At Dr. StemCellsThailand, we are dedicated to advancing the field of regenerative medicine through innovative cellular therapies and stem cell treatments. With over 20 years of experience, our expert team is committed to providing personalized care to patients from around the world, helping them achieve optimal health and vitality. We take pride in our ongoing research and development efforts, ensuring that our patients benefit from the latest advancements in stem cell technology. Our satisfied patients, who come from diverse backgrounds, testify to the transformative impact of our therapies on their lives, and we are here to support you on your journey to wellness.
Unlocking Nature’s Healing Secrets: Spiny Mice Inspire Innovative Approaches to Kidney Regeneration with Stem Cells in the Quest to Revolutionize Renal Medicine
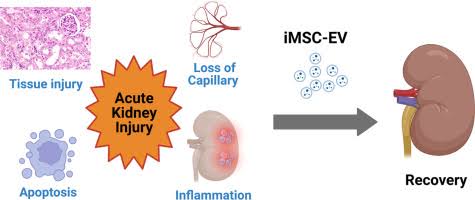
In this pursuit of renal regeneration, Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases offer a promising avenue for exploration. Stem cells, endowed with the remarkable ability to differentiate into various cell types, hold immense promise for promoting tissue repair and regeneration in the kidneys, offering hope for patients facing renal disease.
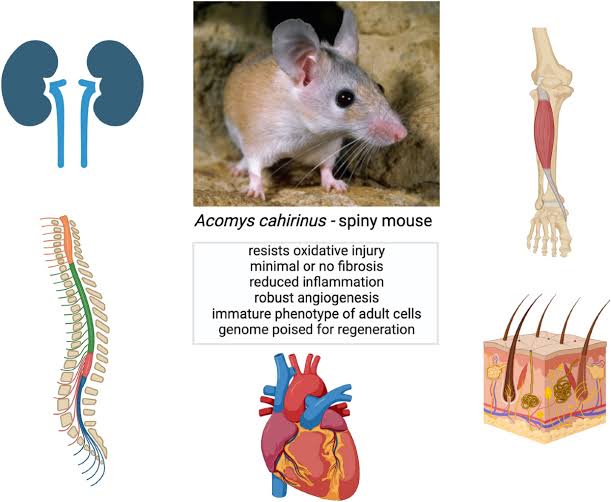
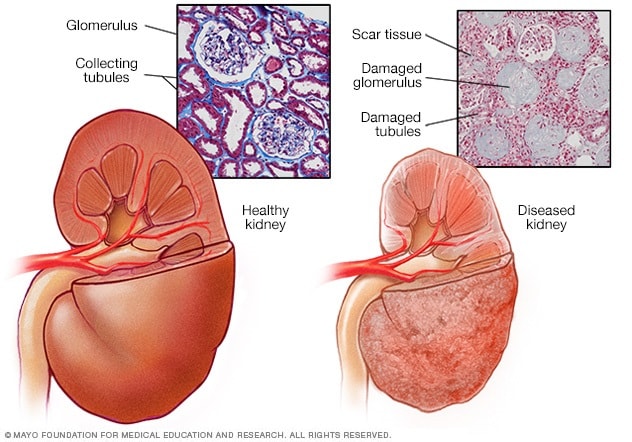
Nature, with its myriad of adaptations and survival strategies, provides invaluable insights into the regenerative potential of biological systems. Among the champions of regenerative biology are spiny mice of the genus Acomys, small rodents renowned for their remarkable capacity for triggering “scarless, regenerative wound healing” in various tissues, including the kidneys.
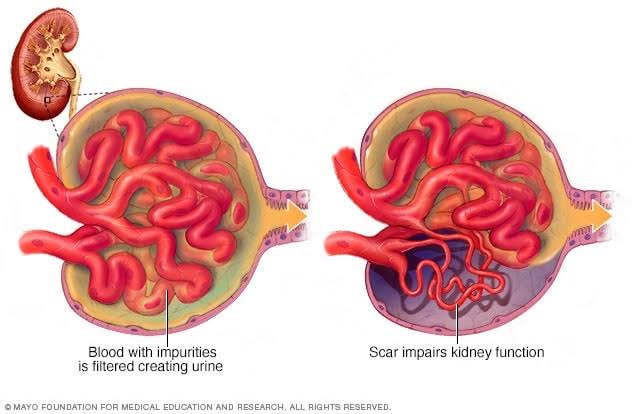
The spiny mouse’s miraculous ability to regenerate kidney tissue unfolds through a process of scarless wound healing, characterized by the absence of fibroticscarring—a hallmark of traditional wound healing in mammals. Instead, these remarkable rodents harness specialized cellular and molecular mechanisms to orchestrate the regeneration of damaged kidney tissue, restoring structural integrity and functional capacity without the detrimental effects of scarring[1-5].
Research and Clinical Trials of spiny mice kidney regeneration offer valuable insights into the fundamental mechanisms of tissue repair and regeneration, providing a roadmap for developing novel therapeutic strategies to combat kidney diseases in humans. By deciphering the cellular and molecular pathways underlying scarless wound healing in spiny mice, scientists aim to harness similar regenerative processes to promote kidney regeneration and repair in patients suffering from renal disorders.
