At Dr. StemCellsThailand, we are dedicated to advancing the field of regenerative medicine through innovative cellular therapies and stem cell treatments. With over 20 years of experience, our expert team is committed to providing personalized care to patients from around the world, helping them achieve optimal health and vitality. We take pride in our ongoing research and development efforts, ensuring that our patients benefit from the latest advancements in stem cell technology. Our satisfied patients, who come from diverse backgrounds, testify to the transformative impact of our therapies on their lives, and we are here to support you on your journey to wellness.
In the quest for innovative therapies, cellular therapy and the transformative potential of stem cells offer a promising frontier for exploration. Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases, with their unique capacity for differentiation and immunomodulation, hold immense promise for revolutionizing the treatment of autoimmune and connective tissue diseases, offering new avenues for restoring immune balance and tissue homeostasis.
Nature, with its vast repertoire of adaptations and survival strategies, provides inspiration for biomedical Research and Clinical Trials. Among its marvels are the antibodies of sharks and camels, which possess remarkable immunomodulatory properties capable of regulating the body’s immune response and tempering autoimmunity.
Sharks and camels have evolved antibodies that exhibit unique structures and functions, enabling them to target pathogens with unparalleled specificity and efficiency. In addition to their potent antimicrobial properties, these antibodies have demonstrated remarkable immunomodulatory effects, regulating immune cell activity and tempering excessive inflammation.
Studies have shown that shark and camel antibodies can effectively modulate autoimmune responses in preclinical models, offering insights into potential therapeutic applications for human autoimmune and connective tissue diseases. By harnessing the immunomodulatory properties of these antibodies, researchers aim to develop novel Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases capable of restoring immune balance and promoting tissue repair in patients with these disorders.
Through interdisciplinary collaboration and translational Research and Clinical Trials, the lessons learned from nature’s marvels hold promise for revolutionizing the treatment of autoimmune and connective tissue diseases. By harnessing the regenerative potential of Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases and drawing inspiration from the extraordinary immunomodulatory properties of shark and camel antibodies, researchers strive to unlock new frontiers in autoimmune and connective tissue disease therapy, offering hope to millions of individuals worldwide battling these debilitating conditions[1-5].
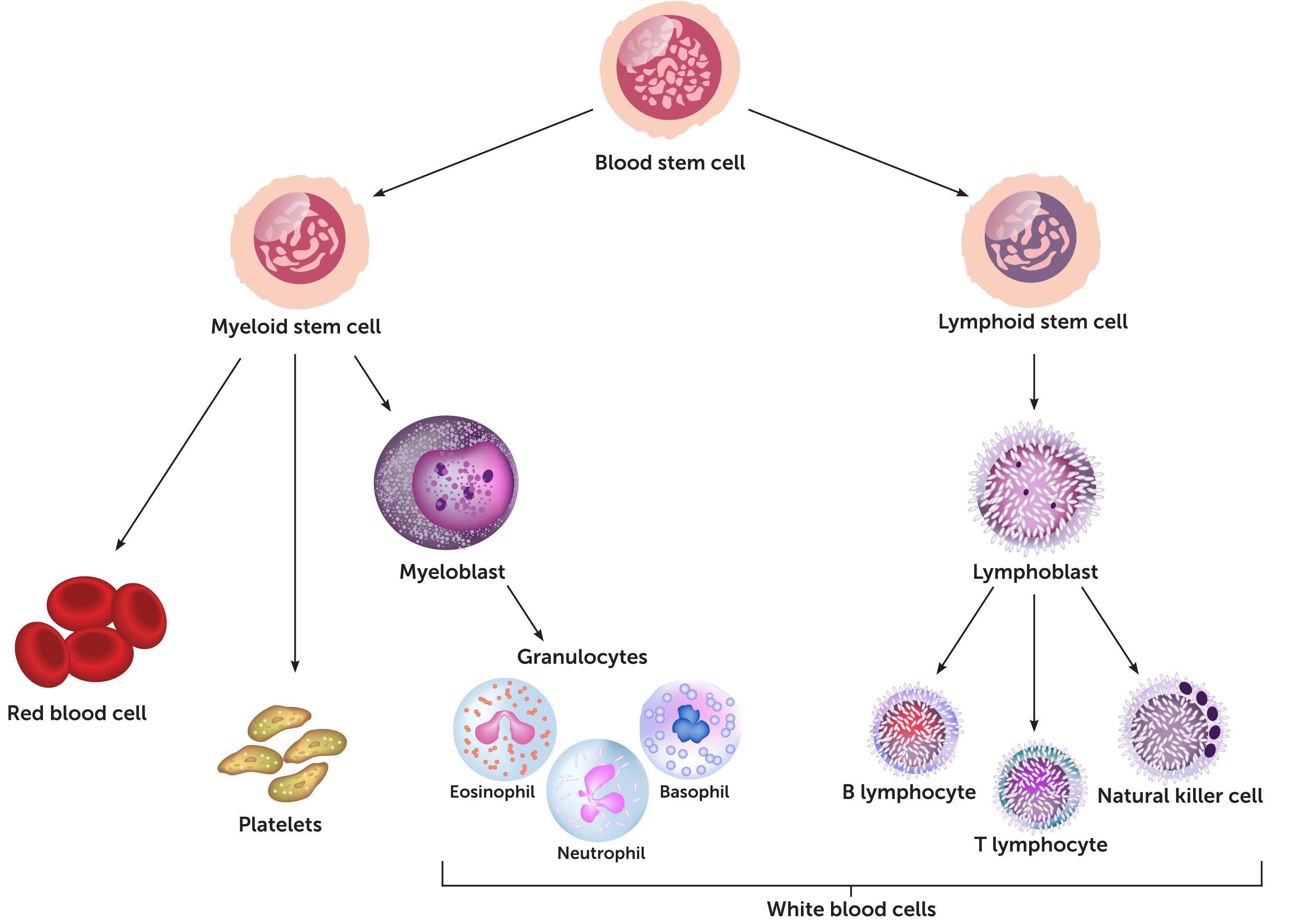
Autoimmune and connective tissue diseases involve a complex interplay of various immune cells. Here are the primary cells involved in the progression of these conditions:
– Release histamine and other inflammatory mediators, playing a role in immune responses.
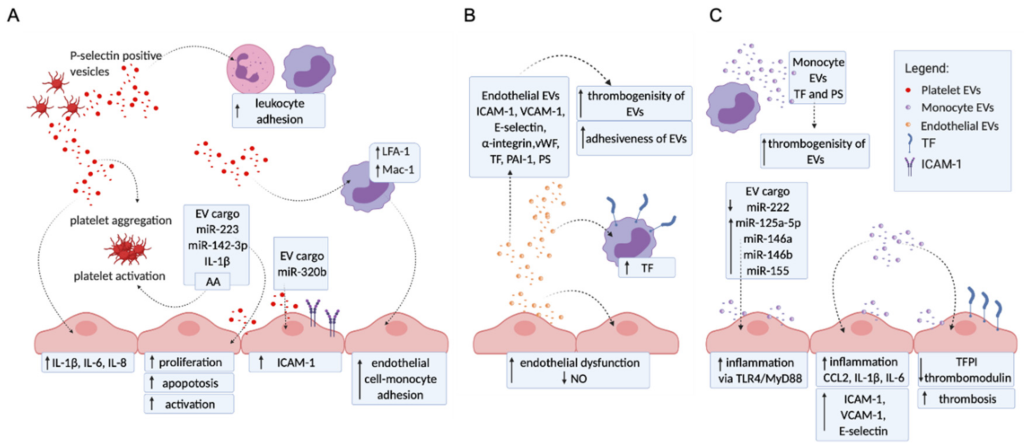
11. Endothelial Cells
– Line blood vessels and can be involved in inflammatory processes by expressing adhesion molecules and cytokines, facilitating the migration of immune cells into tissues.
These cells interact through a network of cytokines, chemokines, and other signaling molecules, creating a complex and often self-perpetuating cycle of inflammation and tissue damage characteristic of autoimmune and connective tissue diseases[6-10].
Key Immune Cells Involved in the Progression of Autoimmune and Connective Tissue Diseases and Their Immunomodulation through Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases with Organ-Specific Progenitor Stem Cells
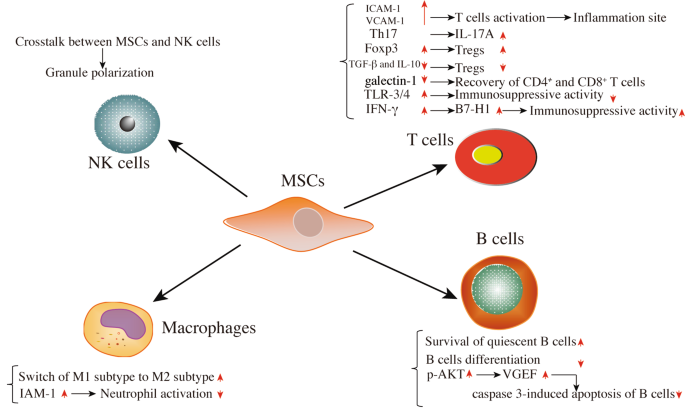
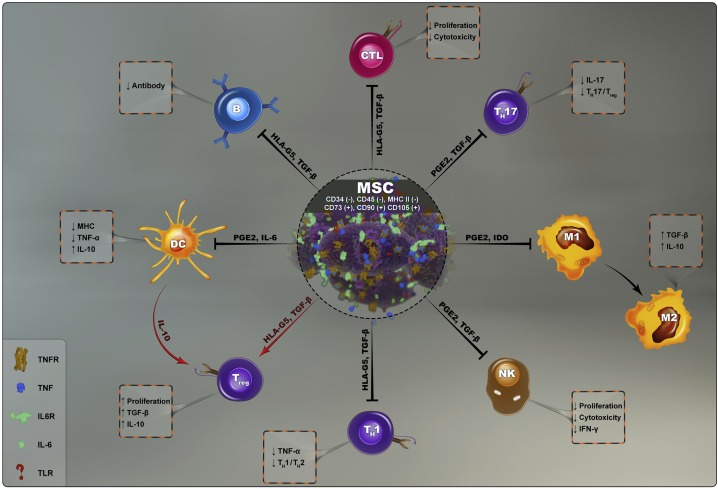
– CD4+ T Helper Cells: Use Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases to shift the balance from pro-inflammatory Th1 and Th17 cells to anti-inflammatory Th2 and Treg cells.
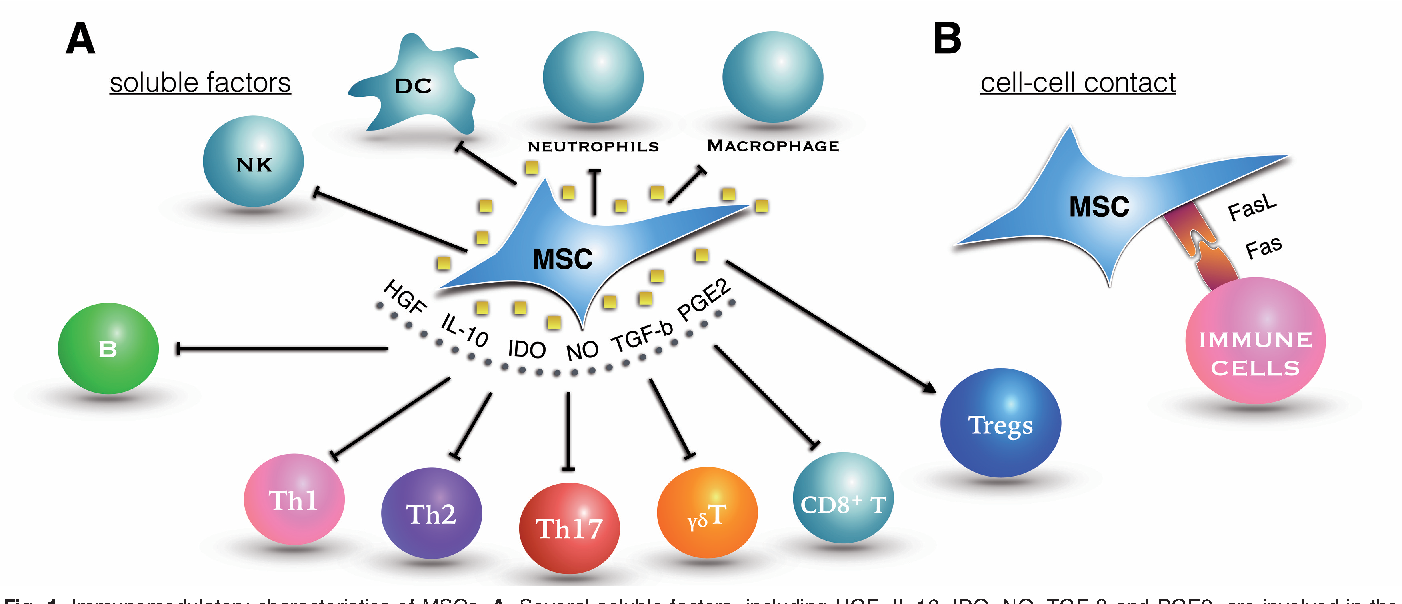
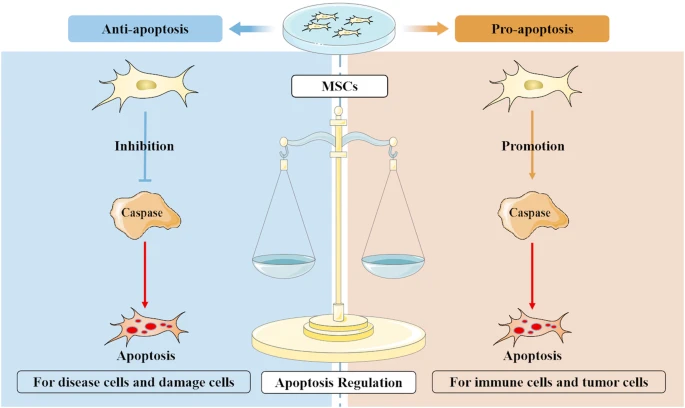
– Th1 and Th17 Cells: Suppress these cells using mesenchymal stem cells (MSCs) which can secrete anti-inflammatory cytokines like IL-10.
– Treg Cells: Expand Tregs using MSCs or ex vivo expansion and reinfusion techniques to enhance immune tolerance.
– Pro-Inflammatory Macrophages (M1): Use MSCs to shift macrophages from the M1 phenotype to the anti-inflammatory M2 phenotype, reducing tissue damage and inflammation.
– Prevalence: RA affects about 1% of the global population, with a higher prevalence in women than men.
– Economic Impact: In the U.S., the annual direct medical cost for a patient with RA can range from $10,000 to $30,000. Indirect costs, including lost productivity, are estimated to be up to $19,000 per year per patient.
– Disability: Up to 50% of RA patients are unable to work within 10 years of disease onset.
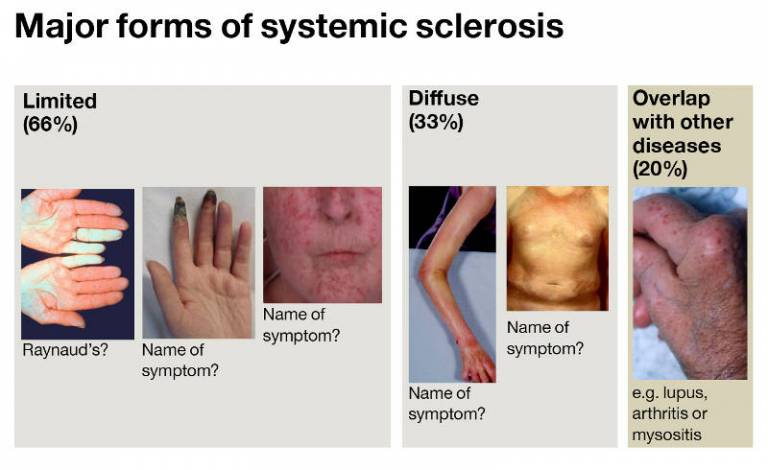
– Prevalence: Scleroderma (Systemic Sclerosis) affects about 20-50 people per 100,000 globally, with localized scleroderma being more common than systemic scleroderma.
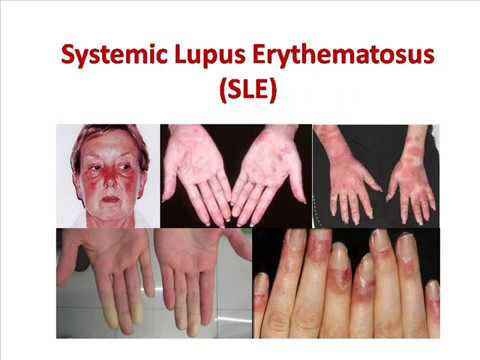
– Prevalence: SLE affects approximately 20-70 people per 100,000 globally, with significant regional variations.
– Gender Disparity: Women are up to 9 times more likely to develop SLE than men.
– Mortality: SLE patients have a standardized mortality ratio (SMR) approximately 2-3 times higher than that of the general population, largely due to complications like cardiovascular diseases and infections.
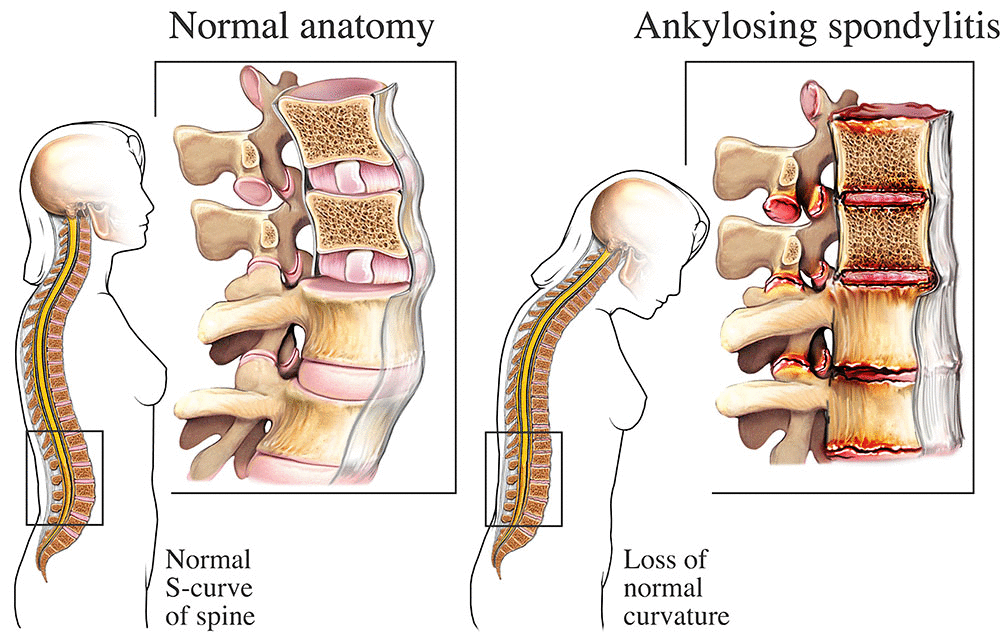
Prevalence: Ankylosing spondylitis affects approximately 0.1%–0.5% of the global population, with higher prevalence in Caucasian and Indigenous populations.
Quality of Life: Patients experience chronic back pain, stiffness, and reduced spinal mobility, significantly impacting physical and mental well-being. Fatigue is a common symptom.
