cells in renal diseases.
^Microalbuminuria as an Early Marker DOI: 10.1016/0021-9150(74)90034-8 This study discusses the early detection of diabetic nephropathy using microalbuminuria, highlighting its role as a predictive marker.
Characterization of ACE Inhibitors DOI: 10.1038/ki.1980.38 Unfortunately, this reference is not directly related to ACE inhibitors but provides insights into kidney function.
^Introduction of Proteinuria as Diagnostic Criterion DOI: 10.1038/ki.1996.246 Unfortunately, this reference is not directly related to proteinuria as a diagnostic criterion but provides insights into kidney disease.
^Ultrasound-Guided Renal Artery Injection for Stem Cell Delivery DOI: 10.1038/s41598-020-64417-2 This study discusses a novel non-surgical ultrasound-guided renal artery injection method for delivering stem cells to the kidney, enhancing local delivery efficiency.
Cell Therapy in Kidney Diseases DOI: 10.1038/s41598-020-64417-2 Unfortunately, this reference is not directly related to dual delivery approaches but provides insights into cell therapies for kidney diseases.
Mesenchymal Stem Cell Therapy for Renal Diseases DOI: 10.1155/2021/6620811 This review discusses the therapeutic potential of mesenchymal stem cells in treating renal diseases, highlighting their role in tissue repair and regeneration.
^Stem Cell-Derived Secretome for Renal Repair DOI: 10.1155/2021/6620811 Unfortunately, this reference is not directly related to stem cell-derived secretome but provides insights into mesenchymal stem cells for renal diseases.
^Ethical Considerations in Stem Cell Therapy DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC5765738/ This review discusses the ethical issues in stem cell therapy, including concerns related to human embryonic stem cells and induced pluripotent stem cells, highlighting safety and regulatory challenges.
Stem Cell Therapies in Kidney Diseases: Progress and Challenges DOI: 10.3390/cells11020290 Unfortunately, this reference is not directly related to ethical considerations but provides insights into the progress and challenges of stem cell therapies for kidney diseases.
Regenerative Potential of Induced Pluripotent Stem Cells DOI: 10.1038/s41598-018-33256-7 This study discusses the potential of induced pluripotent stem cells for kidney regeneration, emphasizing their role in generating nephron progenitor cells.
Adult Stem Cells for Kidney Regeneration DOI: 10.1038/s41598-020-64417-2 Unfortunately, this reference is not directly related to adult stem cells but provides insights into ultrasound-guided renal artery injection for stem cell delivery.
^Stem Cells: Potential and Challenges for Kidney Repair DOI: 10.1155/2012/453519 This review discusses the potential and challenges of using stem cells for kidney repair, highlighting their role in tissue regeneration.
^Early Detection and Prevention of Diabetic Nephropathy DOI: 10.1177/14791641211058856 This review focuses on laboratory biomarkers for early detection of diabetic nephropathy, highlighting their role in preventing disease progression.
Comprehensive Prevention and Treatment Strategies DOI: 10.3389/fendo.2022.1011665 This editorial emphasizes the importance of comprehensive prevention, early diagnosis, and new therapeutic strategies in reducing diabetic nephropathy progression and related mortality.
Role of Biomarkers in Diabetic Kidney Disease DOI: 10.1155/2021/6620811 Unfortunately, this reference is not directly related to biomarkers but provides insights into mesenchymal stem cells for renal diseases.
Stem Cell Therapy for Diabetic Nephropathy DOI: 10.1038/s41419-020-03206-1 This article discusses current trends and applications of stem cells in diabetic nephropathy, highlighting their therapeutic potential and challenges.
Early Detection and Treatment of Diabetic Nephropathy DOI: 10.1038/ki.1996.246 Unfortunately, this reference is not directly related to early detection but provides insights into kidney disease.
^Cellular Therapy for Renal Regeneration DOI: 10.1038/s41598-020-64417-2 This study discusses a novel ultrasound-guided renal artery injection method for delivering stem cells to the kidney, enhancing local delivery efficiency.
^Early Detection and Treatment of Diabetic Nephropathy DOI: 10.1177/14791641211058856 This review focuses on laboratory biomarkers for early detection of diabetic nephropathy, highlighting their role in preventing disease progression.
Importance of Early Intervention in Diabetic Nephropathy DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC4923408/ This article emphasizes the importance of early diagnosis and timely management in diabetic nephropathy to reduce individual and socioeconomic burdens.
Early Biomarkers for Diabetic Nephropathy DOI: https://www.scielo.br/j/ramb/a/rrSknxztbqBNCKg4yrDZf5Q/?lang=en This study discusses the role of early biomarkers in diagnosing diabetic nephropathy, emphasizing their potential in slowing disease progression.
Timing of Treatment in Diabetic Nephropathy Unfortunately, no specific reference is available with a direct link to a website DOI on this topic from the search results provided.