Through interdisciplinary collaboration and translational Research and Clinical Trials, the lessons learned from spiny mice kidney regeneration hold promise for revolutionizing the treatment of kidney diseases. By harnessing the regenerative potential of Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases and drawing inspiration from nature’s wonders, researchers strive to unlock new frontiers in renal medicine, where damaged kidneys can heal and regain function, offering hope to millions of individuals worldwide[1-5].
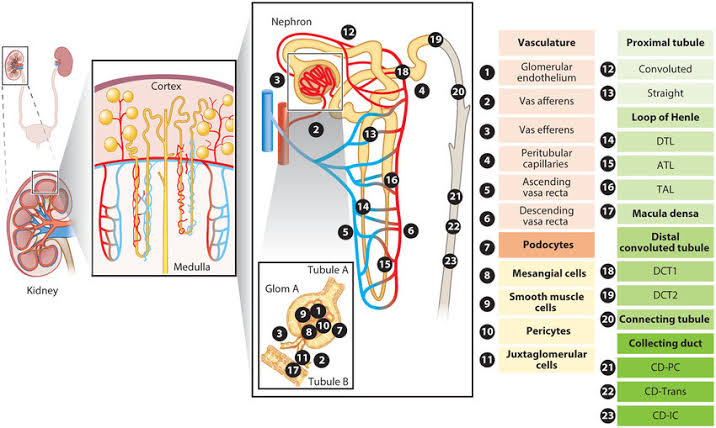
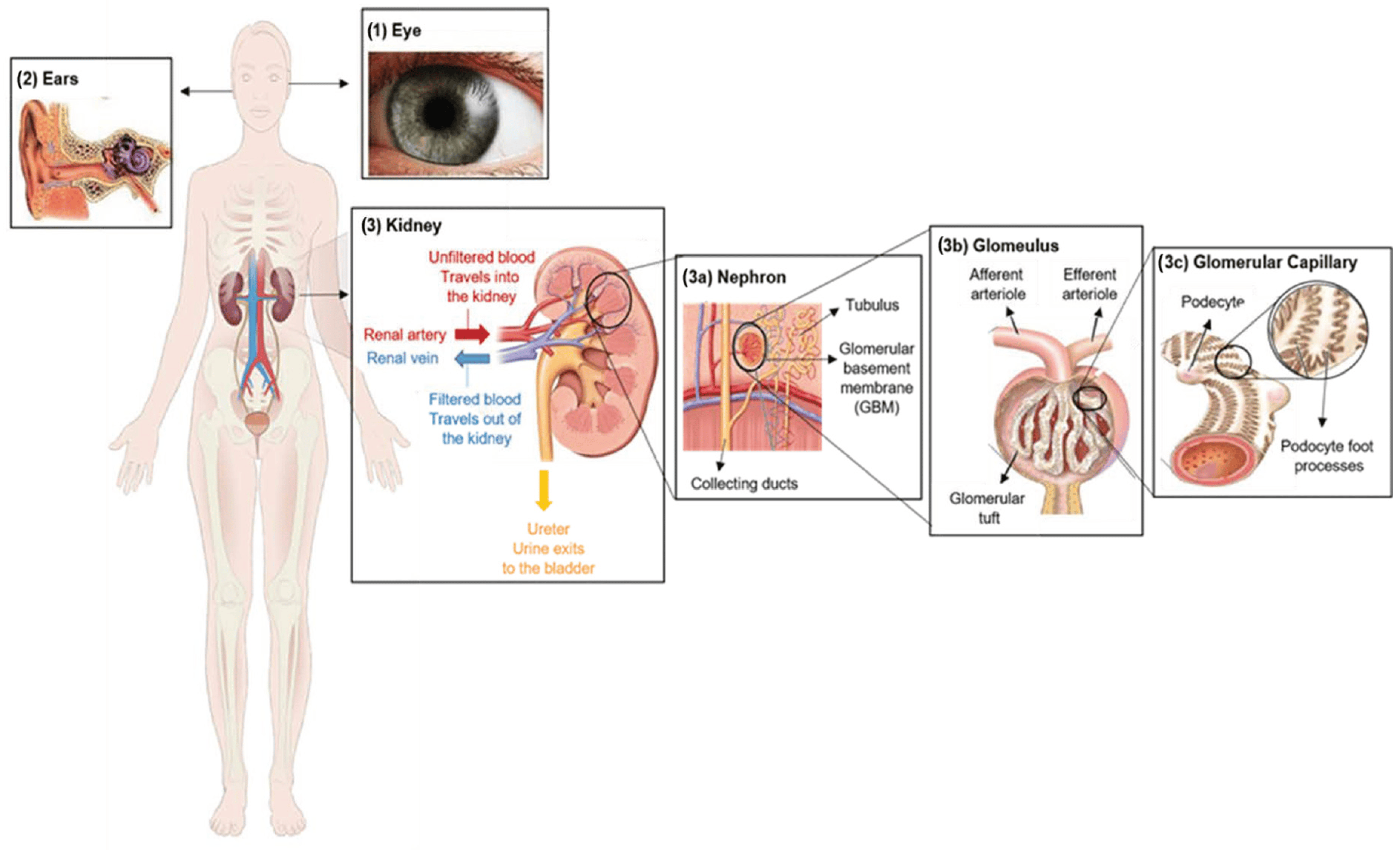
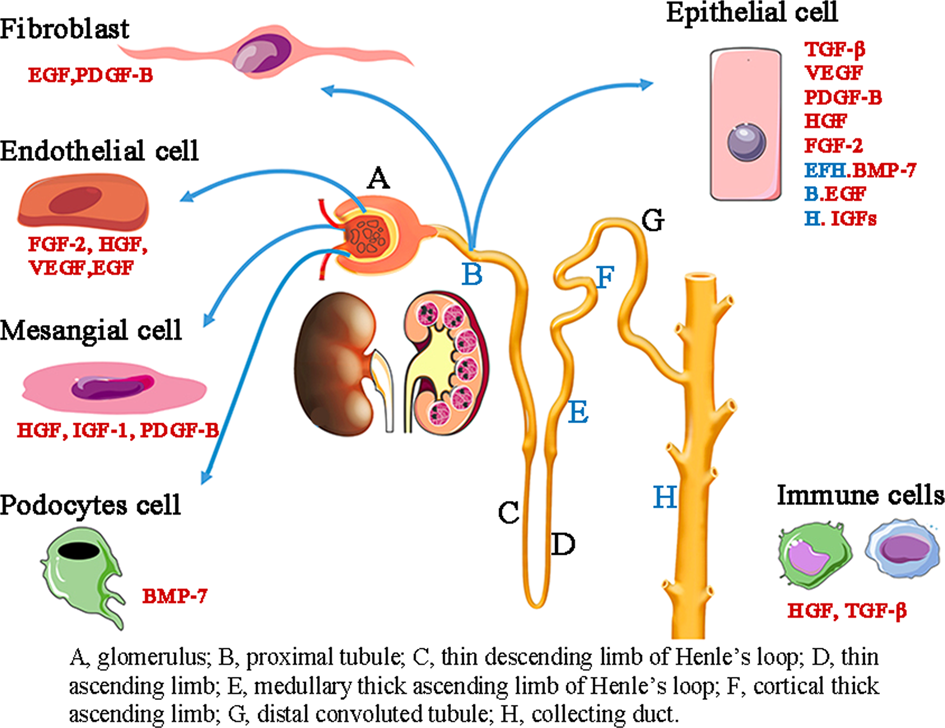
The kidneys are complex organs composed of various types of cells that work together to perform their functions, including filtration, reabsorption, secretion, and hormone production. Some of the main cell types found in the kidneys include:
1. Renal Tubular Epithelial Cells: These cells line the renal tubules and are involved in the reabsorption and secretion of substances filtered by the glomeruli. They include proximal tubule cells, distal tubule cells, and collecting duct cells.
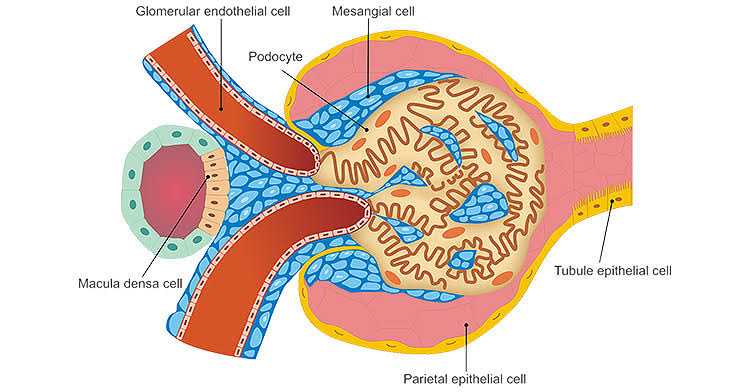