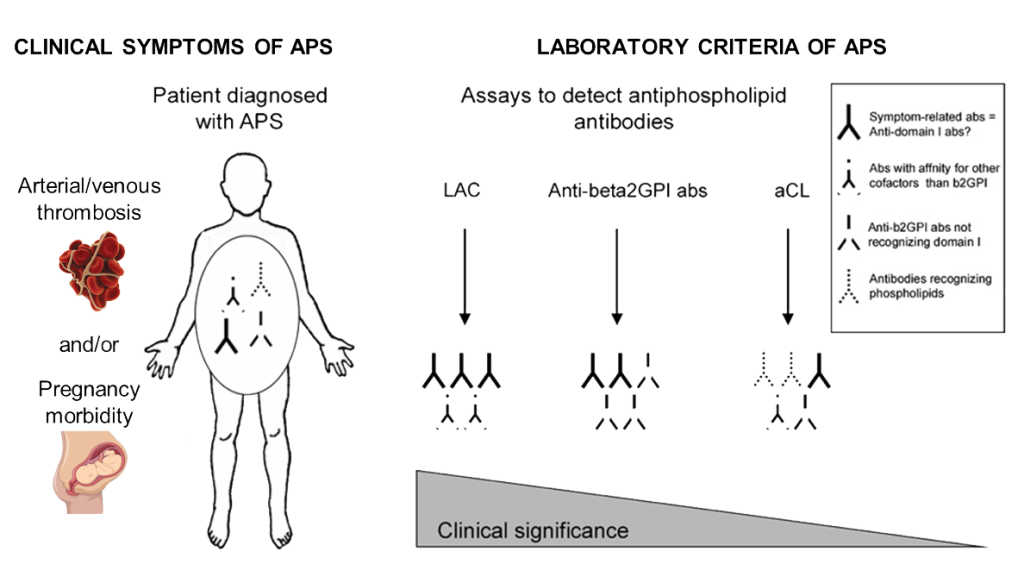
Prevalence: APS is estimated to affect about 40–50 cases per 100,000 individuals, with a higher prevalence in females.
Quality of Life: APS is characterized by recurrent blood clots, pregnancy complications, and neurological symptoms, leading to reduced quality of life due to chronic health challenges.
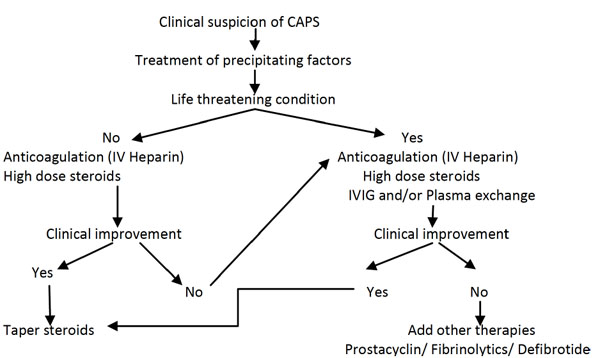
Mortality: Untreated APS can result in life-threatening events, such as stroke, myocardial infarction, or catastrophic antiphospholipid syndrome (CAPS), contributing to higher mortality rates.
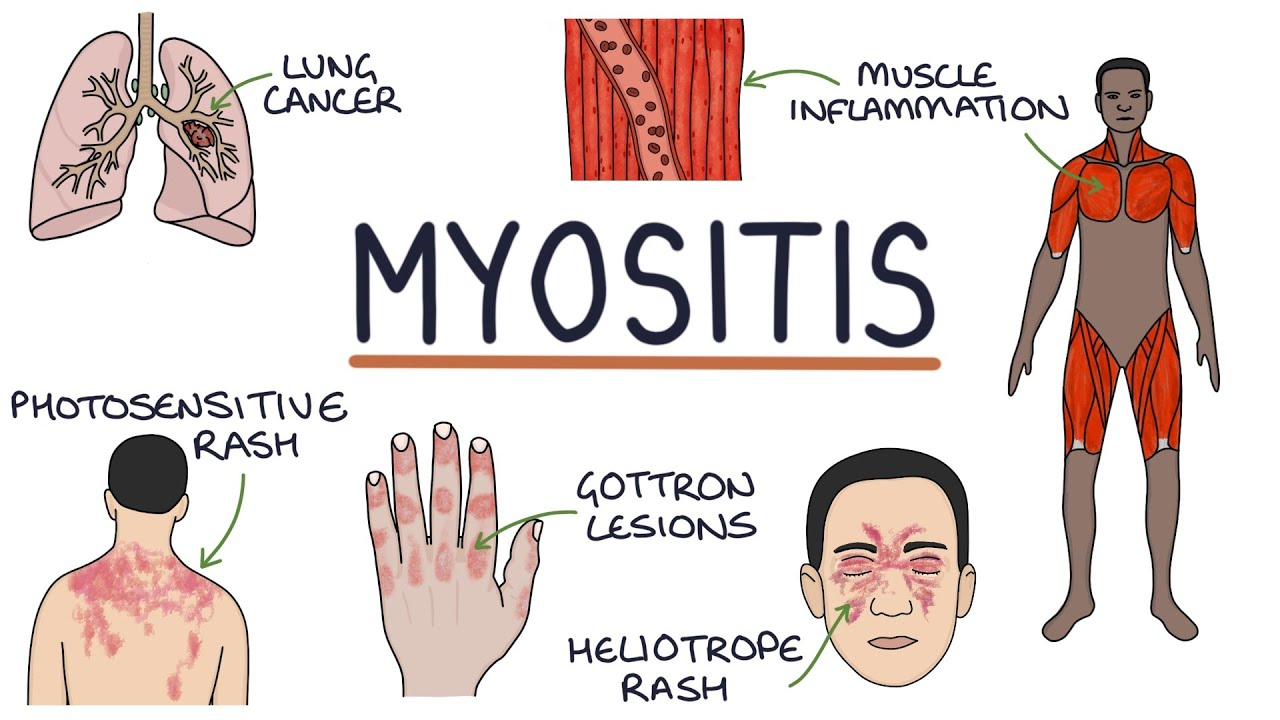
Prevalence: Dermatomyositis has an estimated prevalence of 1–10 cases per 100,000 individuals, affecting both adults and children.
Quality of Life: Patients suffer from muscle weakness, skin rashes, and systemic symptoms like fatigue and dysphagia, severely impairing daily functioning.
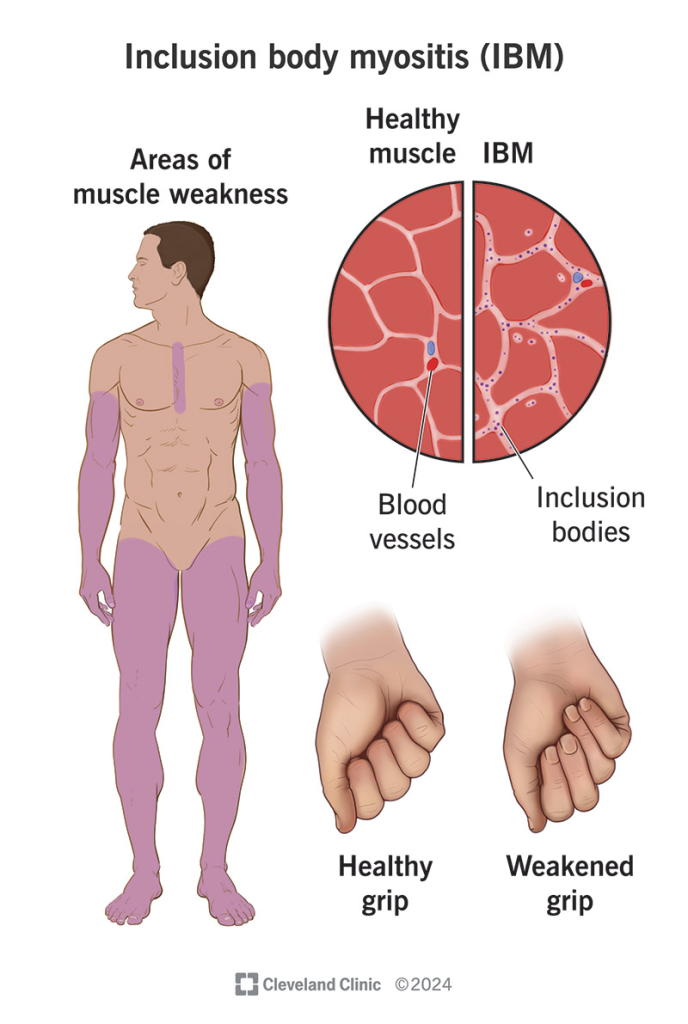
Prevalence: IBM is a rare condition, affecting approximately 15–70 cases per 1 million people, more commonly in individuals over 50 years of age.
Quality of Life: It leads to progressive muscle weakness, particularly in the quadriceps and forearm muscles, causing significant physical disability over time.
Mortality: Although not directly fatal, complications like falls, respiratory failure, and aspiration pneumonia contribute to increased mortality in advanced stages.
Mortality: While not typically fatal, complications such as lymphoma and organ involvement may increase mortality risk.
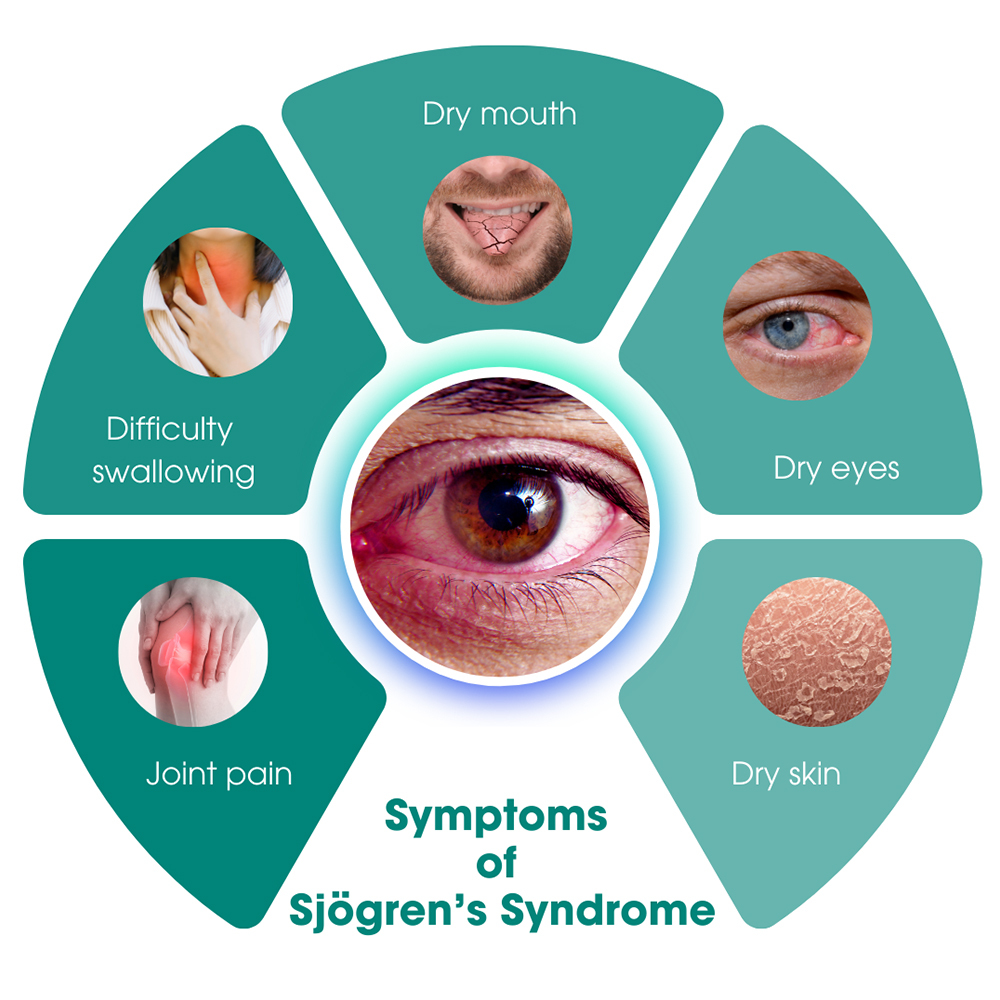
Prevalence: Sjögren’s syndrome affects approximately 0.1%–4% of the population, with a marked female predominance.
Quality of Life: Symptoms include dry eyes and mouth, fatigue, and joint pain, profoundly impacting both physical and emotional well-being. Secondary Sjögren’s can coexist with other autoimmune diseases.
Prevalence: Polymyositis is rare, with an estimated prevalence of 1–10 cases per 100,000 individuals, primarily affecting adults, especially women, between 30 and 60 years of age.
Quality of Life: Patients experience progressive muscle weakness, particularly in the proximal muscles, leading to difficulties in performing daily tasks like climbing stairs or lifting objects. Fatigue and systemic symptoms are common.
– Early Diagnosis: RA often has a gradual onset, making early diagnosis difficult. Delayed diagnosis can lead to joint damage before effective treatment is initiated.
– Treatment Response: Not all patients respond to conventional DMARDs (Disease-Modifying Anti-Rheumatic Drugs) or biologics, and some develop resistance over time.
– Side Effects: Long-term use of medications like steroids and biologics can lead to significant side effects, including increased infection risk and cardiovascular issues.
– Heterogeneity: Scleroderma presents with a wide range of symptoms, from localized skin involvement to severe systemic disease, making standard treatment protocols challenging.
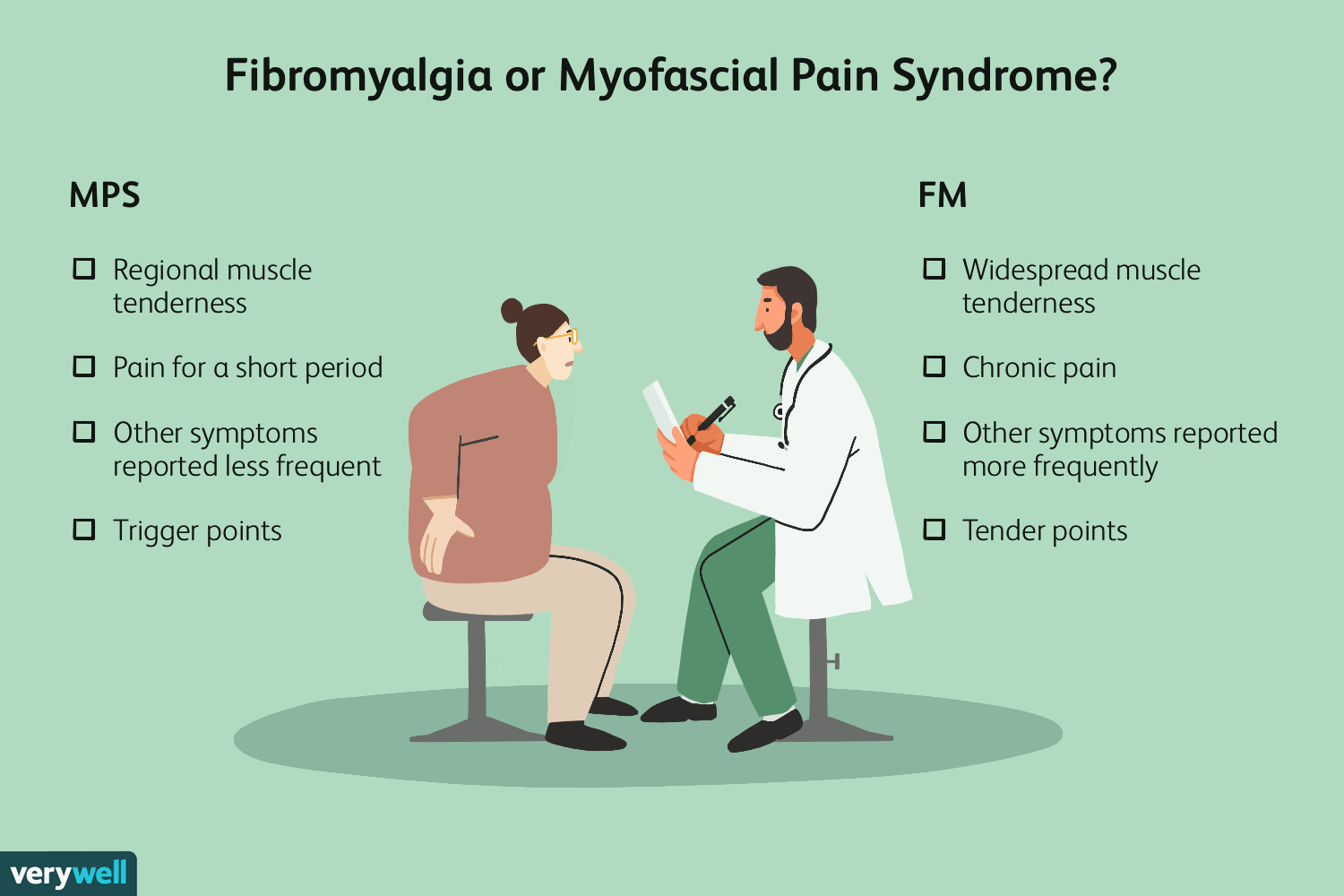
– Diagnosis: FM is often misdiagnosed or underdiagnosed due to the lack of specific diagnostic tests and overlapping symptoms with other conditions.
– Treatment Efficacy: Current treatments, including medications, physical therapy, and cognitive behavioral therapy, are only partially effective and do not work for all patients.
– Chronic Pain Management: Effective management of chronic pain remains a significant challenge, impacting patients’ quality of life.
– Stigma: FM patients often face stigma and disbelief about the legitimacy of their condition, which can affect their mental health and access to appropriate care.
– Diagnosis: IIMs are rare and can be difficult to diagnose due to their varied presentations and overlap with other conditions.
– Treatment Resistance: Some patients do not respond well to standard immunosuppressive treatments.
– Disease Monitoring: Regular monitoring of disease activity and treatment side effects is challenging due to the need for frequent clinical and laboratory evaluations.
Etiology: AS is primarily associated with genetic factors, particularly the HLA-B27 gene, and environmental triggers, although the exact pathogenesis remains unclear.
Diagnosis: Diagnosis is based on clinical evaluation, imaging (e.g., X-rays or MRI), and genetic testing for HLA-B27. Misdiagnosis is common due to overlapping symptoms with other back pain disorders.
Etiology: APS is an autoimmune disorder characterized by the presence of antiphospholipid antibodies, triggering thrombosis and pregnancy complications. Its exact cause is unknown.
Diagnosis: Diagnosis involves clinical criteria (e.g., history of thrombosis or pregnancy loss) and laboratory testing for antiphospholipid antibodies (e.g., lupus anticoagulant, anticardiolipin, β2-glycoprotein I).
Symptom Management: Management focuses on anticoagulation therapy (e.g., warfarin or heparin) and preventive measures to reduce thrombotic risk.
Quality of Life: Recurrent thrombotic events and associated complications reduce physical function and cause psychological stress.
Diagnosis: Diagnosis involves clinical features and the presence of high titers of anti-U1 RNP antibodies. Misdiagnosis can occur due to overlapping symptoms with other autoimmune diseases.
Symptom Management: Treatment is tailored to the predominant symptoms and includes corticosteroids, immunosuppressants, and symptomatic therapy.
Quality of Life: Symptoms like fatigue, Raynaud’s phenomenon, and joint pain can significantly reduce quality of life.
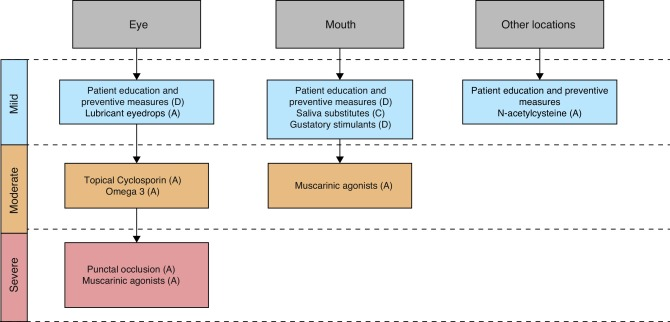
Etiology: Sjögren’s syndrome is an autoimmune disorder characterized by lymphocytic infiltration of exocrine glands, though its exact cause is unknown.