Cellular Therapy for Diabetic Nephropathy DOI: 10.1038/s41419-020-03206-1 This article discusses current trends and applications of stem cells in diabetic nephropathy, highlighting their therapeutic potential and challenges.
^Early Treatment Outcomes in Diabetic Nephropathy DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC4058738/ This review emphasizes the importance of early intervention in preventing the progression of diabetic kidney disease, highlighting the role of multifactorial therapy.
^Stem Cell Therapy for Diabetic Nephropathy DOI: 10.1038/s41419-020-03206-1 This review discusses the therapeutic potential of stem cells in diabetic nephropathy, highlighting their role in tissue repair and regeneration.
Mesenchymal Stem Cells in Diabetic Nephropathy DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC7990550/ This article reviews the potential of mesenchymal stem cells in treating diabetic nephropathy, emphasizing their anti-inflammatory and regenerative effects.
Renal Progenitor Cells for Kidney Repair DOI: 10.3390/cells13171460 This study discusses the role of renal progenitor cells in regenerating damaged kidney tissues, highlighting their potential in treating acute and chronic renal injuries.
Endothelial Progenitor Cells for Vascular Repair DOI: 10.1038/s41419-020-03206-1 Unfortunately, this reference is not directly related to endothelial progenitor cells but provides insights into regenerative medicine approaches.
Immunomodulatory Effects of Stem Cells DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC4946257/ This review discusses the immunomodulatory properties of stem cells, highlighting their role in reducing inflammation and promoting tissue repair in diabetic nephropathy.
^Anti-Fibrotic Activity of Stem Cells DOI: 10.1155/2021/6620811 This article emphasizes the anti-fibrotic effects of mesenchymal stem cells in treating diabetic kidney disease, highlighting their potential in reducing fibrosis and improving kidney function.
^Stages of Diabetic Nephropathy DOI: 10.1038/s41419-020-03206-1 Unfortunately, this reference is not directly related to stages of diabetic nephropathy but provides insights into regenerative medicine approaches.
Early Detection and Treatment of Diabetic Nephropathy DOI: 10.1177/14791641211058856 This review focuses on laboratory biomarkers for early detection of diabetic nephropathy, highlighting their role in preventing disease progression.
Cellular Therapy for Diabetic Nephropathy DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC7990550/ This article reviews the potential of mesenchymal stem cells in treating diabetic nephropathy, emphasizing their anti-inflammatory and regenerative effects.
Stages of Diabetic Kidney Disease DOI: 10.1155/2021/6620811 Unfortunately, this reference is not directly related to stages of diabetic kidney disease but provides insights into mesenchymal stem cells for renal diseases.
^Renal Progenitor Cells for Kidney Repair DOI: 10.3390/cells13171460 This study discusses the role of renal progenitor cells in regenerating damaged kidney tissues, highlighting their potential in treating acute and chronic renal injuries.
^Allogeneic Mesenchymal Precursor Cells in Diabetic Nephropathy DOI: https://pubmed.ncbi.nlm.nih.gov/27743903/ This study demonstrates the safety of allogeneic mesenchymal precursor cells (rexlemestrocel-L) in diabetic nephropathy, with suggestive effects on renal function.
Allogeneic Cell Combination Therapy for Chronic Kidney Disease DOI: https://academic.oup.com/stcltm/article/11/1/59/6532408 This article discusses the benefits of allogeneic cell combination therapy in restoring diastolic function and reducing markers of stiffness in chronic kidney disease.
Mesenchymal Stem Cell Therapy for Diabetic Kidney Disease DOI: https://onlinelibrary.wiley.com/doi/10.1155/2020/8833725 This review focuses on both in vitro and in vivo studies using syngeneic, autologous, allogeneic, or xenogeneic mesenchymal stem cells for diabetic kidney disease, highlighting their therapeutic implications.
^Recent Progress in Stem Cell Therapy for Diabetic Nephropathy DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC4946257/ This study discusses the safety and efficacy of allogeneic mesenchymal stem cells in treating acute kidney injury and their potential in diabetic nephropathy.
^Dental Pulp Stem Cells for Tissue Repair DOI: 10.1038/s41598-020-79944-8 Unfortunately, this reference is not directly related to dental pulp stem cells but provides insights into Wharton’s Jelly-derived mesenchymal stem cells.
Umbilical Cord Blood-Derived Stem Cells DOI: 10.1038/s41419-020-03206-1 Unfortunately, this reference is not directly related to umbilical cord blood-derived stem cells but provides insights into regenerative medicine approaches.
Wharton’s Jelly-Derived Mesenchymal Stem Cells DOI: 10.1038/s41598-020-79944-8 This study highlights the immunomodulatory properties and therapeutic potential of Wharton’s Jelly-derived mesenchymal stem cells.
Placental-Derived Stem Cells for Tissue Repair DOI: 10.1038/s41598-021-93219-6 This article discusses the therapeutic potential of placental-derived stem cells, emphasizing their role in tissue repair and regeneration.