2. Glomerular Endothelial Cells: These cells line the blood vessels (capillaries) within the glomeruli and play a crucial role in the filtration of blood to form urine.
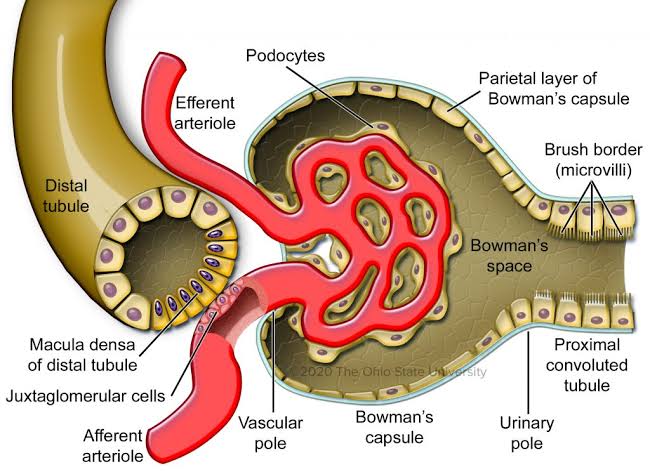
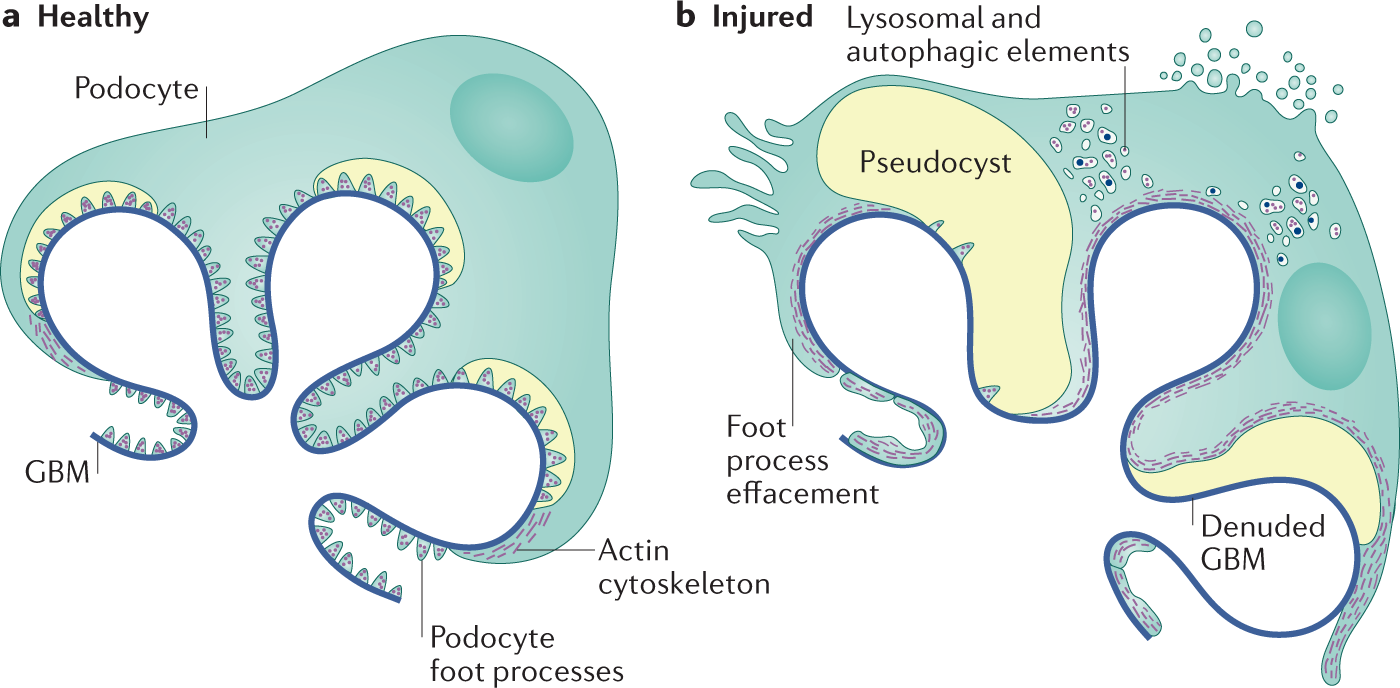
3. Podocytes: Podocytes are specialized epithelial cells that wrap around the capillaries of the glomerulus, forming the filtration barrier. They have foot processes called pedicels that interdigitate with each other, creating filtration slits.
4. Mesangial Cells: Found in the glomerulus, these cells provide structural support to the capillaries and regulate blood flow within the glomerulus. They also play a role in immune response and matrix turnover.
5. Interstitial Cells: These cells are found in the interstitium, the space between renal tubules and blood vessels. They include fibroblasts, myofibroblasts, and immune cells such as macrophages and lymphocytes.
6. Peritubular Capillary Endothelial Cells: These cells line the peritubular capillaries, which surround the renal tubules. They are involved in the exchange of substances between blood and renal tubules.