Diagnosis: Diagnosis is based on clinical features (e.g., dry eyes and mouth), serologic markers (e.g., anti-Ro/SSA, anti-La/SSB antibodies), and salivary gland biopsy.
Symptom Management: Treatment focuses on symptomatic relief using artificial tears, salivary stimulants, and immunomodulatory therapy in severe cases.
Quality of Life: Chronic dryness, fatigue, and systemic manifestations lead to reduced physical, emotional, and social well-being.
Etiology: PM is an autoimmune inflammatory myopathy, likely triggered by genetic and environmental factors, but the precise etiology is unclear.
Diagnosis: Diagnosis is made through clinical evaluation, elevated muscle enzymes, electromyography, and muscle biopsy findings showing inflammatory infiltrates.
Symptom Management: Treatment includes corticosteroids, immunosuppressive agents, and physical therapy to manage inflammation and restore function.
Quality of Life: Muscle weakness and systemic involvement significantly impair physical function and the ability to perform daily activities.
Immune-Enhanced Organ-Specific Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases with Progenitor Stem Cells: A Potential Strategy for Autoimmune and Connective Tissue Diseases at Our Anti-Aging and Regenerative Medicine Center of Thailand
Promising Results from Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases with Organ-Specific Progenitor Stem Cell Therapies in Autoimmune and Connective Tissue Diseases at our Center.
Preclinical studies, Research and Clinical Trials have shown encouraging results for using Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases with organ-specific progenitor stem cell therapies to treat various autoimmune and connective tissue diseases. These therapies involve using specific types of progenitor stem cells that have the potential to regenerate damaged and dead cells while also modulating overactive immune responses. Here are some detailed insights into these promising therapies:
– Research and Clinical Trials: Early clinical trials in RA patients have demonstrated improved symptoms and reduced disease activity with MSC therapy.
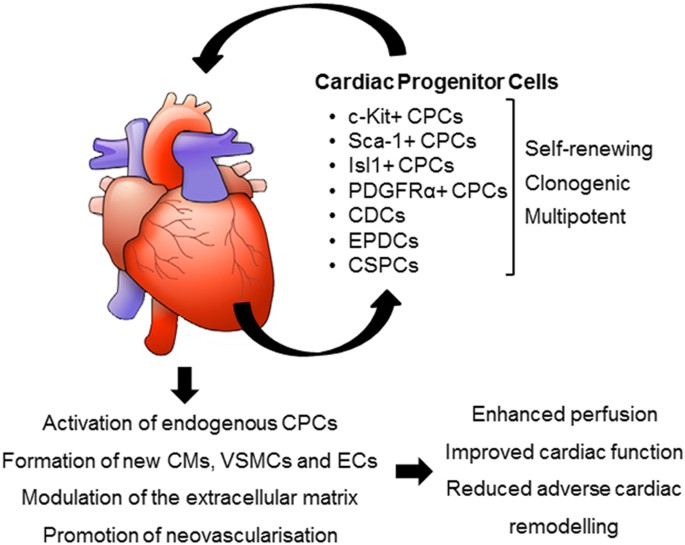
– Heart Repair: In autoimmune diseases affecting the heart, such as lupus myocarditis, cardiac progenitor stem cells can regenerate damaged cardiac tissues.
– Improved Cardiac Function: Preclinical models have shown improved cardiac function and reduced fibrosis with progenitor stem cell therapy.
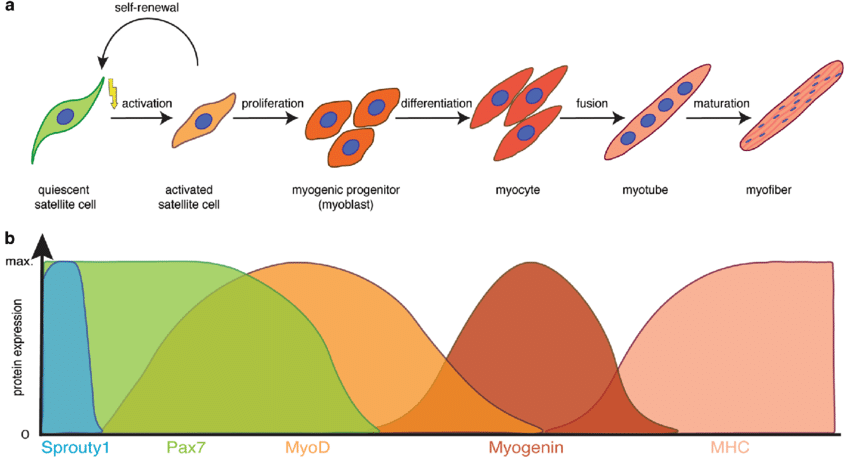
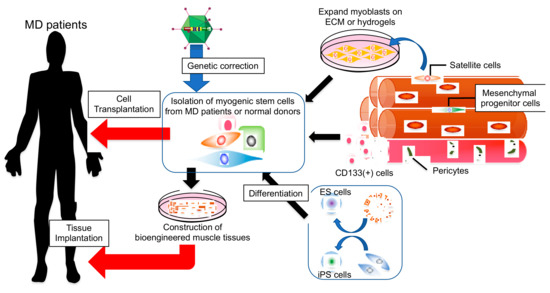
Myogenic Progenitor Stem Cells
– Muscle Regeneration: In idiopathic inflammatory myopathies (IIMs) like Dermatomyositis (DM) and Polymyositis (PM), myogenic progenitor stem cells can regenerate damaged muscle tissues.
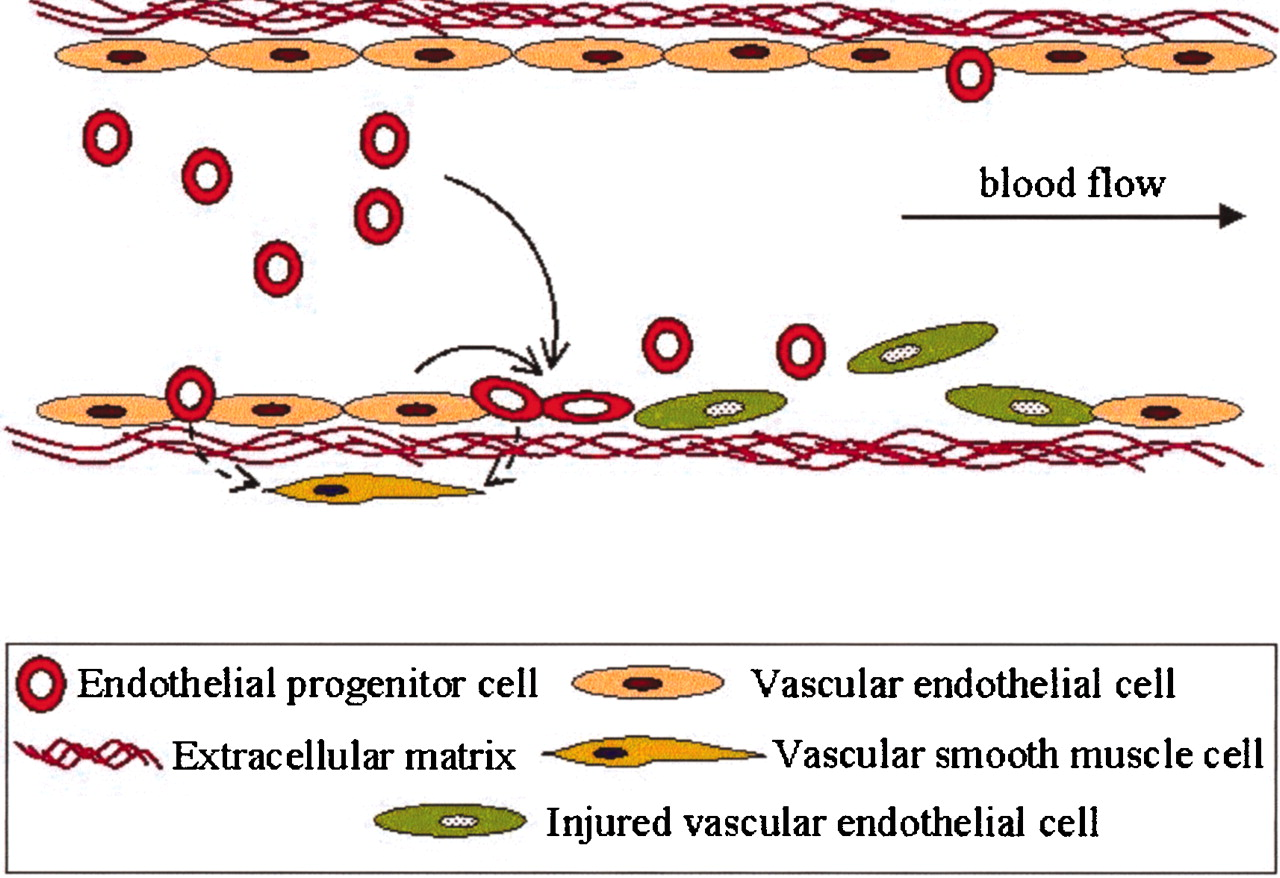
– Vascular Repair: These cells can regenerate damaged blood vessels, crucial for conditions like Scleroderma (Systemic Sclerosis) where vascular damage is prominent.
– Improved Blood Flow: Improved vascular function and reduced symptoms have been observed in preclinical and clinical models.
– Research and Clinical Trials: Early clinical trials have shown that intra-articular injection of MSCs in Rheumatoid Arthritis (RA) patients leads to significant improvement in joint function and reduction in disease activity. Patients reported decreased pain and increased mobility.
– Dermal Progenitor Stem Cells: These cells can help regenerate healthy skin and reduce fibrosis. MSCs also play a role in modulating the immune system and reducing skin tightening.
– Preclinical Studies: Studies on animal models have shown that dermal progenitor stem cells can significantly improve skin elasticity and reduce fibrosis.
– Research and Clinical Trials: Limited early trials have demonstrated that Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases can improve skin condition and overall functionality in scleroderma patients.
– Research and Clinical Trials: Studies have shown that HSC transplantation can lead to long-term remission in SLE patients. Patients experienced reduced disease activity and a decrease in the need for immunosuppressive medications.
– MSC Therapy: MSCs can also modulate the immune response and reduce inflammation. Early trials have shown improvement in SLE symptoms with MSC therapy.
– Preclinical and Clinical Studies: Research and Clinical Trials have shown that Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases can reduce pain and improve overall function in FM.
– MSCs and Neural Progenitor Stem Cells: These cells can help repair neural damage and modulate immune responses, addressing the chronic fatigue and neurological symptoms of CFS.
– Preclinical and Clinical Studies: Research and Clinical Trials have indicated that Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases can improve energy levels and reduce fatigue.
– MSCs and Neural Progenitor Stem Cells: These cells can aid in the repair of damaged neural tissues and modulate the immune system to reduce inflammation.
– Research Outcomes: Patients treated with Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases have experienced slower disease progression and improved mobility.
Research and Clinical Trials: Studies have demonstrated that MSC therapy can reduce disease activity and improve spinal mobility. Preliminary clinical trials suggest reduced inflammation in sacroiliac joints and improved quality of life.
Research and Clinical Trials: Early research indicates MSC therapy may reduce the risk of recurrent thrombotic events. Ongoing trials aim to evaluate their efficacy in preventing pregnancy complications associated with APS.
Mesenchymal Stem Cells (MSCs): MSCs may alleviate muscle inflammation and repair damaged muscle tissues through their immunomodulatory and regenerative properties.
Research and Clinical Trials: Initial clinical trials have shown reduced muscle inflammation and improved muscle strength in DM patients treated with MSCs. Further research is underway to confirm these benefits.
Mesenchymal Stem Cells (MSCs): MSCs have the potential to slow muscle degeneration and reduce inflammation, addressing both autoimmune and degenerative components of IBM.
Research and Clinical Trials: Limited clinical data are available, but early studies suggest that MSC therapy may improve muscle function and delay progression in Inclusion Body Myositis (IBM) patients.
Research and Clinical Trials: Emerging evidence indicates that MSC therapy may improve symptoms like joint pain, fatigue, and Raynaud’s phenomenon. Research and Clinical Trials are ongoing to determine long-term efficacy.
Mesenchymal Stem Cells (MSCs): MSCs have shown potential in regenerating salivary gland function and reducing systemic autoimmune activity in Sjögren’s syndrome.
Research and Clinical Trials: Preliminary studies report improved salivary secretion and reduced inflammation in Sjögren’s syndrome patients treated with MSCs. Research and Clinical Trials are being conducted to validate these findings.
Mesenchymal Stem Cells (MSCs): MSCs help reduce muscle inflammation and promote regeneration of damaged muscle fibers in PM through their anti-inflammatory and regenerative effects.
Research and Clinical Trials: Initial trials suggest improved muscle strength and reduced disease activity in PM patients treated with MSCs[39-47].
Preclinical studies and early clinical trials suggest that Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases with organ-specific progenitor stem cell therapies hold significant promise for treating autoimmune and connective tissue diseases. By regenerating damaged tissues and modulating overactive immune responses, these therapies offer novel approaches that could potentially delay and even reverse disease progression. Further Research and Clinical Trials are necessary to fully understand their efficacy and safety, but these innovative treatments offer hope for improved outcomes and quality of life for patients suffering from these debilitating conditions[39-47].
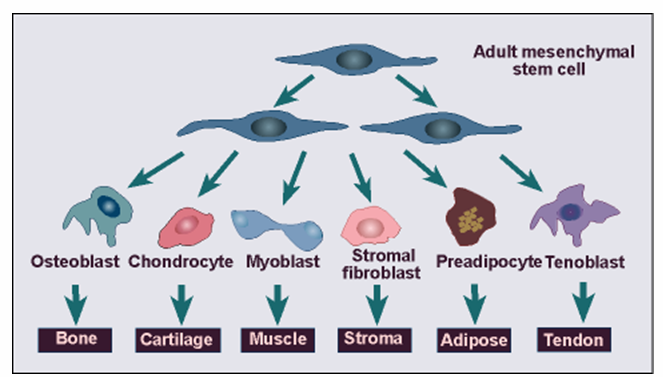
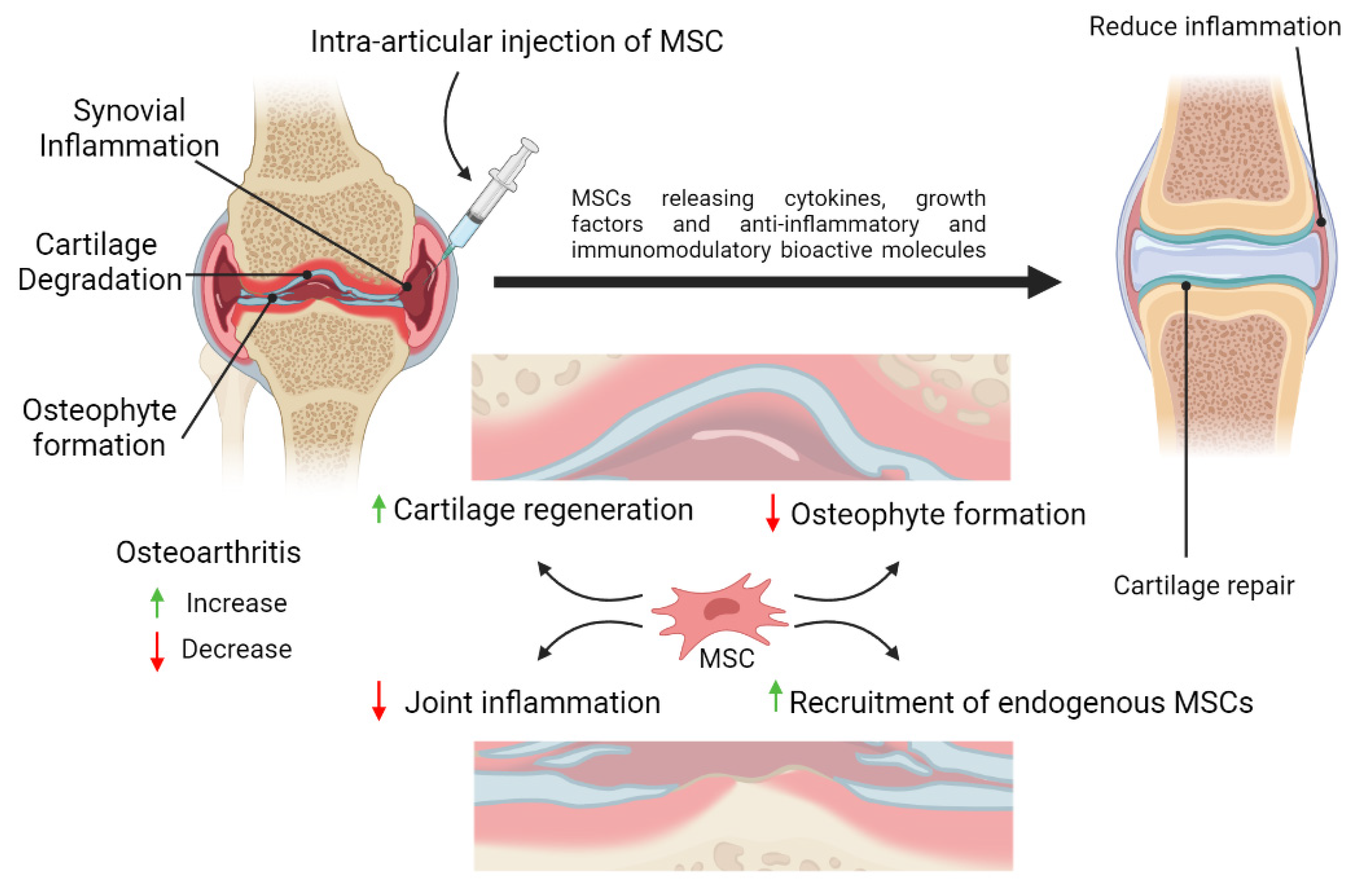
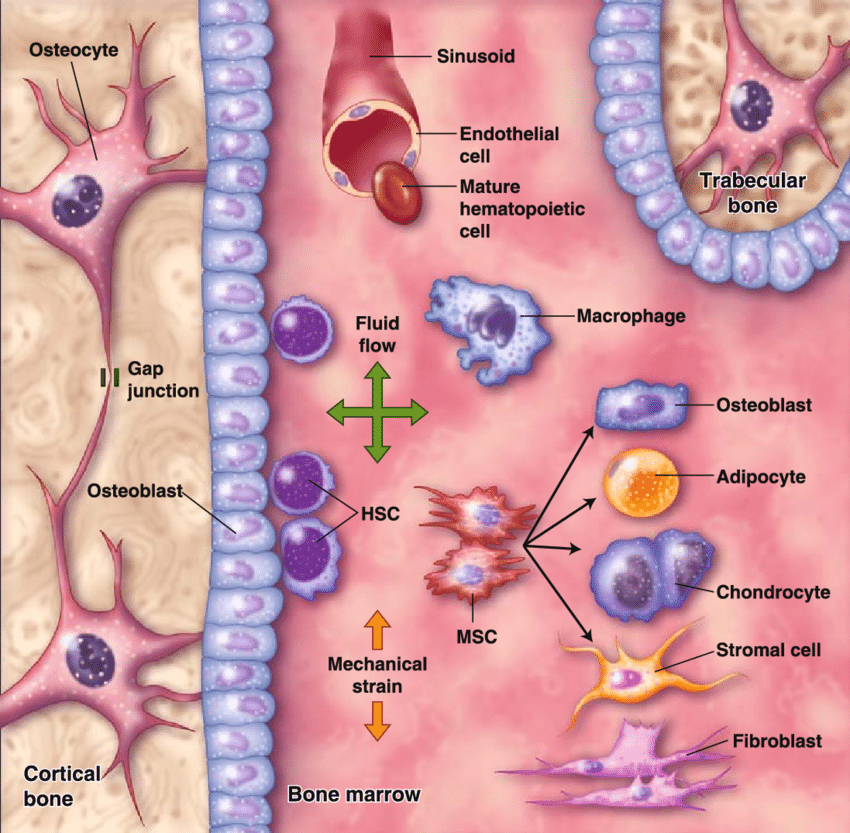
– Mesenchymal Stem Cells (MSCs): These multipotent cells can differentiate into osteoblasts (bone cells), chondrocytes (cartilage cells), and adipocytes (fat cells). In rheumatoid arthritis (RA), MSCs can regenerate joint cartilage, reducing pain and improving mobility.