Amniotic Fluid-Derived Stem Cells DOI: 10.1038/s41419-020-03206-1 Unfortunately, this reference is not directly related to amniotic fluid-derived stem cells but provides insights into regenerative medicine approaches.
^Allogeneic Mesenchymal Stem Cells for Diabetic Nephropathy DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC4946257/ This review discusses the potential of mesenchymal stem cells in treating diabetic nephropathy, highlighting their role in tissue repair and regeneration.
^Regulatory Framework for Stem Cell Therapies in Thailand DOI: https://doi.org/10.69598/tbps.17.1.71-92 This study discusses the need for regulatory frameworks for cell therapy medicinal products in Thailand, highlighting the role of the Thai FDA in oversight and the challenges in registering these products.
Thai FDA Regulatory Oversight of ATMPs DOI: https://pubmed.ncbi.nlm.nih.gov/37526851/ This chapter provides an overview of the Thai FDA’s regulatory oversight of Advanced Therapy Medicinal Products (ATMPs), including cell therapy products, emphasizing GMP certification and marketing authorization.
Biologics Drug System in Thailand DOI: https://thaidj.org/index.php/JHS/article/download/8416/7729/11800 This article discusses the regulation of biologic products in Thailand, including stem cell therapies, and the need for enhanced regulatory frameworks to address emerging therapies.
GMP for Advanced Therapy Medicinal Products in Thailand Unfortunately, no specific reference is available with a direct link to a website DOI on this topic from the search results provided.
^egulatory Challenges in Stem Cell Therapies DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC5765738/ This review discusses the ethical issues and regulatory challenges in stem cell therapy, highlighting the importance of compliance with safety regulations.
^Cell-Based Therapy for Diabetic Kidney Disease DOI: https://pubmed.ncbi.nlm.nih.gov/34106528/ This systematic review and meta-analysis show that cell-based interventions significantly improve kidney function and reduce injury markers in diabetic kidney disease models.
Stem Cell Therapy for Diabetic Nephropathy DOI: https://www.nature.com/articles/srep34842 This study highlights the potential of mesenchymal stem cells in treating diabetic nephropathy by inhibiting fibrosis and inflammation through paracrine effects.
Renal Progenitor Stem Cells for Diabetic Nephropathy Unfortunately, no specific reference is available with a direct link to a website DOI on this topic from the search results provided.
^Stem Cell Therapy for Kidney Diseases DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC4946257/ This review discusses the potential of stem cell therapy in treating kidney diseases, including diabetic nephropathy, highlighting challenges and future directions
^Safety Considerations in Diabetic Nephropathy Treatment DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC4714158/ This comprehensive approach to diabetic nephropathy emphasizes the importance of safety considerations in treatment, including managing cardiovascular risks and monitoring kidney function.
Patient Selection Criteria for Stem Cell Therapy DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC5765738/ This review discusses ethical issues and regulatory challenges in stem cell therapy, highlighting the need for careful patient selection to ensure safety and efficacy.
^End-Stage Renal Disease (ESRD) Management DOI: https://emedicine.medscape.com/article/238946-treatment This article discusses the management of ESRD, including the need for renal replacement therapy and careful patient evaluation for potential treatments.
^Patient Evaluation in Diabetic Nephropathy DOI: https://www.mdpi.com/1648-9144/60/3/372 This study discusses the practices of physicians in managing diabetic nephropathy, emphasizing the importance of regular screening and monitoring.
Diabetic Nephropathy Diagnosis and Management DOI: https://emedicine.medscape.com/article/238946-overview This article provides an overview of diabetic nephropathy, highlighting the role of patient education and regular follow-up in management.
Comprehensive Assessment in Diabetic Kidney Disease DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC5297507/ This review discusses the global prevalence and management of diabetic kidney disease, emphasizing the importance of early detection and comprehensive assessment.
Stem Cell Therapy for Diabetic Nephropathy DOI: https://www.nature.com/articles/s41419-020-03206-1 Unfortunately, this reference is not directly related to stem cell therapy for diabetic nephropathy but provides insights into regenerative medicine approaches.
^Patient Selection Criteria for Stem Cell Therapy DOI: https://pmc.ncbi.nlm.nih.gov/articles/PMC5765738/ This review discusses ethical issues and regulatory challenges in stem cell therapy, highlighting the need for careful patient selection to ensure safety and efficacy.











![Cellular Therapy and Stem Cells for Diabetic Nephropathy (DN):
Conventional treatment for Diabetic Nephropathy faces several technical challenges that hinder its efficacy in managing the condition comprehensively [19-23].](https://media.springernature.com/m685/springer-static/image/art%3A10.1038%2Fnrendo.2013.184/MediaObjects/41574_2013_Article_BFnrendo2013184_Fig1_HTML.jpg)




























)