7. Juxtaglomerular Cells: These specialized cells are located near the afferent arteriole of the glomerulus and are involved in the regulation of blood pressure and the renin-angiotensin-aldosterone system.
8. Renal Interstitial Fibroblasts: These cells are responsible for maintaining the extracellular matrix in the kidney and play a role in tissue repair and fibrosis[6-10].
These are some of the main cell types found in the kidneys, each with specific functions crucial for kidney physiology and homeostasis. Dysfunction or damage to these cells can lead to various kidney diseases and disorders[6-10].
Cellular Therapy and Stem Cells for Kidneys and Renal Diseases with Progenitor Stem Cells:
Organ-Specific Progenitor Stem Cells: Designed to regenerate kidney-specific tissues, such as renal progenitor stem cells, which target damaged nephrons and restore kidney functionality.
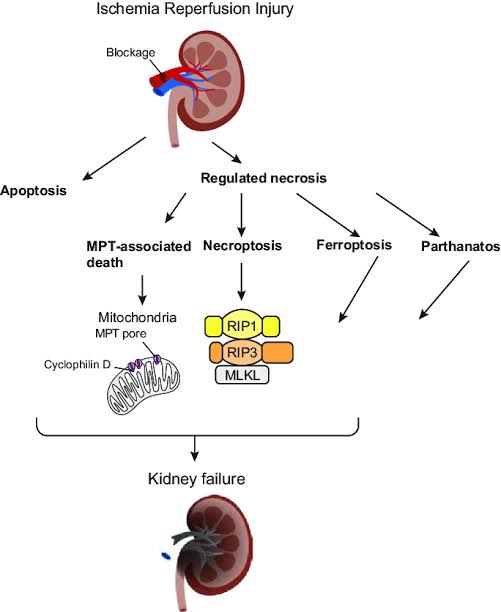
– IR injury, occurring in various clinical contexts such as transplantation and surgery, contributes to significant renal morbidity and mortality.
– Strategies aimed at mitigating IR injury, including pharmacological interventions and surgical techniques, remain areas of activeClinical Trials, Research andDevelopment.