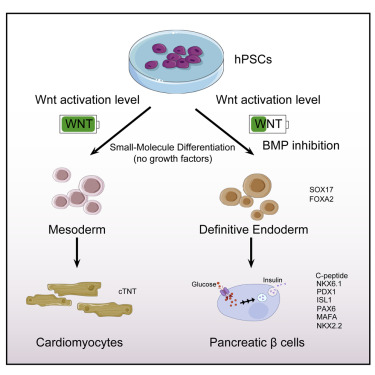
– Pancreatic Progenitor Stem Cells: In type 1 diabetes, these cells can potentially regenerate insulin-producing beta cells and modulate the autoimmune attack on the pancreas[48-52].
– Research and Clinical Trials: Early-phase trials suggest that myogenic progenitor stem cells can lead to muscle regeneration and functional improvement.
– Mechanism: These cells regenerate damaged muscle fibers and reduce inflammation, improving muscle strength and function.
Research and Clinical Trials: Early studies using Mesenchymal Stem Cells (MSCs) therapy in Ankylosing Spondylitis (AS) patients have demonstrated reduced spinal inflammation, improved mobility, and decreased disease activity.
Mechanism: MSCs modulate immune responses, reduce inflammatory cytokines, and potentially prevent joint fusion by promoting tissue repair and reducing fibrosis.
Mechanism: MSCs exert anticoagulant effects and modulate immune system activity, reducing the production of antiphospholipid antibodies and associated inflammation.
Research and Clinical Trials: Clinical trials have shown that Mesenchymal Stem Cells (MSCs) therapy can reduce muscle inflammation, improve strength, and mitigate skin manifestations in Dermatomyositis (DM) patients. Results are promising, but larger studies are needed.
Mechanism: MSCs repair damaged muscle tissue, suppress immune-mediated inflammation, and release trophic factors that enhance muscle regeneration.
Research and Clinical Trials: Research on MSCs in Inclusion Body Myositis (IBM) has shown potential benefits in slowing muscle degeneration and improving muscle function. Ongoing Research and Clinical Trials aim to evaluate therapeutic efficacy.
Mechanism: MSCs reduce inflammatory cytokines, promote muscle regeneration, and provide neuroprotective effects, addressing both inflammatory and degenerative aspects of IBM.
Research and Clinical Trials: Studies report that MSC therapy enhances salivary gland function and reduces systemic inflammation of patients with Sjögren’s syndrome.
Mechanism: MSCs regenerate damaged salivary gland tissue, reduce lymphocytic infiltration, and restore glandular function through their immunomodulatory properties.
Research and Clinical Trials:Mesenchymal Stem Cells (MSCs) therapy has shown promise in reducing muscle inflammation and improving strength in Polymyositis (PM) patients, with early studies indicating positive outcomes. Larger-scale trials are needed.
Mechanism: MSCs repair inflamed and damaged muscle tissues by suppressing pro-inflammatory immune responses and enhancing muscle fiber regeneration.
The focus and purpose of exploring Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases with organ-specific progenitor stem cells in autoimmune and connective tissue diseases are to develop innovative treatments that target disease mechanisms at a cellular level. These therapies aim to regenerate damaged tissues, modulate immune responses, and reduce inflammation, offering significant potential to improve patient outcomes and quality of life. As research progresses, these therapies may become integral components of the treatment arsenal for autoimmune and connective tissue diseases[53-57].
– Skin and Fibrosis Reduction (Scleroderma): Dermal progenitor stem cells can differentiate into fibroblasts, helping to regenerate healthy skin and reduce fibrosis in scleroderma.
– Muscle Repair (IIMs): Myogenic progenitor stem cells can differentiate into muscle fibers, regenerating damaged muscle tissue in idiopathic inflammatory myopathies such as dermatomyositis and polymyositis.
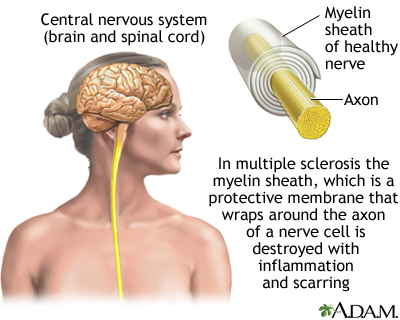
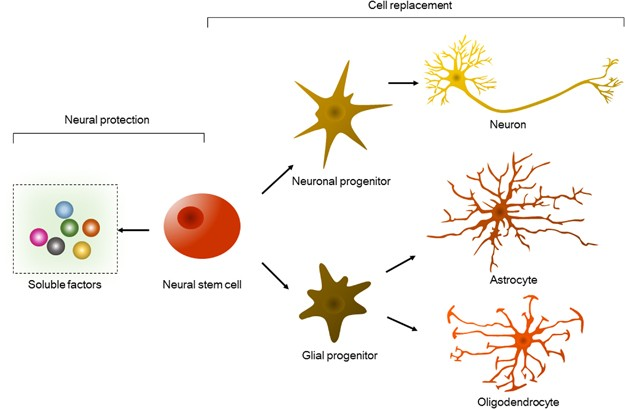
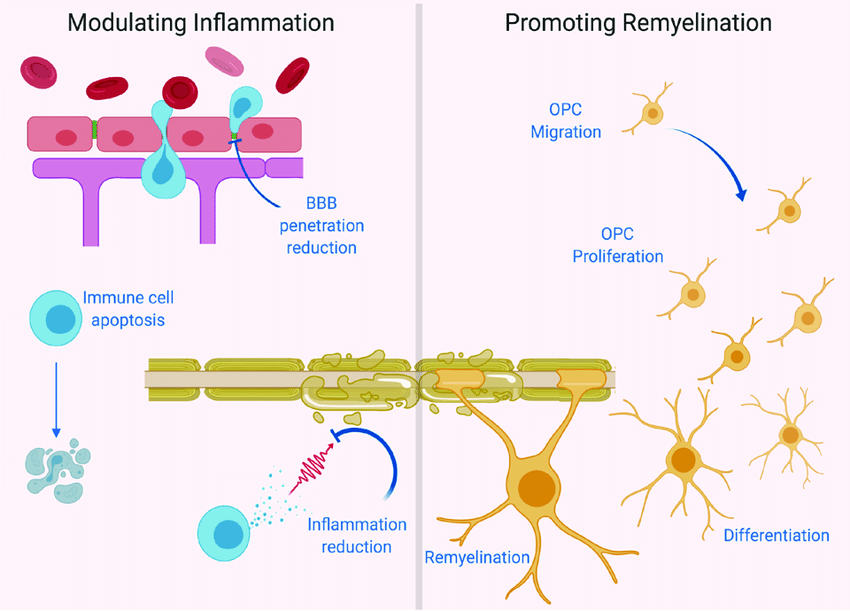
– Neural Repair (MS): Neural progenitor stem cells can differentiate into neurons and oligodendrocytes, promoting the repair of myelin and neural tissues in multiple sclerosis[58-62].
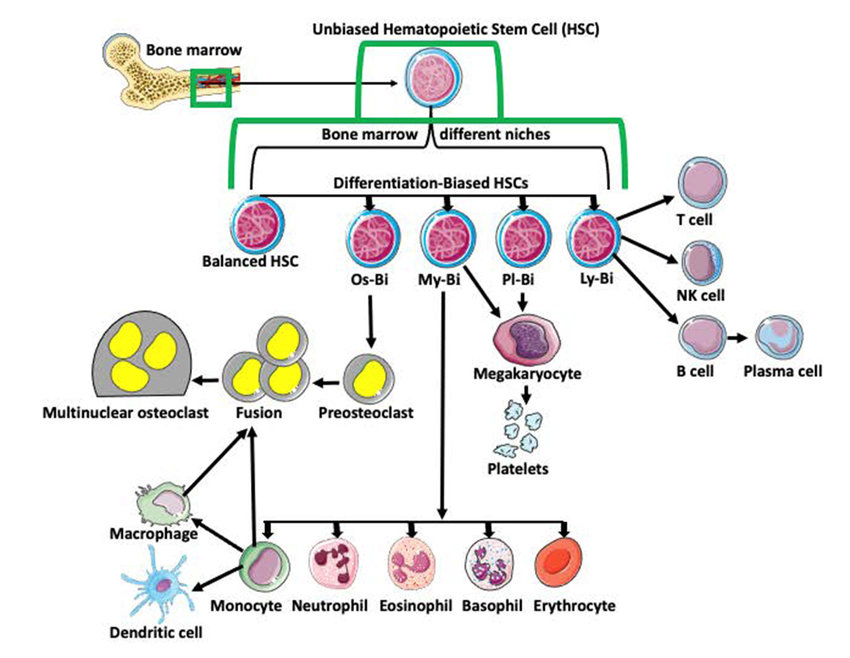
– Hematopoietic Stem Cells (HSCs): HSC transplantation can reset the immune system by eradicating autoreactive immune cells and allowing the regeneration of a new, tolerant immune repertoire. This mechanism is particularly beneficial in severe cases of systemic lupus erythematosus (SLE) and multiple sclerosis (MS).
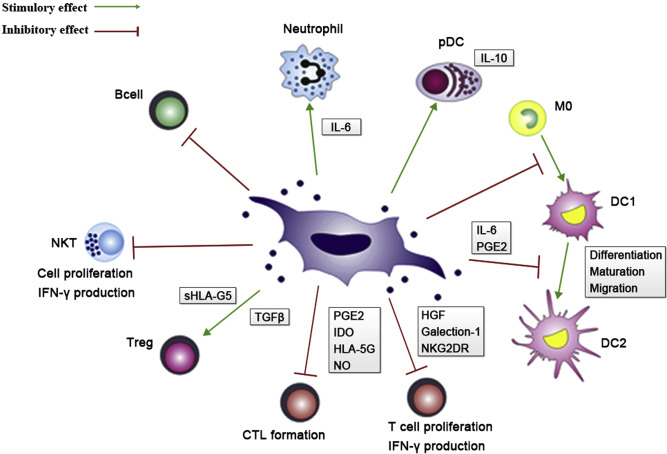
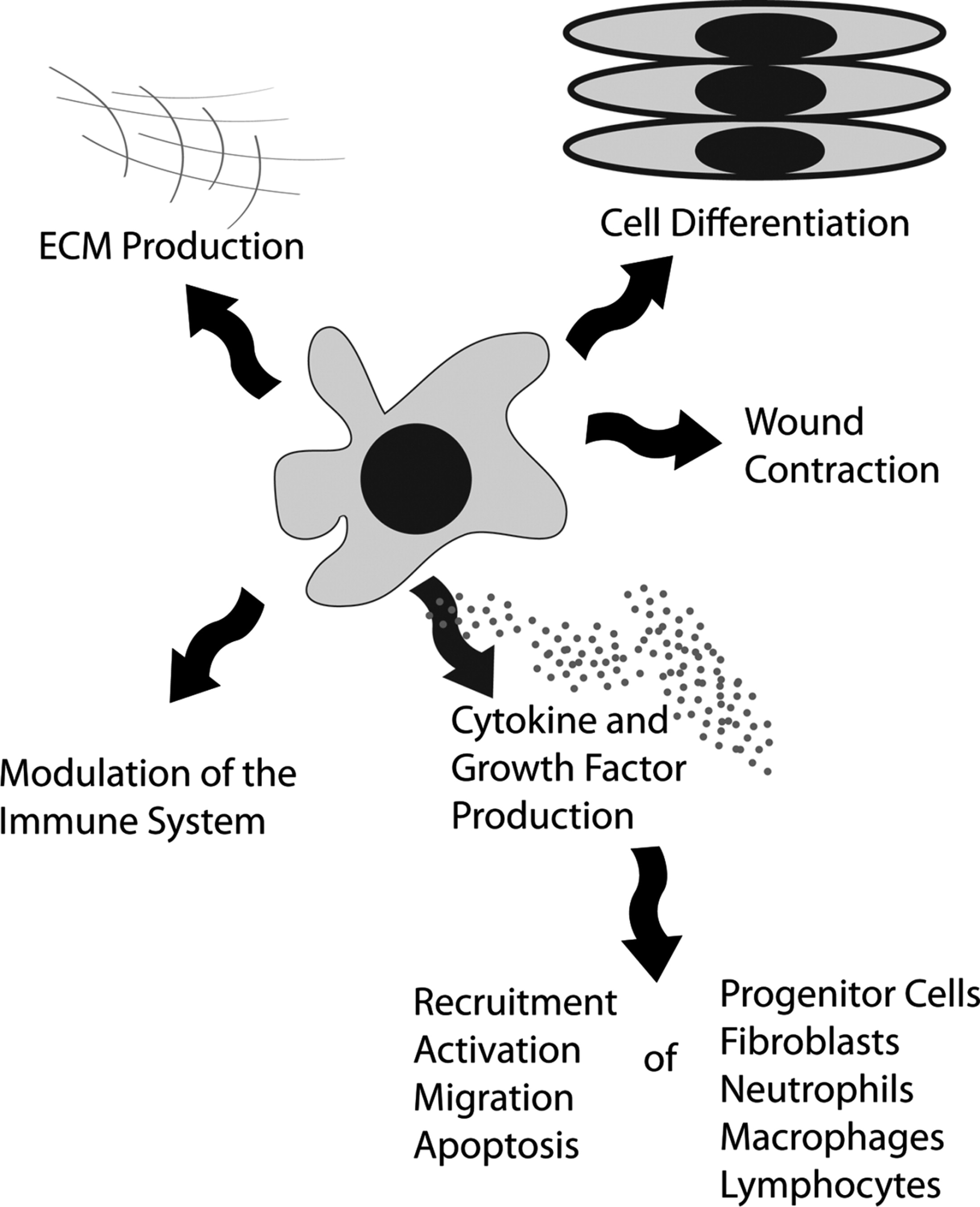
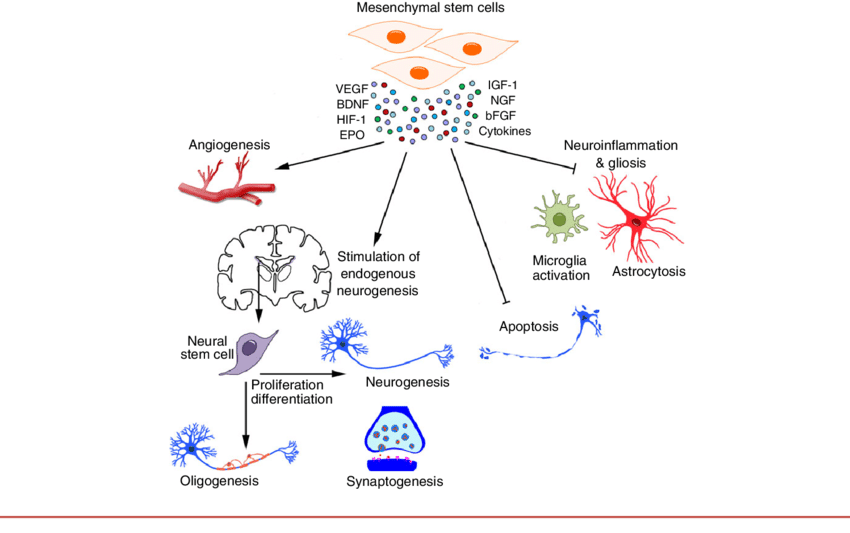
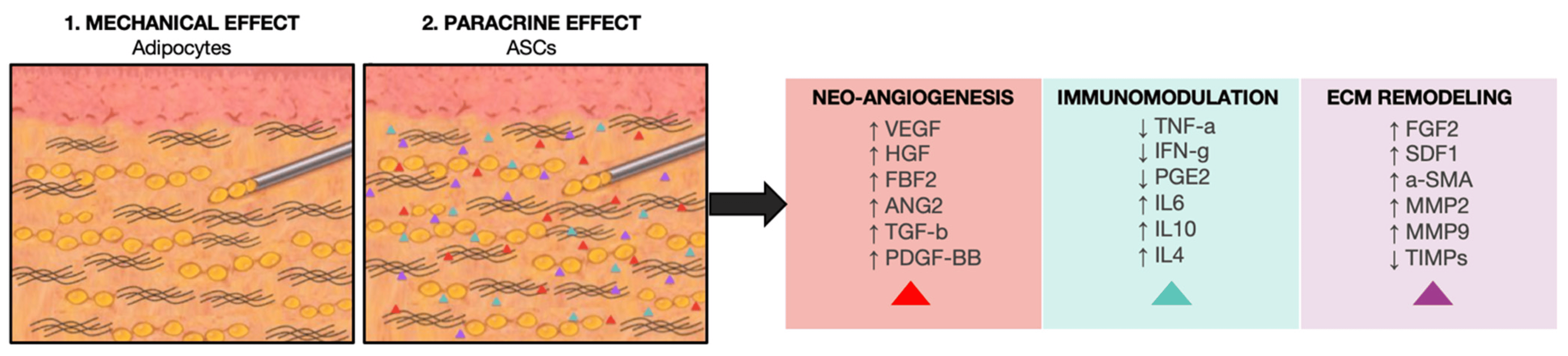
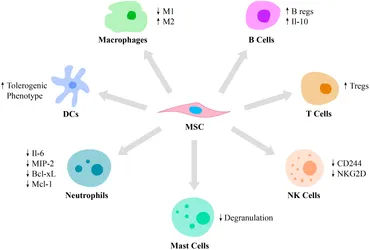
– Mesenchymal Stem Cells (MSCs): MSCs modulate immune responses by secreting immunomodulatory cytokines such as transforming growth factor-beta (TGF-β) and interleukin-10 (IL-10). These cytokines suppress inflammatory T-cell responses and promote the development of regulatory T cells (Tregs), which help maintain immune tolerance[58-62].
– Cytokine Secretion: MSCs secrete a variety of anti-inflammatory cytokines, including TGF-β, IL-10, and prostaglandin E2 (PGE2), which reduce inflammation and inhibit the activity of pro-inflammatory immune cells.
– Inflammatory Pathway Modulation: By interacting with immune cells, MSCs can downregulate inflammatory pathways, such as the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway, reducing the production of pro-inflammatory cytokines and chemokines[58-62].
– Tissue Repair and Angiogenesis: Progenitor stem cells secrete growth factors such as vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF), and hepatocyte growth factor (HGF). These factors promote tissue repair, angiogenesis (formation of new blood vessels), and the regeneration of damaged tissues.
– Anti-Apoptotic Effects: Paracrine factors from stem cells can reduce apoptosis (programmed cell death) in damaged tissues, preserving cell viability and promoting tissue regeneration[58-62].