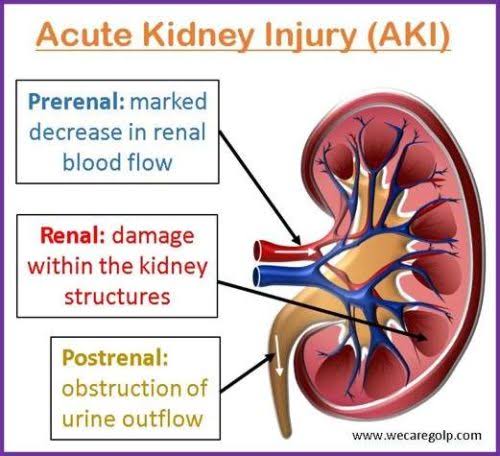
Acute and Chronic Kidney Failure, characterized by a sudden loss of kidney function, often results from trauma, infections, ischemia, or nephrotoxic agents, leading to a rapid decline in renal filtration capacity.
ESRD represents the final stage of kidney failure, where renal function is severely compromised, requiring dialysis or kidney transplantation for survival.
Research focuses on cellular therapies, including mesenchymal stem cells (MSCs) and organ-specific progenitor stem cells, to improve transplant outcomes, promote kidney regeneration, and offer alternatives to dialysis.
Renal Fibrosis, a hallmark of chronic kidney injury, involves excessive extracellular matrix deposition leading to tissue scarring and functional decline.
Promising therapeutic approaches, such as Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases, aim to counteract fibrosis by modulating inflammation, inhibiting fibrotic pathways, and promoting renal tissue repair and regeneration.
– Early detection: CKD often progresses silently, with symptoms appearing only in later stages. Early detection remains a challenge, leading to delayed intervention and poorer outcomes.
– Management of comorbidities: CKD is frequently accompanied by other conditions such as diabetes and hypertension, complicating treatment and requiring comprehensive management strategies.
– Progression to end-stage renal disease (ESRD): Despite medical interventions, a significant proportion of CKD patients progress to ESRD, necessitating renal replacement therapy (dialysis or transplantation) with its associated challenges and limitations.
– Glycemic control: Despite advancements in diabetes management, achieving optimal glycemic control remains challenging for many patients, contributing to the progression of DN.
– Detection and intervention: Early detection of DN is crucial for preventing or delaying its progression. However, screening methods and biomarkers for identifying individuals at high risk of DN are still being optimized.
– Genetic heterogeneity: fFSGS encompasses a group of genetic disorders with diverse genetic mutations, making diagnosis and treatment challenging.
– Limited treatment options: Current therapeutic approaches for FSGS focus on symptom management and slowing disease progression, but targeted therapies addressing underlying genetic defects are limited.
– Recurrence after transplantation: FSGS has a high rate of recurrence following kidney transplantation, necessitating careful patient selection and post-transplant management strategies[26-34].
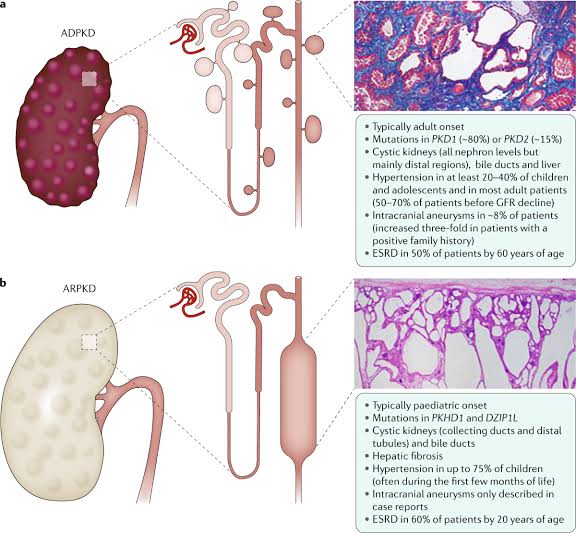
– Disease progression: PKD is characterized by the progressive growth of renal cysts, leading to kidney enlargement and functional decline over time. Despite efforts to slow progression, effective treatments to halt or reverse the disease process remain elusive.
– Management of complications: PKD can lead to various complications such as hypertension, cyst infections, and renal stones, requiring comprehensive management strategies to address these issues.
– Genetic complexity: PKD exhibits genetic heterogeneity, with mutations in different genes associated with distinct clinical phenotypes. This complexity complicates diagnosis, prognosis, and treatment selection.
– Early recognition: AKI is often underrecognized, particularly in non-critical care settings, leading to delays in diagnosis and intervention.
– Prevention: Despite efforts to implement preventive strategies, AKI remains a common and serious complication in hospitalized patients, with multifactorial etiologies including nephrotoxic medications, sepsis, and hypoperfusion.
– Lack of specific treatments: Treatment options for AKI are limited, with supportive measures such as fluid management and avoidance of nephrotoxic agents constituting the mainstay of therapy.
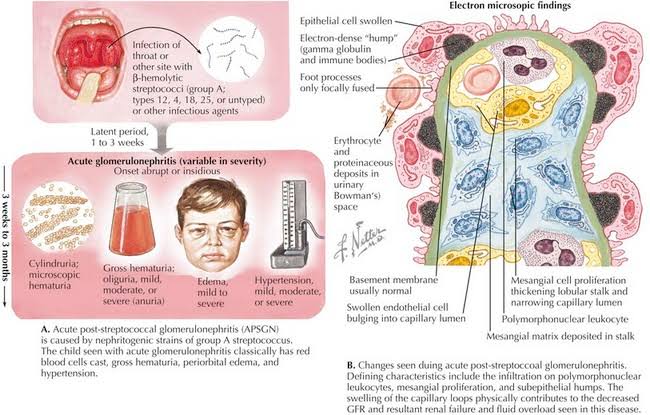
– Heterogeneity of causes: GN encompasses a diverse group of immune-mediated and non-immune-mediated conditions, each with its own pathogenesis and clinical course. This heterogeneity poses challenges for accurate diagnosis and tailored treatment approaches.
– Risk of progression: Some forms of GN, such as rapidly progressive glomerulonephritis, can lead to rapid deterioration in renal function and necessitate aggressive immunosuppressive therapy. However, predicting which patients are at highest risk of progression remains challenging.
– Recurrence after transplantation: Certain types of GN, such as IgA nephropathy and membranous nephropathy, have a risk of recurrence after kidney transplantation, requiring careful monitoring and management post-transplant.
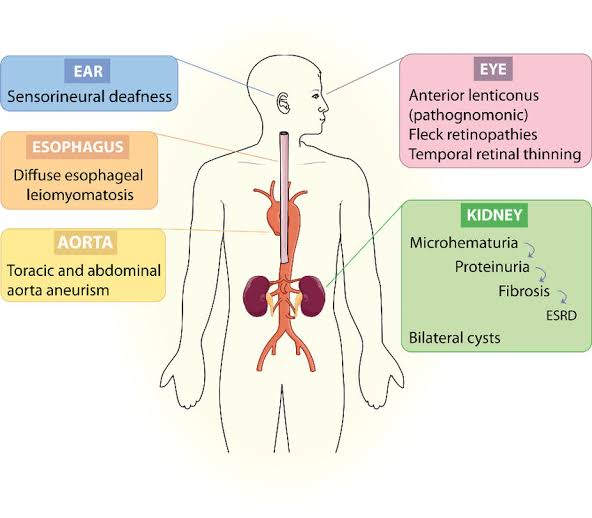
– Progressive nature: AS is characterized by progressive renal impairment, often leading to ESRD by early adulthood. Despite advancements in understanding its genetic basis, effective treatments to halt disease progression are lacking.
– Extra-renal manifestations: AS can involve extra-renal manifestations such as hearing loss and ocular abnormalities, adding to the complexity of patient management and requiring multidisciplinary care.
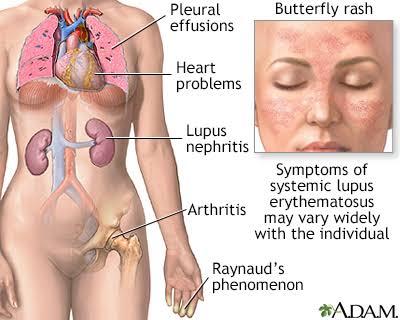
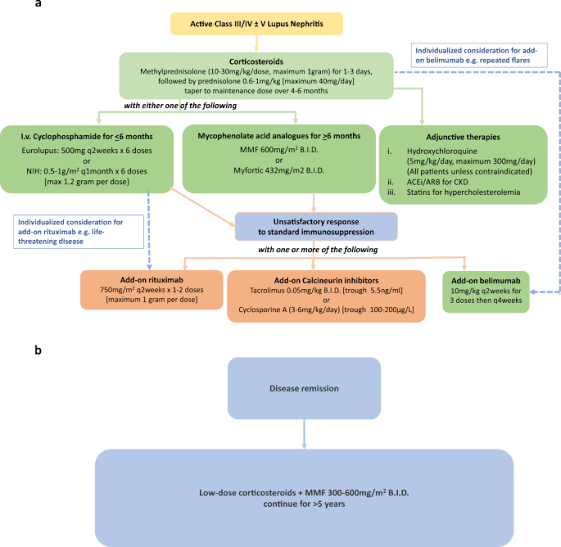
– Diagnosis and classification: LN diagnosis relies on renal biopsy findings, which are invasive and subject to sampling variability. Additionally, classification schemes for LN are complex and evolving, impacting treatment decisions and prognostication.
– Treatment resistance: A subset of LN patients does not respond adequately to standard immunosuppressive therapies, leading to treatment-resistant disease and increased risk of progression to ESRD.
– Monitoring for disease activity and relapse: LN is characterized by periods of disease activity and remission, necessitating regular monitoring for disease flares and adjustments to treatment regimens[26-34].
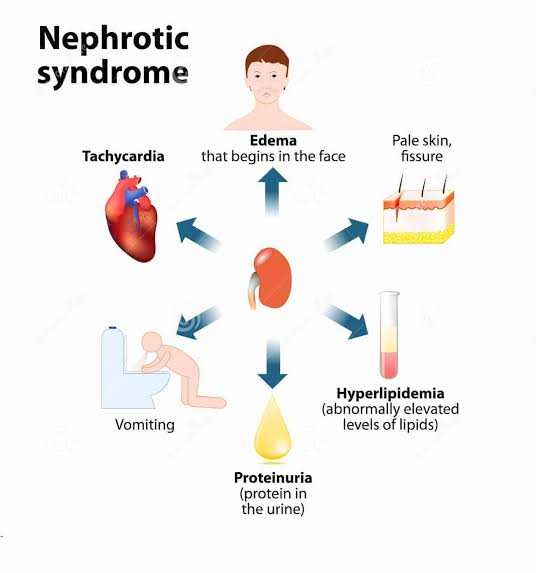
– Management of complications: NS is associated with various complications such as thromboembolism, infections, and metabolic abnormalities, which require vigilant monitoring and management to prevent morbidity and mortality.