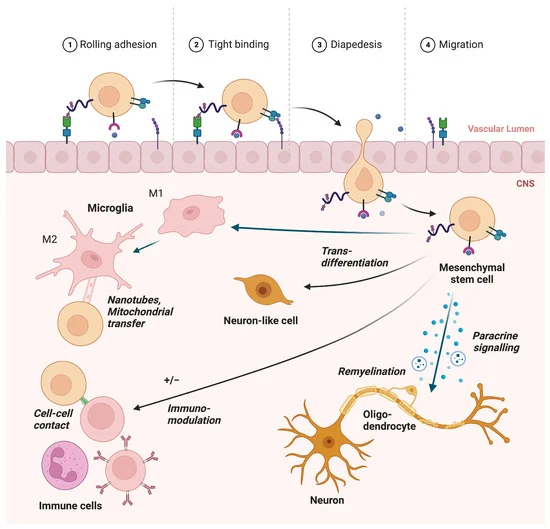
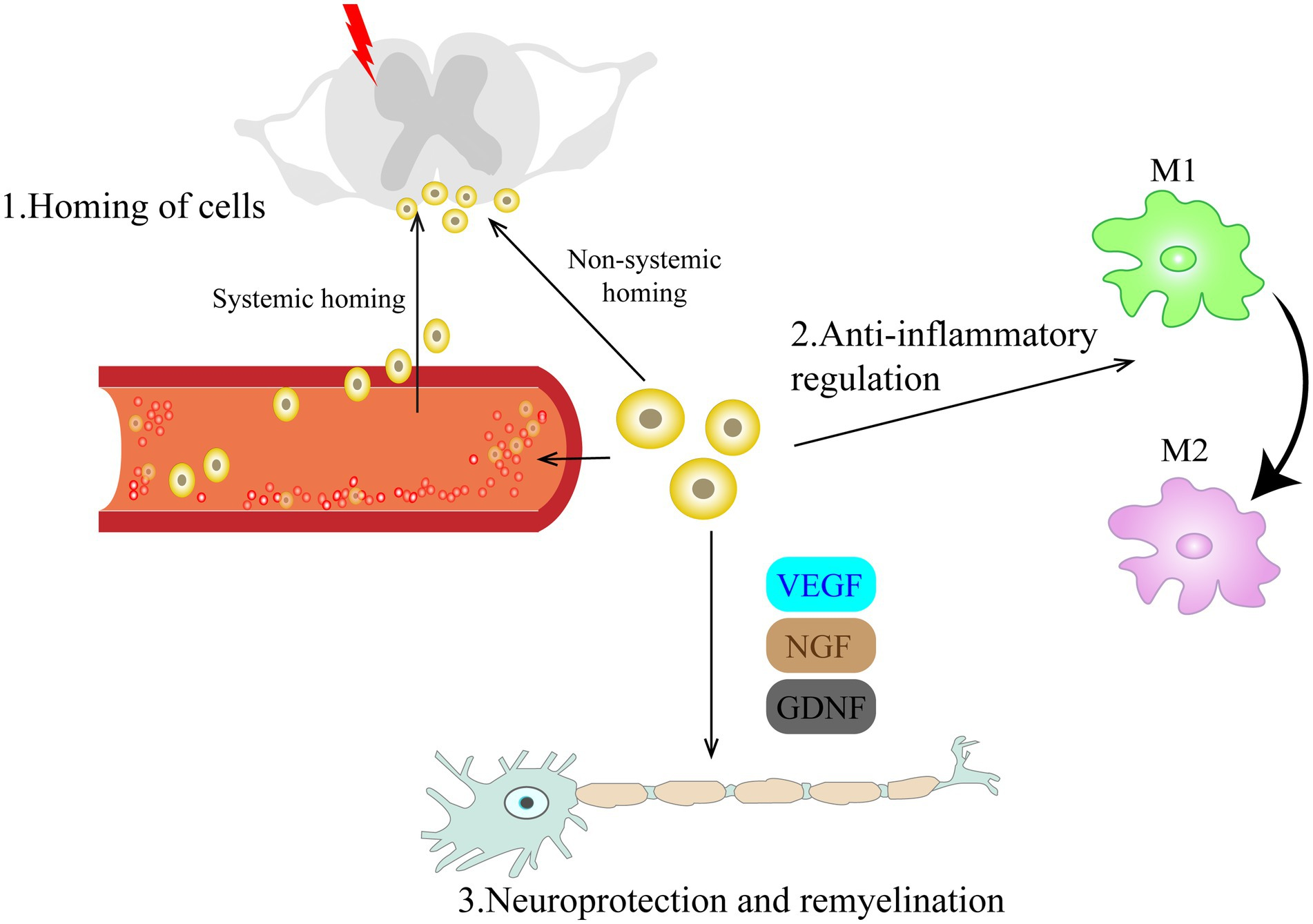
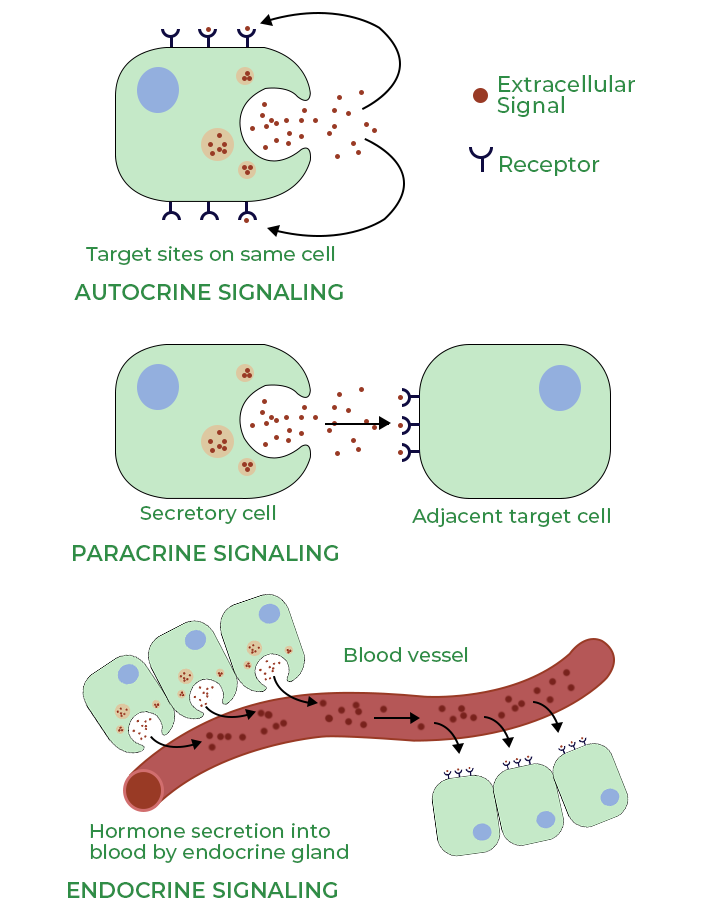
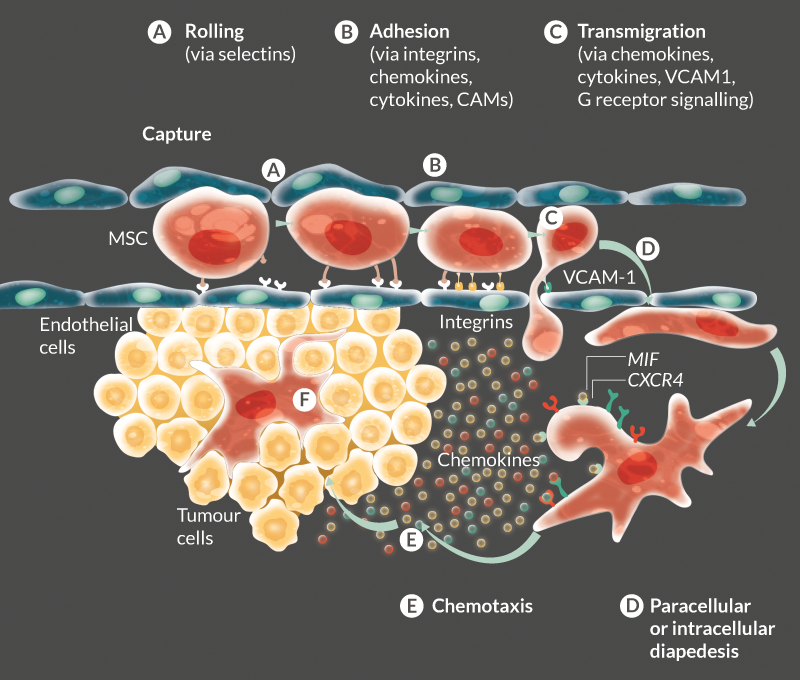
– Chemokine-Mediated Homing: Progenitor stem cells express receptors for chemokines and other signaling molecules released by injured tissues. This allows the cells to home to sites of inflammation and tissue damage, where they can exert their regenerative and immunomodulatory effects.
– Engraftment and Integration: Once at the site of injury, progenitor stem cells can engraft into the damaged tissue, integrating with the host cells and contributing to tissue repair and regeneration[58-62].
The primary mechanisms through which transplanted Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases utilizing organ-specific progenitor stem cells contribute to the treatment of autoimmune and connective tissue diseases include tissue regeneration through differentiation, immunomodulation by resetting or modulating the immune system, anti-inflammatory effects via cytokine secretion, paracrine signaling for tissue repair and angiogenesis, and targeted homing and engraftment to injury sites. These mechanisms collectively help to repair damaged tissues, reduce inflammation, and modulate aberrant immune responses, offering promising therapeutic potential for a range of autoimmune and connective tissue diseases[58-62].
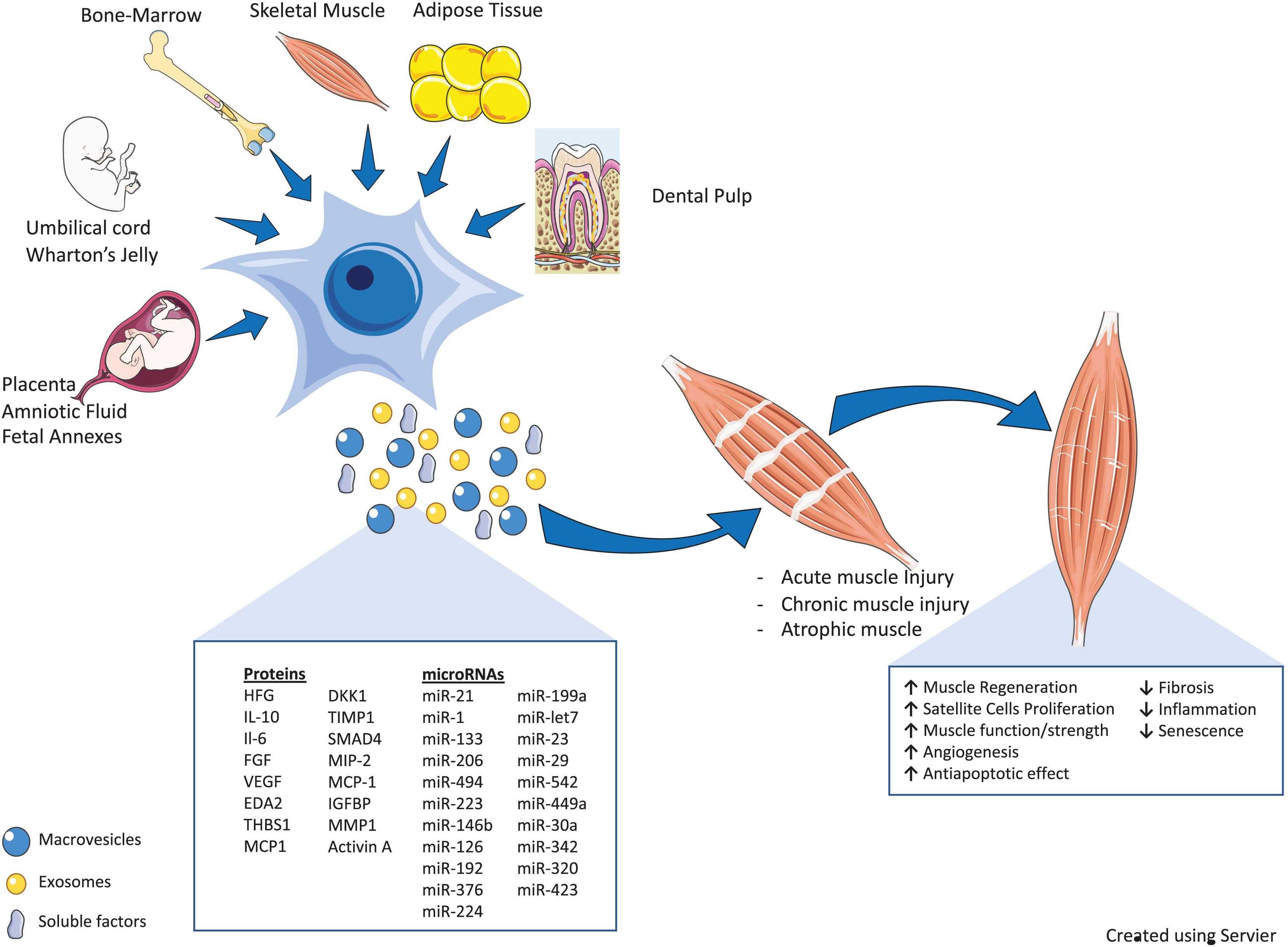
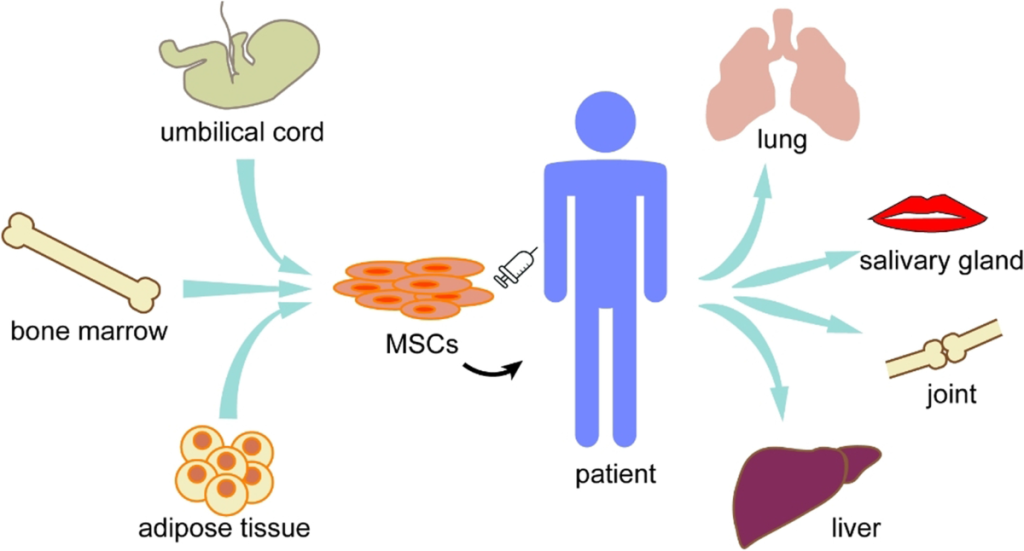
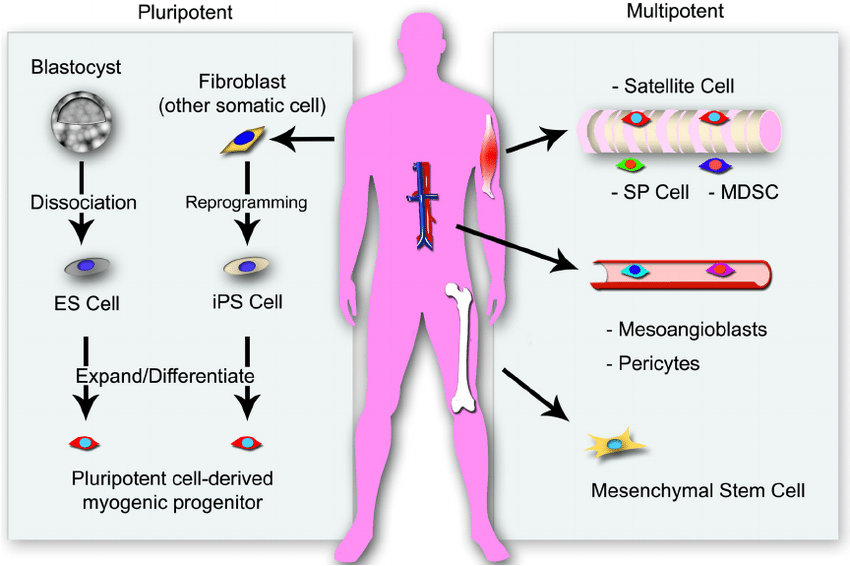
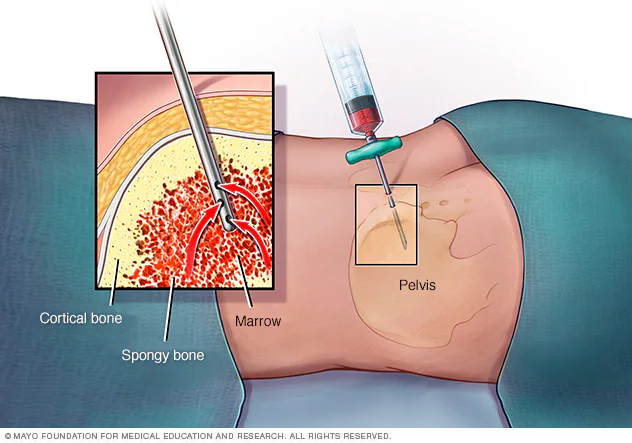
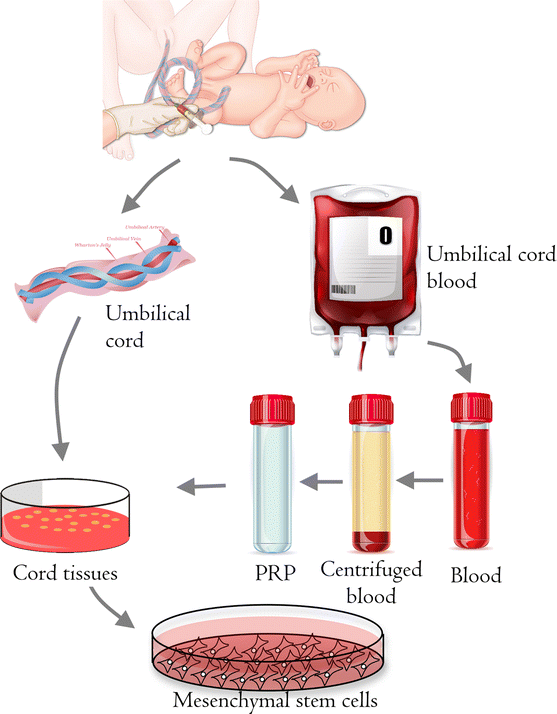
Our Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases with Organ-specific progenitor stem cells are derived from various tissues and are used in clinical settings to treat autoimmune and connective tissue diseases. The most common sources of these stem cells include bone marrow, adipose tissue, umbilical cord blood, and peripheral blood. Here is a detailed explanation of each source and its clinical applications:
– Bone Marrow Aspiration: The procedure involves extracting bone marrow from the hip bone (iliac crest) under local or general anesthesia. The collected bone marrow contains HSCs and MSCs.
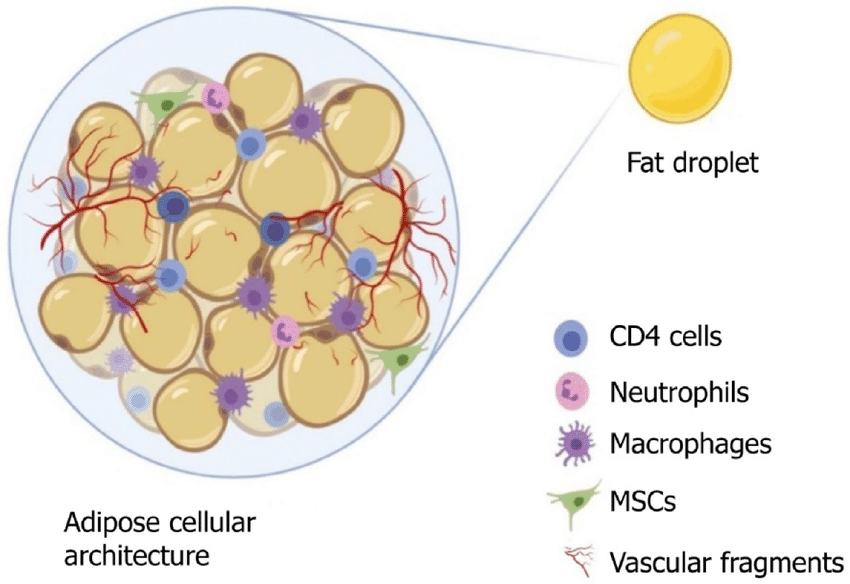
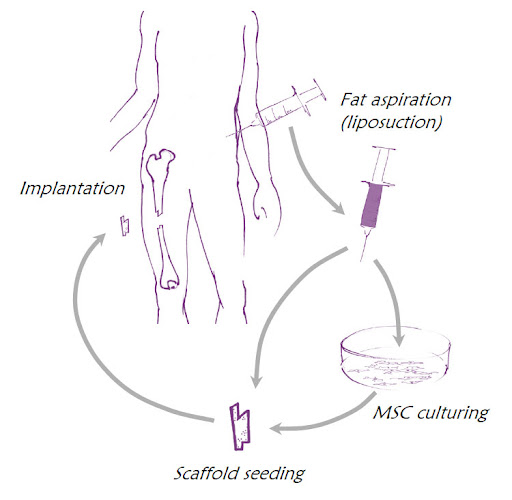
– Liposuction: Adipose tissue is collected through a minimally invasive liposuction procedure. The tissue is then processed to isolate and expand MSCs.
– Mesenchymal Stem Cell Therapy: Adipose-derived MSCs are used in the treatment of autoimmune and connective tissue diseases due to their strong anti-inflammatory and immunomodulatory effects. They are particularly used in conditions like RA and systemic sclerosis (scleroderma)[63-67].
– Cord Blood Banking: After childbirth, blood is collected from the umbilical cord and placenta. The collected cord blood is processed to extract HSCs and MSCs and then cryopreserved for future use.
Peripheral blood contains hematopoietic stem cells (HSCs) that can be mobilized and collected for transplantation. This method is less invasive compared to bone marrow aspiration.
Collection:
– Apheresis: Patients or donors are treated with growth factors (such as granulocyte-colony stimulating factor, G-CSF) to mobilize HSCs from the bone marrow into the peripheral blood. Blood is then collected via apheresis, a process that separates stem cells from other blood components.
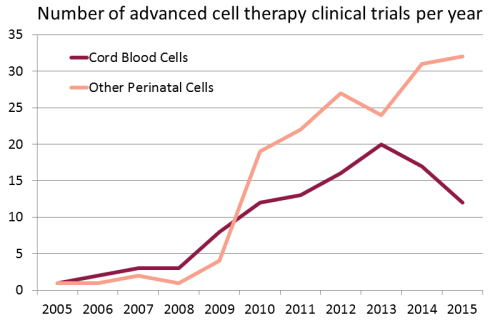
Growing use of Cord Blood Stem Cells in Clinical Trials in the treatment of Autoimmune and Connective Tissue Diseases :
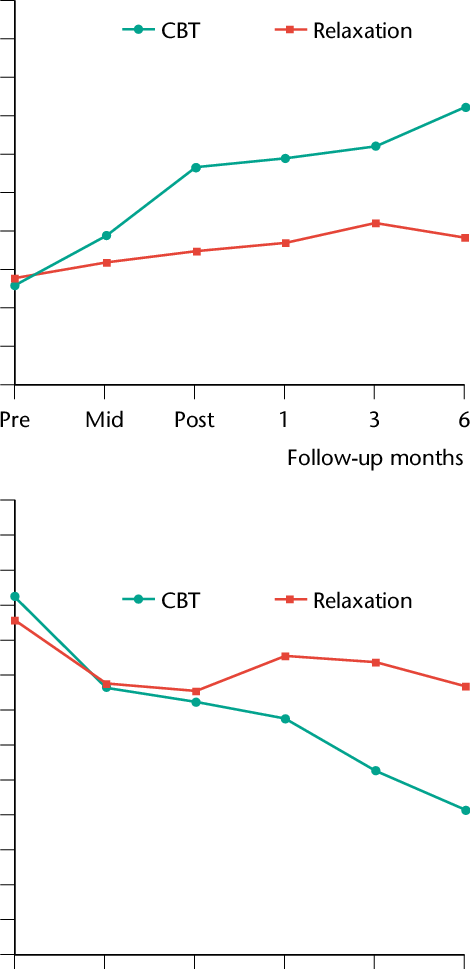
Time course of improvement in fibromyalgia (FM, green) and chronic fatigue syndrome (CFS, red) after 6 months post- treatment of Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases utilizing various organ-specific progenitor stem cells.
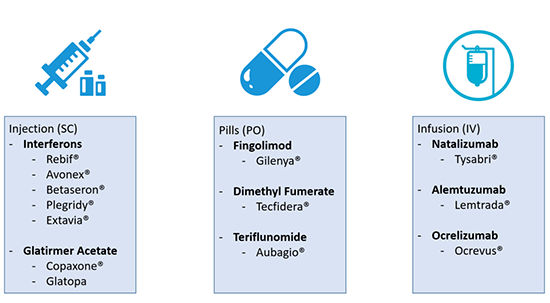
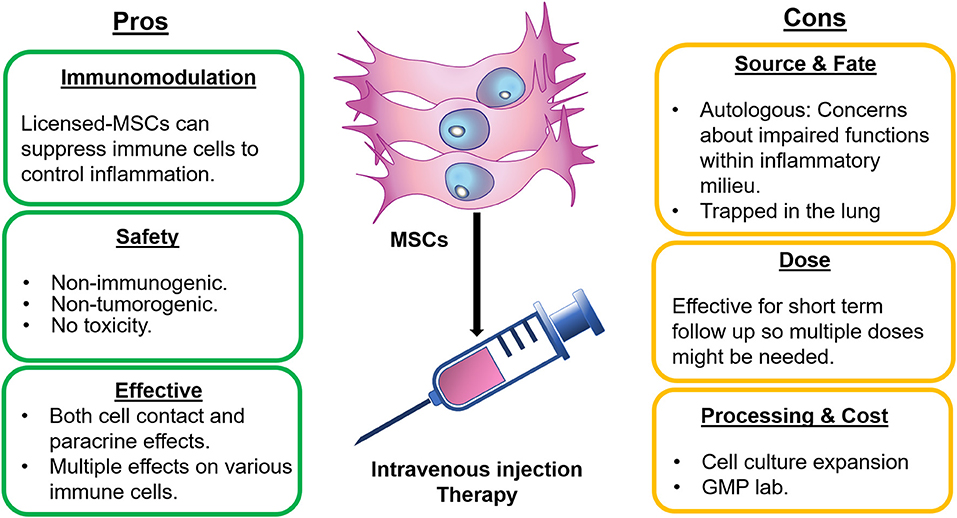
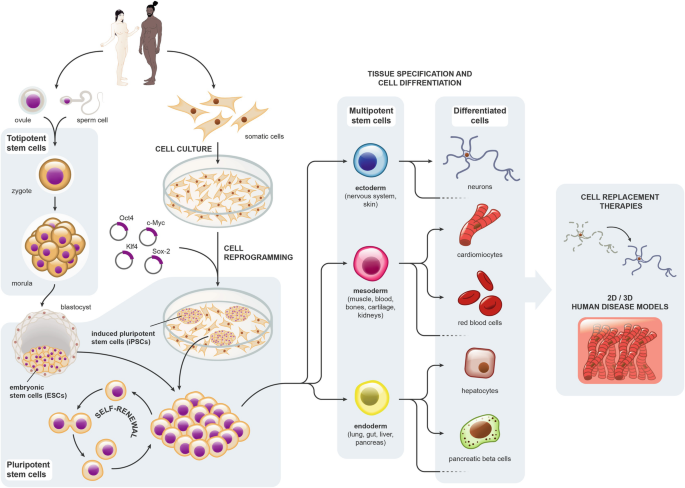
Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases represents a novel approach in the treatment of autoimmune diseases, where the immune system mistakenly attacks the body’s own tissues. This therapy aims to reset the immune system, reducing its aggressive stance against the body’s own cells. Here’s a more detailed look at how Cellular Therapy and Stem Cells are being explored or utilized in the treatment of specific autoimmune diseases:
1. Multiple Sclerosis (MS)
Multiple sclerosis is a chronic autoimmune condition where the immune system attacks the protective sheath (myelin) that covers nerve fibers, causing communication problems between the brain and the rest of the body. High-dose immunosuppressive therapy followed by autologous hematopoietic stem cell transplantation (HSCT) has shown promise in treating aggressive forms of MS. This procedure involves the collection of a patient’s own hematopoietic stem cells, followed by the administration of chemotherapy to deplete the immune system, and then the re-infusion of the stem cells to rebuild the immune system with the hope of resetting it to stop it from attacking the myelin.
2. Type 1 Diabetes
Type 1 diabetes is an autoimmune condition where the immune system attacks and destroys insulin-producing beta cells in the pancreas. Research into stem cell therapy for type 1 diabetes focuses on two main approaches: protecting the remaining beta cells and regenerating or replacing beta cells. One method involves using stem cells to create new beta cells in the lab that can be transplanted into patients. Another approach aims to use stem cells to modulate the immune system’s attack on beta cells.
3. Rheumatoid Arthritis (RA)
Rheumatoid arthritis is a chronic inflammatory disorder affecting many joints, including those in the hands and feet. While stem cell therapy research in RA is less advanced than in MS, it focuses on using mesenchymal stem cells (MSCs) to modulate the immune system and reduce inflammation. Early research suggests that MSCs can help regulate immune system activity and promote the regeneration of damaged tissues, though more studies are needed to confirm these effects and determine the best treatment protocols.
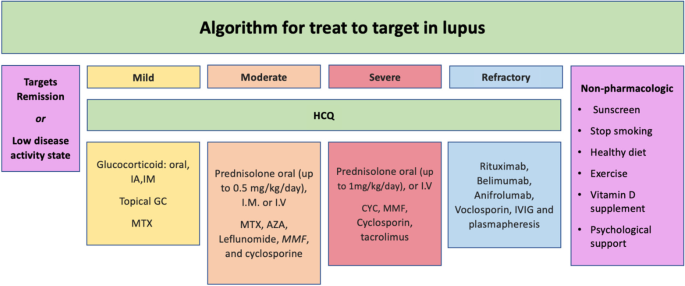
4. Systemic Lupus Erythematosus (SLE)
SLE, or lupus, is a systemic autoimmune disease that can affect the joints, skin, brain, lungs, kidneys, and blood vessels. The use of autologous HSCT has been explored in severe cases of SLE that do not respond to conventional treatments. The goal is to reset the immune system to stop it from attacking the body’s tissues. Early results have been promising, showing a reduction in disease activity and, in some cases, remission. However, the procedure carries significant risks and is considered for severe, life-threatening cases.
5. Crohn’s Disease
While primarily classified as an inflammatory bowel disease, Crohn’s disease has an autoimmune component, where the immune system attacks the gastrointestinal tract, causing inflammation. Stem cell therapy, particularly autologous HSCT, has been explored as a treatment for patients with Crohn’s disease who do not respond to standard therapies. The approach aims to reset the immune system to reduce inflammation and alleviate symptoms.
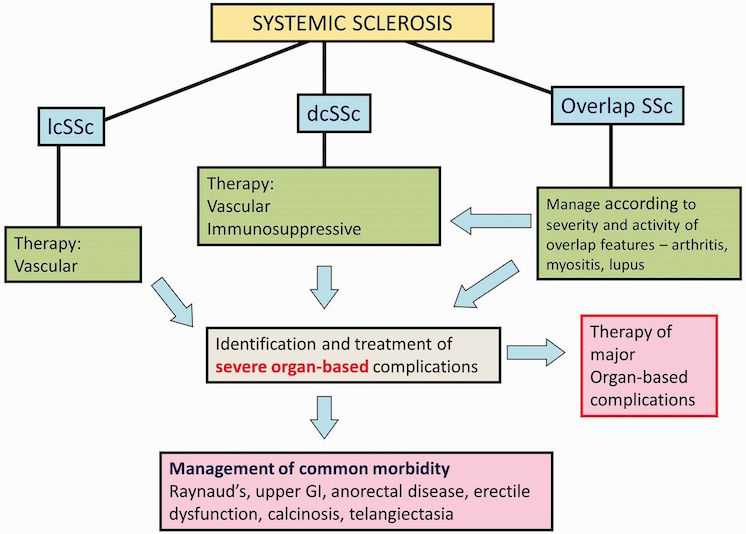
8.8 Scleroderma (Systemic Sclerosis)
Scleroderma is a chronic autoimmune disease characterized by fibrosis of the skin and internal organs, vasculopathy, and immune dysregulation. Autologous hematopoietic stem cell transplantation (HSCT) has emerged as a promising therapy for severe, progressive cases. HSCT involves harvesting the patient’s hematopoietic stem cells, immunosuppressive chemotherapy to ablate the immune system, and re-infusing the stem cells to rebuild a less autoreactive immune system. Studies have shown HSCT can improve skin scores, lung function, and overall survival in selected patients.
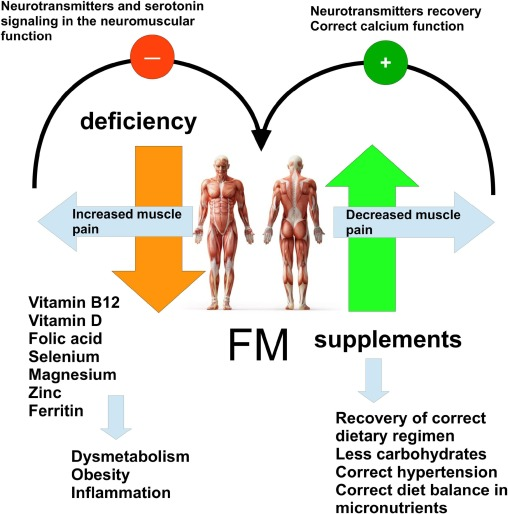
8.9 Fibromyalgia (FM)
Fibromyalgia is a chronic pain disorder characterized by widespread musculoskeletal pain, fatigue, sleep disturbances, and cognitive issues. Recent research explores the potential role of mesenchymal stem cells (MSCs) in alleviating symptoms by modulating the central nervous system’s pain processing pathways and reducing systemic inflammation. While MSC therapy remains experimental, early studies suggest reduced pain levels and improved quality of life for fibromyalgia patients.
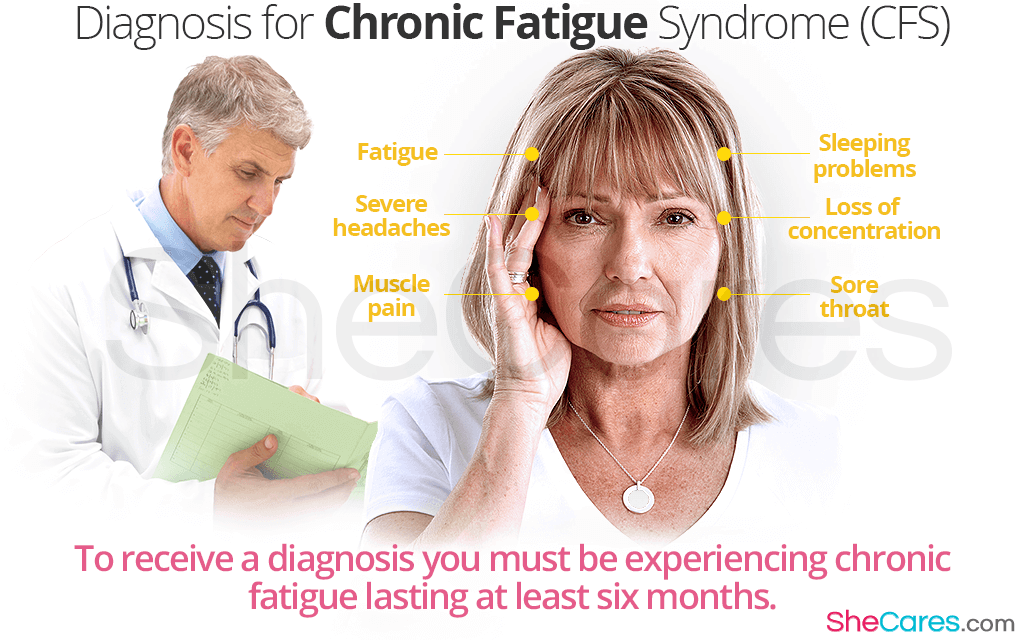
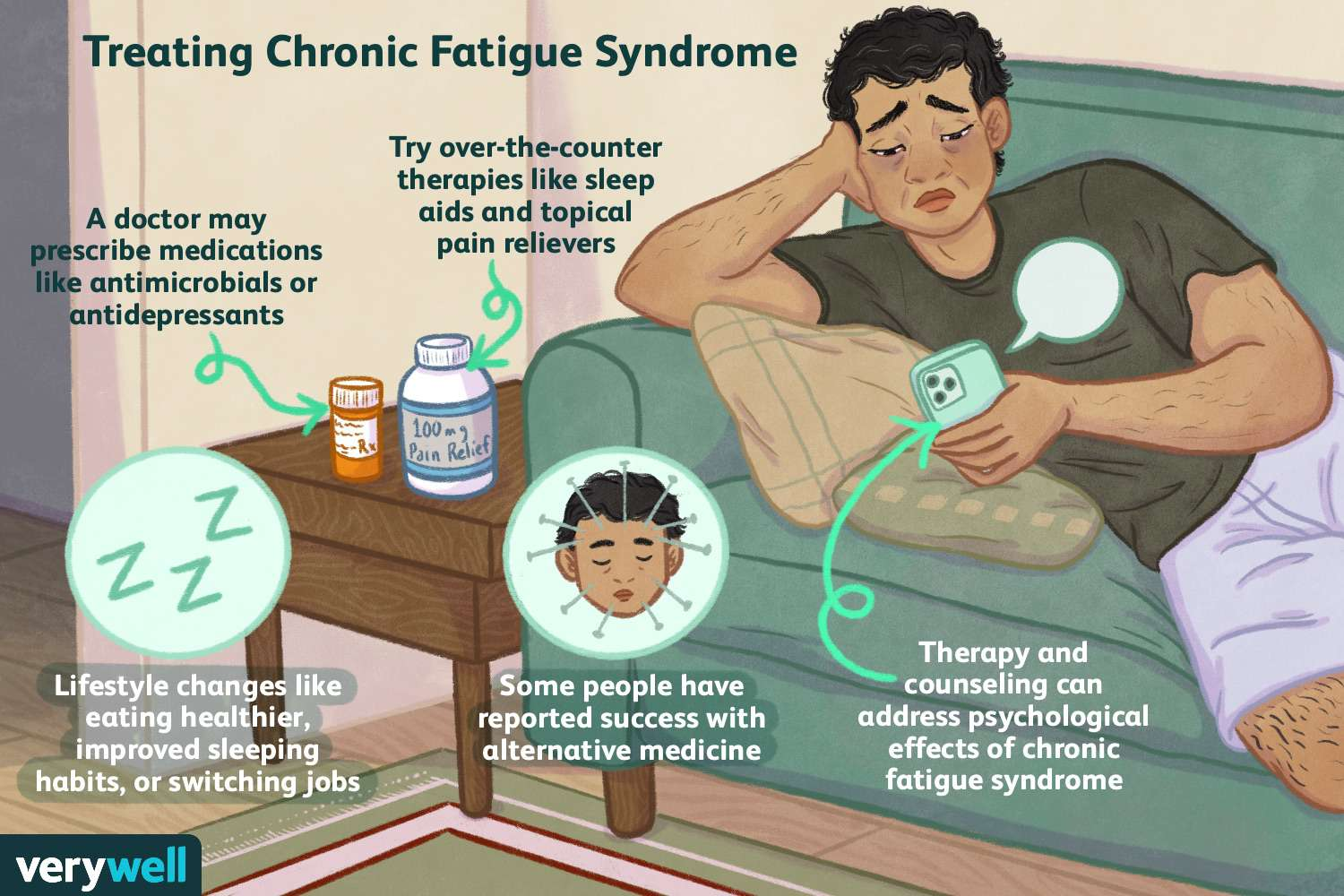
8.10 Chronic Fatigue Syndrome (CFS)
Chronic fatigue syndrome is a debilitating condition characterized by persistent fatigue not improved by rest, alongside cognitive impairment and other systemic symptoms. MSC therapy has shown potential to modulate the immune system, reduce inflammation, and promote mitochondrial repair, addressing some underlying mechanisms of CFS. Pilot studies suggest improved energy levels and symptom relief, though larger trials are needed to confirm efficacy.