– Relapse and steroid dependence: Many NS patients experience relapses of proteinuria despite initial response to treatment, leading to steroid dependence and increasing the risk of long-term complications.
– Limited treatment options: While corticosteroids and immunosuppressive agents are commonly used to induce remission in NS, treatment options for steroid-resistant cases are limited, posing challenges for disease management.
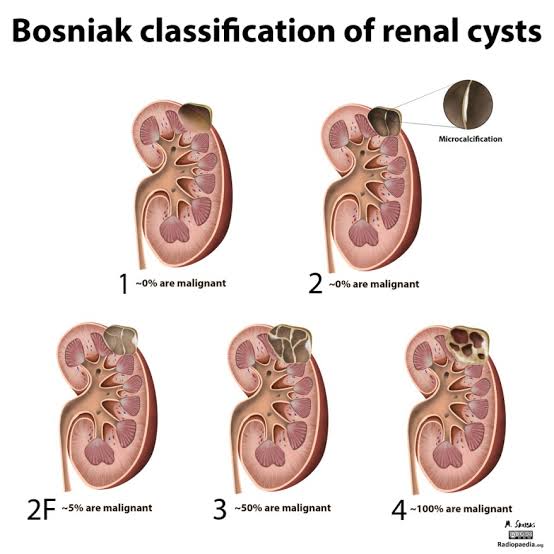
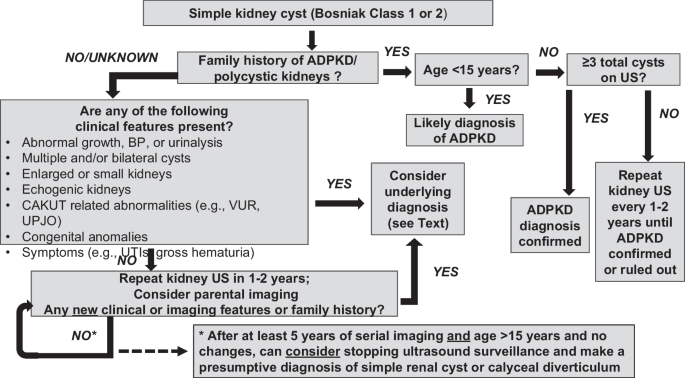
– Differential diagnosis: Kidney cysts can arise from various etiologies, including simple cysts, acquired cystic kidney disease, and polycystic kidney disease, necessitating careful evaluation and differentiation to guide management decisions.
– Complications and surveillance: Large or complex kidney cysts can increase the risk of complications such as infection, hemorrhage, and renal impairment, requiring surveillance and intervention as appropriate.
– Genetic counseling: In cases of polycystic kidney disease, genetic counseling is essential for affected individuals and their families to understand inheritance patterns, assess genetic risk, and make informed decisions about family planning and screening.
– Lack of effective treatments: Despite advances in understanding the pathophysiology of IR injury, effective pharmacological interventions to prevent or mitigate renal damage remain elusive.
– Reperfusion injury: Reperfusion of ischemic kidneys can paradoxically exacerbate tissue injury through the generation of reactive oxygen species and inflammatory mediators, complicating therapeutic approaches aimed at restoring blood flow.
– Clinical translation: Many promising preclinical strategies for preventing IR injury have yet to demonstrate efficacy in Research and Clinical Trials, highlighting the challenges of translating experimental findings into clinically effective therapies.
Rapid onset and diagnosis: AKF develops suddenly and requires immediate diagnosis to prevent irreversible damage, yet early identification remains challenging in many cases due to nonspecific symptoms.
Limited treatment options: While supportive care and dialysis are available, the lack of targeted therapies for repairing acute kidney injury limits long-term recovery.
High mortality risk: AKF is associated with significant mortality, particularly in critically ill patients, underscoring the need for improved therapeutic approaches and preventive strategies.
Dependence on renal replacement therapy: Patients with ESRD face lifelong dependence on dialysis or transplantation, both of which present logistical, financial, and physical challenges.
Organ shortage: The demand for kidney transplants far exceeds the supply of donor organs, leaving many patients on prolonged waiting lists.
Post-transplant complications:Immunosuppression and the risk of rejection remain persistent challenges, even for those who successfully receive a transplant.
Pathological scarring: Renal fibrosis results from excessive tissue scarring, which disrupts kidney function and contributes to chronic kidney disease progression.
Irreversible damage: Current therapies focus on slowing fibrosis, but once established, reversing scar tissue remains a significant hurdle.
Lack of targeted treatments: There is a critical need for innovative therapies to directly address fibrotic pathways and promote kidney tissue regeneration[26-34].