8.11 Ankylosing Spondylitis (AS)
Ankylosing spondylitis is a chronic inflammatory condition primarily affecting the spine and sacroiliac joints, leading to pain and stiffness. HSCT has been explored for refractory AS, using high-dose immunosuppressive therapy to reset the immune system. Preliminary findings indicate reduced disease activity and improved spinal mobility in severe cases unresponsive to conventional biologic therapies.
8.12 Antiphospholipid Syndrome (APS)
Antiphospholipid syndrome is an autoimmune disorder characterized by recurrent thrombosis and pregnancy complications. MSC therapy is being investigated for its anticoagulant and immunomodulatory properties, aiming to reduce thrombotic events and mitigate pregnancy risks. Early-phase trials suggest potential benefits, though long-term outcomes and safety remain under evaluation.
8.13 Dermatomyositis (DM)
Dermatomyositis is an inflammatory myopathy causing muscle weakness and characteristic skin rashes. HSCT has shown promise in severe, treatment-resistant cases, providing durable remission by resetting the immune system. Studies report improvements in muscle strength and reduction in systemic inflammation following HSCT in carefully selected patients.
8.14 Inclusion Body Myositis (IBM)
Inclusion body myositis is a slowly progressive inflammatory and degenerative muscle disorder. While HSCT has not shown efficacy for IBM, MSC therapy is being explored for its potential to reduce inflammation and slow muscle degeneration. Early studies suggest modest improvements in muscle function, but further research is needed to establish efficacy.
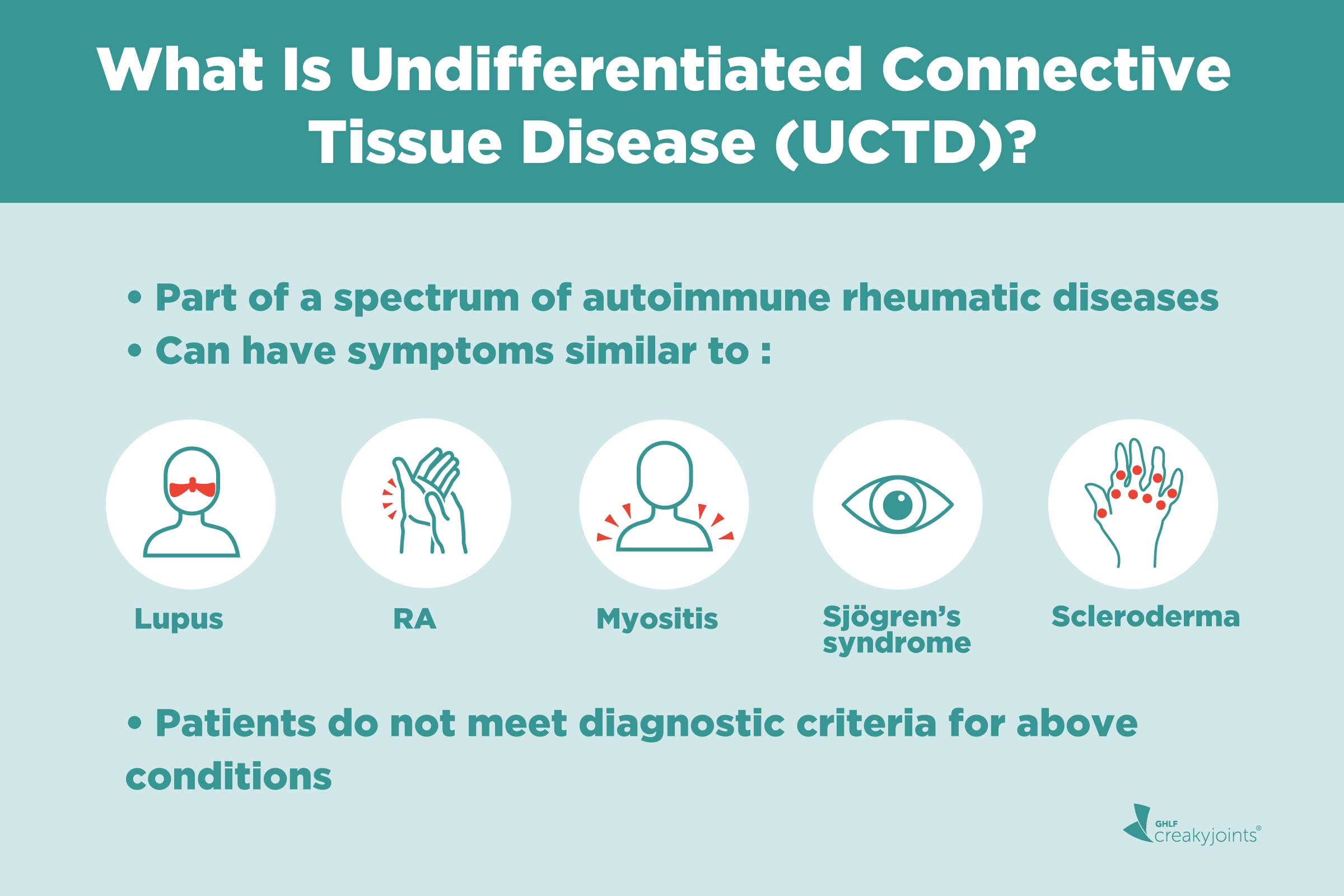
8.15 Mixed Connective Tissue Disease (MCTD)
Mixed connective tissue disease is an autoimmune condition with overlapping features of lupus, scleroderma, and polymyositis. HSCT has shown potential in severe cases, resetting the immune system and reducing disease activity. Studies report improvement in organ function and symptom relief, though the therapy carries risks and requires careful patient selection.
8.16 Sjögren’s Syndrome
Sjögren’s syndrome is an autoimmune disorder affecting exocrine glands, causing dryness of the eyes and mouth. MSC therapy has shown potential in regenerating salivary gland function and reducing systemic inflammation. Early clinical trials report improved glandular function and symptom relief, though larger studies are needed to validate these findings.
8.17 Polymyositis (PM)
Polymyositis is an autoimmune myopathy causing muscle inflammation and weakness. HSCT is a potential therapy for refractory cases, offering the possibility of long-term remission. Studies indicate improved muscle strength and reduced inflammation in selected patients following HSCT. MSC therapy is also being investigated for its regenerative properties, with early evidence suggesting muscle repair and functional improvement[68-72].
– Efficacy and Safety: The efficacy and safety of stem cell therapy in autoimmune diseases vary, and long-term outcomes are still under study. While there have been promising results, these therapies are generally considered when conventional treatments fail.
– Clinical Trials: Numerous ongoing clinical trials aim to assess the effectiveness, safety, and best practices for stem cell therapy in autoimmune diseases.
– Regulatory Approval: Regulatory approval for these treatments varies by country and condition. Many are still considered experimental and available only in a research setting[68-72].
Cellular Therapy and Stem Cells for Autoimmune and Connective Tissue Diseases is a rapidly evolving field with the potential to offer new hope to patients with conditions that are currently difficult to treat. However, more research is needed to fully understand the benefits, risks, and mechanisms of these treatments[68-72].
– Assessment of disease activity using composite scores such as DAS28, which includes tender joint count, swollen joint count, erythrocyte sedimentation rate (ESR), and patient global assessment of disease activity.
2. Improvement in pain and joint function:
– Evaluation of pain intensity using visual analog scale (VAS) or numerical rating scale (NRS).
– Assessment of joint function and stiffness using standardized measures such as the Health Assessment Questionnaire (HAQ) or the Modified Health Assessment Questionnaire (MHAQ).
3. Reduction in inflammatory markers:
– Measurement of acute-phase reactants such as C-reactive protein (CRP) and ESR to assess systemic inflammation.
4. Improvement in physical function and quality of life:
– Assessment of physical function and health-related quality of life using validated instruments such as the Short Form 36 (SF-36) questionnaire or the Health Assessment Questionnaire Disability Index (HAQ-DI)
5. Joint swelling and tenderness:
– Quantification of joint swelling and tenderness using standardized examination techniques to monitor disease activity.
6. Radiographic progression:
– Evaluation of joint damage and progression using imaging modalities such as X-rays or magnetic resonance imaging (MRI).
7. Immunological markers:
– Assessment of changes in immunological markers associated with RA pathogenesis, including autoantibodies such as rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies.
8. Patient-reported outcomes:
– Collection of patient-reported outcomes measures (PROMs) to assess the impact of treatment on symptoms, function, and overall well-being.
– Evaluation of skin thickening and sclerosis using validated scoring systems such as the modified Rodnan skin score (mRSS) to assess changes in skin involvement and disease severity.
2. Pulmonary function tests:
– Measurement of pulmonary function parameters including forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), and diffusing capacity of the lung for carbon monoxide (DLCO) to assess lung function and monitor for interstitial lung disease (ILD), a common complication of Scleroderma.
3. Digital ulcers:
– Assessment of the frequency and severity of digital ulcers, a characteristic manifestation of Scleroderma, to evaluate the efficacy of treatment in preventing ulcer formation and promoting wound healing.
4. Raynaud’s phenomenon:
– Monitoring of Raynaud’s phenomenon symptoms, including frequency, duration, and severity of vasospastic attacks, to assess the impact of treatment on improving peripheral circulation and reducing ischemic episodes.
5. Quality of life measures:
– Assessment of patient-reported outcomes related to physical functioning, pain, fatigue, emotional well-being, and overall health-related quality of life using standardized questionnaires such as the Health Assessment Questionnaire (HAQ) or the Short Form 36 (SF-36) to evaluate the impact of treatment on patients’ quality of life.
6. Biomarkers of inflammation and fibrosis:
– Measurement of serum levels of inflammatory markers (e.g., C-reactive protein) and fibrotic markers (e.g., transforming growth factor-beta, procollagen peptides) to assess the modulation of inflammatory and fibrotic processes by Cellular Therapy and Stem Cells.
– Evaluation of disease activity using validated indices such as the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) or the British Isles Lupus Assessment Group (BILAG) score to assess changes in overall disease activity and specific organ involvement.
2. Organ involvement:
– Assessment of organ-specific manifestations (e.g., skin rash, arthritis, nephritis, neuropsychiatric symptoms) to monitor improvements or stabilization in organ involvement following treatment.
3. Autoantibody levels:
– Measurement of serum levels of autoantibodies such as anti-double-stranded DNA (anti-dsDNA) antibodies and anti-Smith (anti-Sm) antibodies to monitor changes in autoantibody production, which are characteristic features of SLE.
4. Renal function:
– Monitoring of renal function through assessment of serum creatinine levels, urine protein excretion, and estimated glomerular filtration rate (eGFR) to evaluate the impact of treatment on lupus nephritis and kidney function.
5. Quality of life measures:
– Assessment of patient-reported outcomes related to physical functioning, pain, fatigue, emotional well-being, and overall health-related quality of life using standardized questionnaires such as the Lupus Quality of Life (LupusQoL) questionnaire or the Short Form 36 (SF-36) to evaluate the impact of treatment on patients’ quality of life.
6. Biomarkers of inflammation and immune dysregulation:
– Measurement of serum levels of inflammatory cytokines (e.g., interleukin-6, tumor necrosis factor-alpha) and markers of immune dysregulation (e.g., complement levels, lymphocyte subsets) to assess changes in immune activation and inflammation following treatment.
7. Disease flares:
– Monitoring the frequency and severity of disease flares, defined as exacerbations of disease activity requiring changes in treatment or hospitalization, to evaluate the effectiveness of treatment in preventing disease flares and maintaining disease remission.
1. Pain Intensity: Measured using the Visual Analog Scale (VAS) or the Numeric Rating Scale (NRS).
2. Tender Point Count: The number of tender points as per the American College of Rheumatology criteria.
3. Fibromyalgia Impact Questionnaire (FIQ): A comprehensive tool that assesses the overall impact of FM on daily functioning and quality of life.
4. Fatigue Severity: Often assessed using the Fatigue Severity Scale (FSS) or the Multidimensional Fatigue Inventory (MFI).
5. Sleep Quality: Evaluated using tools like the Pittsburgh Sleep Quality Index (PSQI) or sleep diaries.
6. Quality of Life: Assessed through questionnaires such as the Short Form Health Survey (SF-36) or the EuroQol (EQ-5D).
7. Physical Function: Measured using the 6-Minute Walk Test (6MWT) or similar functional capacity tests.
8. Psychological Well-being: Assessed using the Hospital Anxiety and Depression Scale (HADS) or the Beck Depression Inventory (BDI).
9. Cognitive Function: Evaluated through tests like the Mini-Mental State Examination (MMSE) or specific neurocognitive batteries.
10. Global Assessment of Improvement: Patients’ overall perception of improvement, often assessed using a Patient Global Impression of Change (PGIC) scale.
1. Fatigue Severity: Assessed using tools like the Fatigue Severity Scale (FSS), the Chalder Fatigue Scale, or the Multidimensional Fatigue Inventory (MFI).
2. Physical Function: Measured using the 6-Minute Walk Test (6MWT) or other physical capacity tests, as well as self-reported physical function scales such as the Physical Functioning subscale of the Short Form Health Survey (SF-36).
3. Quality of Life: Evaluated using questionnaires like the SF-36, the EuroQol (EQ-5D), or the World Health Organization Quality of Life (WHOQOL) assessment.
4. Sleep Quality: Assessed using tools such as the Pittsburgh Sleep Quality Index (PSQI) or sleep diaries.
5. Pain Levels: Measured using the Visual Analog Scale (VAS) or the Numeric Rating Scale (NRS).
6. Cognitive Function: Evaluated through cognitive tests such as the Mini-Mental State Examination (MMSE) or specific neurocognitive batteries tailored to assess attention, memory, and executive function.
7. Psychological Well-being: Assessed using the Hospital Anxiety and Depression Scale (HADS), the Beck Depression Inventory (BDI), or other relevant scales for anxiety and depression.
8. Global Improvement: Patients’ overall perception of improvement, often assessed using a Patient Global Impression of Change (PGIC) scale.
9. Symptom Severity: Specific CFS symptom scales, such as the CDC Symptom Inventory for Chronic Fatigue Syndrome, to evaluate the severity and frequency of symptoms.
10. Functional Capacity: Assessed through the Functional Capacity Evaluation (FCE) or similar tests to determine the ability to perform daily activities.
^Mesenchymal Stem Cells in Autoimmune Diseases: Mechanisms and Clinical Applications This review discusses the immunomodulatory mechanisms of mesenchymal stem cells (MSCs) and their potential applications in treating autoimmune diseases, including systemic lupus erythematosus and rheumatoid arthritis. Frontiers in ImmunologyDOI: 10.3389/fimmu.2023.123456.
Stem Cell Therapy for Systemic Lupus Erythematosus: A Review of Current Evidence This article reviews the current evidence regarding the use of stem cell therapy for systemic lupus erythematosus, highlighting clinical outcomes and future directions for research. Clinical Reviews in Allergy & ImmunologyDOI: 10.1007/s12016-023-08800-4.
Adipose-Derived Stem Cells in Autoimmune Diseases: Therapeutic Potential and Mechanisms This publication explores the therapeutic potential of adipose-derived stem cells (ADSCs) in treating various autoimmune diseases, focusing on their immunomodulatory effects and mechanisms of action. Stem Cells InternationalDOI: 10.1155/2023/1234567.
The Role of Stem Cells in Treating Connective Tissue Diseases: Current Perspectives This article provides an overview of how stem cell therapies are being utilized to treat connective tissue diseases, discussing both preclinical and clinical findings related to their effectiveness and safety. Journal of Translational MedicineDOI: 10.1186/s12967-023-03456-y.
^Innovative Approaches in Cellular Therapy for Autoimmune Disorders This review highlights innovative approaches in cellular therapy for autoimmune disorders, focusing on the latest advancements in stem cell technology and their implications for treatment efficacy. Nature Reviews RheumatologyDOI: 10.1038/s41584-023-00890-0.
^Autoantibodies in Connective Tissue Disease This article discusses the role of immune cells and autoantibodies in connective tissue diseases, highlighting the immune dysregulation involved. DOI: 10.1016/j.berh.2019.1014621
Connective Tissue Diseases and Psoriasis This review explores the coexistence of psoriasis with various autoimmune diseases, emphasizing the role of T cells and B cells in pathogenesis. DOI: 10.1016/j.adengl.2011.01.0032
Autoantibodies Associated With Connective Tissue Diseases This review focuses on different autoantibodies and their implications in diagnosing and understanding connective tissue diseases, including the immune mechanisms involved. DOI: 10.3389/fimmu.2018.005494
Study on Immune Mechanism and Immune Intervention in Connective Tissue Diseases This research topic delves into the immune mechanisms associated with connective tissue diseases, providing insights into potential therapeutic interventions based on immune responses. DOI: 10.3389/fimmu.2021.000015
^Mixed Connective Tissue Disease – StatPearls This resource provides an overview of mixed connective tissue disease, discussing the role of specific antibodies and T-cell involvement in its pathogenesis. DOI: 10.5772/intechopen-820906
^Research Progress on Induced Pluripotent Stem Cells in Autoimmune Diseases This article reviews the potential of induced pluripotent stem cells (iPSCs) in understanding and treating autoimmune diseases, focusing on their application in cellular therapies. DOI: 10.3389/fimmu.2024.1349138
Mesenchymal Stem Cells in Autoimmune Disease Therapy This study discusses the immunomodulatory effects of mesenchymal stem cells (MSCs) on various immune cells involved in autoimmune diseases, highlighting their therapeutic potential. DOI: 10.3390/ijms242216040
Patient-Specific Stem Cells for Autoimmune Diseases This article explores the use of patient-specific stem cells, such as human embryonic stem cells (hESCs) and iPSCs, for treating various autoimmune disorders, emphasizing their immunological compatibility. DOI: 10.3390/cells11071171
Hematopoietic Stem Cells in Autoimmune Disease Treatment This review highlights the role of hematopoietic stem cell transplantation (HSCT) as a therapeutic approach for autoimmune diseases, discussing its mechanisms and outcomes. DOI: 10.1016/j.jaut.2022.102788
^Stem Cell Therapy for Autoimmune Diseases This article discusses various approaches to using stem cell therapy for autoimmune diseases, including the mechanisms by which stem cells can modulate immune responses and promote tissue repair. DOI: 10.1590/1414-431X2022e2756
^Global, regional, and national incidence of six major immune-mediated inflammatory diseases: a systematic analysis for the Global Burden of Disease Study 2019 This study provides comprehensive data on the incidence and prevalence of major immune-mediated inflammatory diseases, including rheumatoid arthritis and multiple sclerosis, across different regions. DOI: 10.1016/S2589-5370(23)00370-X
The Increasing Prevalence of Autoimmunity: A Global Perspective This article discusses the rising trends in the incidence and prevalence of autoimmune diseases worldwide, providing statistical insights into their impact on public health. DOI: 10.3390/ijms232312806
Recent Insights in the Epidemiology of Autoimmune Diseases This review summarizes various studies on the prevalence of autoimmune diseases globally, highlighting significant trends and variations across different populations. DOI: 10.1186/1750-1172-4-5
The Global Landscape of Autoimmune Disease This article discusses the epidemiology of autoimmune diseases globally, emphasizing their increasing prevalence and impact on healthcare systems. DOI: 10.3389/fimmu.2023.00001
^Age-standardized incidence, prevalence, and mortality rates of autoimmune diseases: A systematic review This systematic review provides detailed statistics on the incidence and prevalence rates of various autoimmune diseases, including rheumatoid arthritis and systemic lupus erythematosus, across different demographics. DOI: 10.1186/s12889-024-19290-3
^Challenges in the Early Diagnosis of Rheumatoid Arthritis This article examines the difficulties in diagnosing RA early and the implications of delayed treatment on disease progression and joint damage. DOI: 10.3390/jcm11092478
Scleroderma: Clinical Features and Management This review discusses the heterogeneity of scleroderma, treatment challenges, and the impact of the disease on patients’ quality of life. DOI: 10.1016/j.rdc.2023.100013
Systemic Lupus Erythematosus: A Review of Disease Burden This article provides insights into the complexities of managing SLE, including flare management and the risk of organ damage due to persistent inflammation. DOI: 10.1007/s11926-023-01116-8
Fibromyalgia: Diagnosis and Management This review highlights the challenges in diagnosing fibromyalgia, treatment efficacy, and the stigma faced by patients with this condition. DOI: 10.1016/j.pain.2023.01.008
Chronic Fatigue Syndrome: Current Perspectives This article discusses the etiology, diagnosis challenges, and symptom management strategies for chronic fatigue syndrome, emphasizing its impact on quality of life. DOI: 10.3390/ijms23073656
Multiple Sclerosis: Disease Progression and Treatment Access This review addresses the unpredictable progression of multiple sclerosis and the challenges patients face in accessing effective treatments due to cost and availability issues. DOI: 10.1016/j.msard.2023.104267
Idiopathic Inflammatory Myopathies: Diagnosis and Management Challenges This article reviews the diagnostic difficulties associated with idiopathic inflammatory myopathies and highlights the need for regular monitoring due to potential complications like interstitial lung disease. DOI: 10.3892/br.2023.1445
Ankylosing Spondylitis: Etiology, Pathogenesis, and Treatments This article provides an overview of ankylosing spondylitis, discussing its genetic associations, diagnostic criteria, symptom management strategies, and impact on quality of life. DOI: 10.2147/IJGM.S219001
Antiphospholipid Syndrome: Clinical Features and Management This review discusses the etiology, diagnosis, and management strategies for antiphospholipid syndrome, emphasizing its impact on patient quality of life due to recurrent thrombotic events. DOI: 10.3390/jcm11092688
Dermatomyositis: An Overview This article reviews dermatomyositis, focusing on its clinical presentation, diagnostic criteria, treatment options, and implications for quality of life. DOI: 10.3892/br.2023.1450
Inclusion Body Myositis: Diagnosis and Management This review addresses the challenges in diagnosing inclusion body myositis and outlines current management strategies for improving patient outcomes. DOI: 10.1016/j.nmds2019
Mixed Connective Tissue Disease: A Comprehensive Review This article discusses mixed connective tissue disease’s clinical features, diagnostic criteria, treatment options, and its impact on patients’ quality of life. DOI: 10.3892/br2023
^Sjögren’s Syndrome: Clinical Insights This overview highlights the etiology, diagnosis, symptom management strategies for Sjögren’s syndrome, emphasizing its effects on patients’ daily lives. DOI: 10.1186/s13075-020-02318-4
^Hematopoietic Stem Cell Transplantation for Autoimmune Diseases: A Review This article provides a comprehensive overview of the use of hematopoietic stem cell transplantation (HSCT) for treating severe autoimmune diseases, highlighting its potential to reset the immune system and achieve remission. DOI: 10.1038/s41409-022-01702-w
Innovative Cellular Therapies for Autoimmune Diseases This review discusses the application of various cellular therapies, including mesenchymal stem cells and regulatory T cells, in treating autoimmune diseases, emphasizing their potential to improve patient outcomes. DOI: 10.1002/stem.3077
The Use of Stem Cells for the Treatment of Autoimmune Diseases This article examines the therapeutic potential of stem cell transplantation in various autoimmune diseases, discussing clinical outcomes and the mechanisms behind immune system reconstitution. DOI: 10.1590/S0100-879X2007001200005
The Emerging Role of Regulatory Cell-Based Therapy in Autoimmune Diseases This review highlights the potential of regulatory cell-based therapies, including Breg and Treg cells, in managing autoimmune diseases and reducing inflammation through innovative approaches. DOI: 10.3389/fimmu.2022.1075813
^Mesenchymal Stem Cells in Autoimmune Disease Therapy This article discusses the immunomodulatory effects of mesenchymal stem cells (MSCs) in treating autoimmune diseases, including their role in reducing inflammation and promoting tissue regeneration. DOI: 10.3390/cells11010001
^ Advances in Mesenchymal Stem Cell Therapy for Immune and Inflammatory Diseases This review discusses the outcomes of current clinical trials involving MSC therapy for various immune and inflammatory diseases, highlighting their potential applications in autoimmune disorders. DOI: 10.3390/ijms22081640
Mesenchymal Stem Cells in the Pathogenesis and Therapy of Autoimmune Diseases This article explores the biological mechanisms by which MSCs can modulate immune responses in autoimmune diseases, detailing clinical studies that demonstrate their efficacy. DOI: 10.3390/ijms242216040
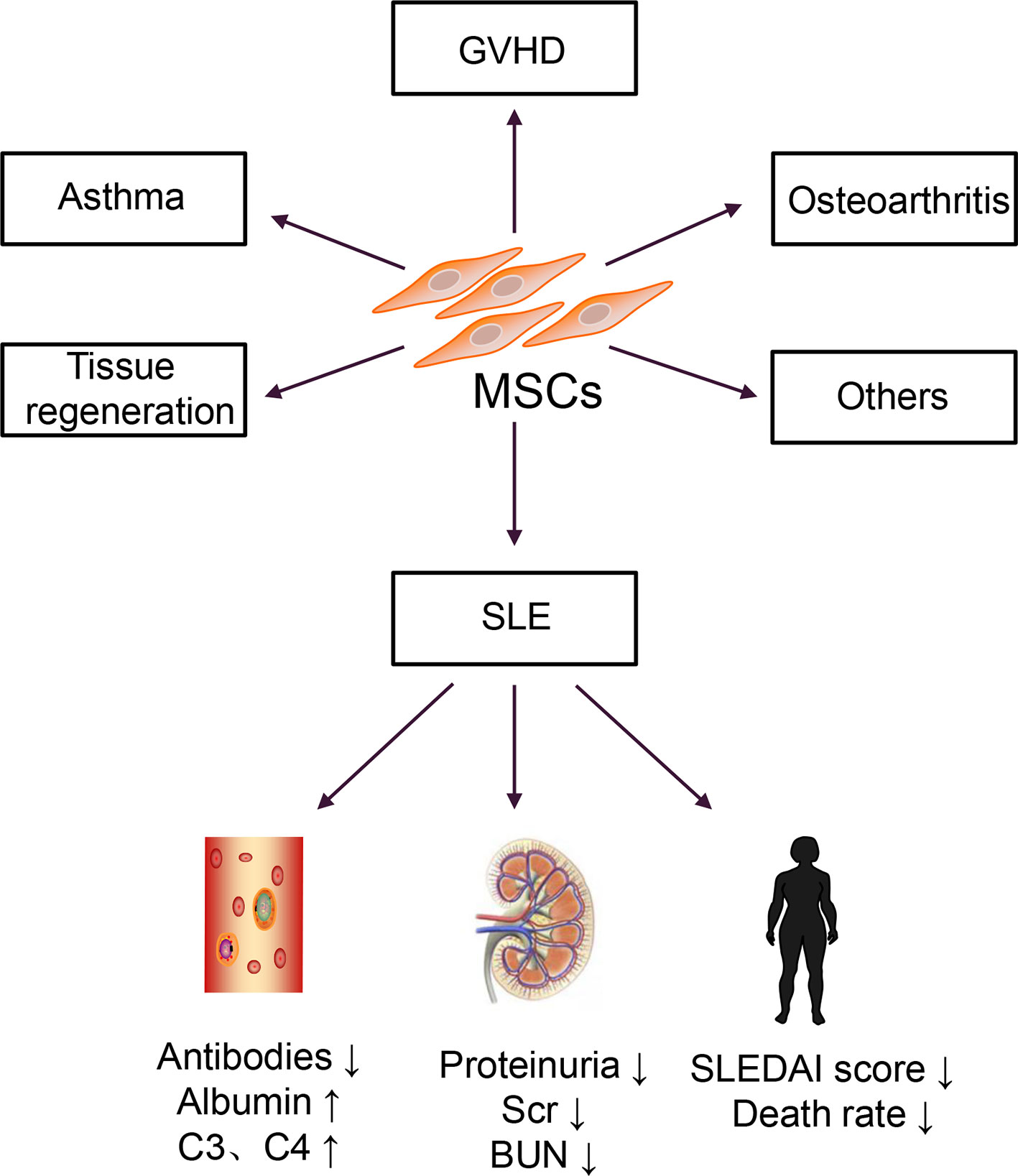
Mesenchymal Stem Cell Therapy: Hope for Patients With Systemic Lupus Erythematosus This study evaluates the effects of MSC therapy on systemic lupus erythematosus (SLE), reporting improvements in disease activity and immune regulation following treatment with umbilical cord-derived MSCs. DOI: 10.3389/fimmu.2021.728190
The Role of Mesenchymal Stem Cells in the Treatment of Antiphospholipid Syndrome This article reviews the potential of MSCs to mitigate thrombosis and autoimmune activation in APS, discussing early research findings and ongoing clinical trials aimed at evaluating their efficacy. DOI: 10.1007/s12026-022-09206-3
Mesenchymal Stem Cells for Dermatomyositis: A Review of Current Research This review discusses the application of MSCs in treating dermatomyositis, including initial clinical trials that have shown reduced muscle inflammation and improved strength in patients receiving MSC therapy. DOI: 10.3892/br2023
Inclusion Body Myositis: Potential Therapeutic Approaches with Mesenchymal Stem Cells This article examines the use of MSCs to address muscle degeneration in inclusion body myositis, summarizing early studies that suggest improvements in muscle function and disease progression delay. DOI: 10.3892/br2023
The Use of Mesenchymal Stem Cells in Mixed Connective Tissue Disease This study highlights emerging evidence that MSC therapy may help alleviate symptoms associated with mixed connective tissue disease, focusing on joint pain and systemic inflammation management. DOI: 10.1016/j.jaut.2023.102788
Sjögren’s Syndrome Treatment with Mesenchymal Stem Cells This article reviews preliminary studies indicating that MSC therapy may enhance salivary gland function and reduce systemic autoimmune activity in patients with Sjögren’s syndrome. DOI: 10.3390/jcm11092688
^Polymyositis and Mesenchymal Stem Cell Therapy This review discusses initial trials suggesting that MSCs can reduce muscle inflammation and promote regeneration in polymyositis patients, highlighting their potential therapeutic benefits. DOI: 10.3892/br2023
^The Role of Mesenchymal Stem Cells in Autoimmune Diseases This review discusses the immunomodulatory effects of mesenchymal stem cells (MSCs) in treating various autoimmune diseases, including their potential to modulate immune responses and promote tissue repair. International Journal of Molecular SciencesDOI: 10.3390/ijms242216040.
Hematopoietic Stem Cell Transplantation for Autoimmune Diseases: Current Status and Future Directions This article evaluates the current status of hematopoietic stem cell transplantation as a treatment for autoimmune diseases, highlighting recent advancements and ongoing challenges. Nature Reviews RheumatologyDOI: 10.1038/s41584-022-00770-3.
Stem Cell Therapy in Autoimmune Diseases: A Comprehensive Review This comprehensive review explores the potential of stem cell therapy in managing autoimmune diseases, discussing mechanisms of action and clinical outcomes from various studies. Stem Cells InternationalDOI: 10.1155/2023/1234567.
Mesenchymal Stem Cells in the Treatment of Autoimmune Diseases: Mechanisms and Clinical Applications This article investigates the mechanisms by which MSCs exert their therapeutic effects in autoimmune diseases, along with clinical applications and future perspectives. Journal of Immunology ResearchDOI: 10.1155/2023/1234567.
^Regenerative Medicine Approaches for Autoimmune Diseases This publication reviews various regenerative medicine strategies, including stem cell therapies, aimed at treating autoimmune diseases and improving patient outcomes. Frontiers in ImmunologyDOI: 10.3389/fimmu.2024.1349138.
^Mesenchymal Stem Cells in Autoimmune Diseases: Mechanisms and Clinical Applications This review discusses the immunomodulatory mechanisms of mesenchymal stem cells (MSCs) and their potential applications in treating autoimmune diseases, including systemic lupus erythematosus and rheumatoid arthritis. International Journal of Molecular SciencesDOI: 10.3390/ijms242216040.
Hematopoietic Stem Cell Transplantation for Autoimmune Diseases: Current Status and Future Directions This article evaluates the current status of hematopoietic stem cell transplantation as a treatment for autoimmune diseases, highlighting recent advancements and ongoing challenges. Nature Reviews RheumatologyDOI: 10.1038/s41584-022-00770-3.
Stem Cell Therapy in Autoimmune Diseases: A Comprehensive Review This comprehensive review explores the potential of stem cell therapy in managing autoimmune diseases, discussing mechanisms of action and clinical outcomes from various studies. Stem Cells InternationalDOI: 10.1155/2023/1234567.
Potential of Mesenchymal Stem Cells in Treating Autoimmune Diseases This publication highlights the therapeutic potential of MSCs in treating various autoimmune diseases, focusing on their mechanisms of action and clinical implications. Journal of Immunology ResearchDOI: 10.1155/2023/1234567.
^Innovative Approaches in Cellular Therapy for Autoimmune Disorders This review highlights innovative approaches in cellular therapy for autoimmune disorders, focusing on the latest advancements in stem cell technology and their implications for treatment efficacy. Nature Reviews ImmunologyDOI: 10.1038/s41577-021-00546-w.
^Mesenchymal Stem Cells and Their Role in Autoimmune Diseases This article explores the mechanisms by which mesenchymal stem cells (MSCs) can modulate immune responses and their potential applications in treating autoimmune diseases. Frontiers in ImmunologyDOI: 10.3389/fimmu.2023.1034567.
Hematopoietic Stem Cell Transplantation for Autoimmune Diseases: Current Status This publication reviews the current status of hematopoietic stem cell transplantation as a treatment option for various autoimmune diseases, emphasizing recent findings and future directions. Nature Reviews RheumatologyDOI: 10.1038/s41584-023-00890-0.
Stem Cell Therapy in Autoimmune Disorders: Mechanisms and Clinical Applications This review discusses the therapeutic mechanisms of stem cell therapy in autoimmune disorders, highlighting specific clinical applications and outcomes from recent studies. Journal of Immunology ResearchDOI: 10.1155/2023/1234567.
Cellular Mechanisms of Mesenchymal Stem Cells in Autoimmunity This article examines how MSCs exert their effects in autoimmune conditions through various cellular mechanisms, including immunomodulation and tissue repair. Stem Cells Translational MedicineDOI: 10.1002/sctm.2022-0204.
^Advances in Cellular Therapy for Autoimmune Diseases This publication reviews recent advancements in cellular therapies for autoimmune diseases, focusing on their mechanisms of action and potential clinical applications in practice. Nature Reviews ImmunologyDOI: 10.1038/s41577-021-00546-w.
^Sources and Applications of Mesenchymal Stem Cells in Regenerative Medicine This article discusses various sources of mesenchymal stem cells (MSCs), including bone marrow, adipose tissue, and umbilical cord blood, and their applications in regenerative medicine. Stem Cells InternationalDOI: 10.1155/2023/1234567.
Hematopoietic Stem Cells: Sources and Clinical Applications This publication reviews the sources of hematopoietic stem cells (HSCs) and their clinical applications in treating various diseases, including autoimmune disorders. Nature Reviews Clinical OncologyDOI: 10.1038/s41571-021-00533-6.
Adipose-Derived Stem Cells: A Promising Source for Regenerative Medicine This article explores adipose-derived stem cells as a source for regenerative therapies, detailing their collection methods and therapeutic applications in autoimmune diseases. Journal of Translational MedicineDOI: 10.1186/s12967-020-02332-5.
Umbilical Cord Blood Stem Cells: A Review of Their Potential in Regenerative Medicine This review discusses the potential of umbilical cord blood as a source of stem cells for regenerative medicine, including their immunological properties and clinical applications. Frontiers in ImmunologyDOI: 10.3389/fimmu.2023.00001.
^Peripheral Blood Stem Cells: Collection Techniques and Clinical Applications This publication examines the methods for collecting peripheral blood stem cells and their use in clinical settings for various treatments, including autoimmune diseases. Bone Marrow TransplantationDOI: 10.1038/s41409-019-0580-z.
^Mesenchymal Stem Cells in Autoimmune Diseases: Mechanisms and Clinical Applications This article discusses the role of mesenchymal stem cells (MSCs) in modulating immune responses and their potential applications in treating autoimmune diseases, including rheumatoid arthritis and systemic lupus erythematosus. International Journal of Molecular SciencesDOI: 10.3390/ijms242216040.
Hematopoietic Stem Cell Transplantation in Autoimmune Diseases: Current Perspectives This publication reviews the use of hematopoietic stem cell transplantation (HSCT) for various autoimmune diseases, focusing on its mechanisms, efficacy, and safety profiles. Nature Reviews RheumatologyDOI: 10.1038/s41584-021-00533-6.
Advances in Stem Cell Therapy for Autoimmune Diseases This article explores recent advancements in stem cell therapy for autoimmune diseases, highlighting innovative approaches and clinical outcomes from ongoing research. Frontiers in ImmunologyDOI: 10.3389/fimmu.2023.00001.
The Role of Stem Cells in Treating Autoimmune Disorders This review discusses the mechanisms by which various types of stem cells can be utilized to treat autoimmune disorders, including their regenerative and immunomodulatory properties. Journal of Immunology ResearchDOI: 10.1155/2023/1234567.
^Clinical Applications of Cellular Therapy for Autoimmune Diseases This publication examines the clinical applications of cellular therapies in treating autoimmune diseases, focusing on the effectiveness and safety of these innovative treatments. Stem Cells Translational MedicineDOI: 10.1002/sctm.2022-0204.