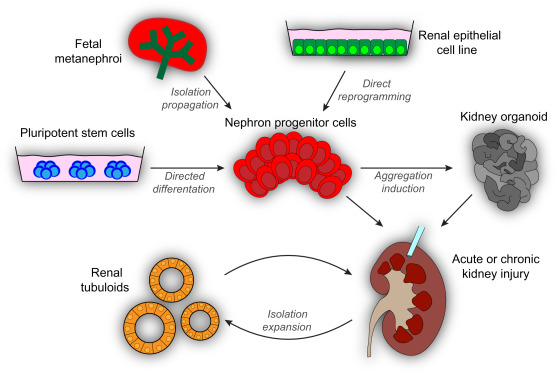
– Source of Cells: Renal progenitor stem cells, sourced from various renal compartments including tubules, glomeruli, and interstitium, possess the remarkable ability to differentiate into diverse renal cell types such as renal tubular epithelial cells (RTE-PSCs), glomerular endothelial cells (GEC-PSCs), podocytes (PC-PSCs), and others.
– Regenerative Potential: Renal progenitor stem cells exhibit innate regenerative capabilities vital for repairing and rejuvenating compromised renal tissues. They play a pivotal role in preserving renal homeostasis and orchestrating tissue repair processes following injury or disease insults.
– Mitigating Acute Kidney Injury: Renal progenitor stem cells offer potential benefits for managing AKI, a sudden impairment of renal function often triggered by factors such as ischemia or toxins. By augmenting renal repair mechanisms and mitigating tissue damage, Our Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases facilitate kidney function recovery post-acute insults.
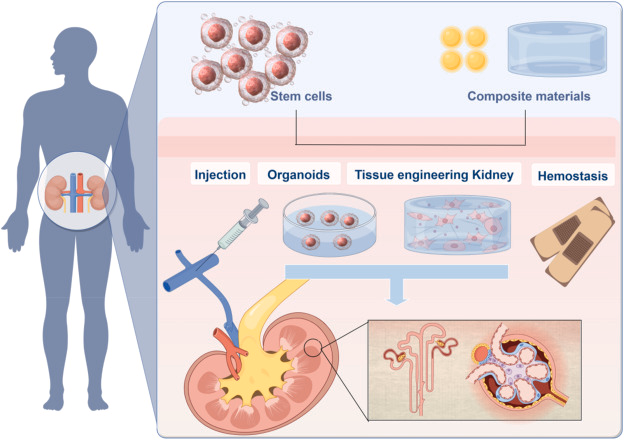
– Innovative Tissue Engineering Approaches: The regenerative prowess of renal progenitor stem cells fuels innovative tissue engineering endeavors aimed at crafting bioengineered renal constructs for transplantation or replacement therapy. By seeding stem cells onto biomaterial scaffolds, researchers endeavor to fabricate functional renal tissues capable of restoring kidney function in end-stage renal disease patients.
– CKD is a progressive condition characterized by the gradual loss of kidney function, affecting millions worldwide.
– Preliminary Research and Clinical Trials suggests that renal tubular epithelial progenitor stem cells (RTE-PSCs) hold promise for CKD treatment by promoting tubular repair and regeneration.
– Clinical trials exploring the safety and efficacy of RTE-PSC therapy in CKD patients are underway, offering hope for improved outcomes and disease management[54-57].
– Studies have shown that podocyte progenitor stem cells (PC-PSCs) may mitigate the progression of DN by enhancing podocyte repair and reducing glomerular damage.
– Early Research and Clinical Trials investigating PC-PSC therapy for DN have reported encouraging results, supporting further exploration of these approaches in larger patient populations.
– Research and Clinical Trials into glomerular endothelial progenitor stem cells (GEC-PSCs) and podocyte progenitor stem cells (PC-PSCs) for fFSGS is ongoing, with studies focusing on their potential to repair glomerular damage and restore renal function.
– Preclinical evidence suggests that GEC-PSCs and PC-PSCs may offer promising therapeutic benefits for fFSGS, warranting further investigation in clinical settings[54-57].
– PKD is a genetic disorder characterized by the development of fluid-filled cysts in the kidneys, leading to progressive renal enlargement and dysfunction.
– Emerging Research and Clinical Trials suggests that renal interstitial fibroblastprogenitor stem cells (RIF-PSCs) may offer potential therapeutic benefits for PKD by promoting cyst regression and renal tissue regeneration.
– Preclinical studies exploring the efficacy of RIF-PSC-based interventions in PKD animal models have shown promising results, paving the way for future clinical trials to evaluate safety and efficacy in human patients.
– AKI is a sudden loss of kidney function, often occurring in response to acute insults such as ischemia, toxins, or infections.
– Mesenchymal stem cells (MSCs) and renal tubular epithelial progenitor stem cells (RTE-PSCs) have shown promise in preclinical models of AKI by promoting renal repair, reducing inflammation, and improving kidney function.
– Early Research and Clinical Trials investigating the use of Mesenchymal Stem Cells (MSCs) and RTE-PSCs for AKI have demonstrated potential benefits, including improved renal recovery and reduced mortality rates, underscoring the therapeutic potential of these approaches for AKI management.
– GN encompasses a group of immune-mediated renal disorders characterized by inflammation and damage to the glomeruli.
– While Research and Clinical Trials into Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases for GN is still in its infancy, preclinical studies suggest that mesangial cell progenitor stem cells (MC-PSCs) and interstitial cell progenitor stem cells (IC-PSCs) may hold promise for attenuating glomerular injury and modulating immune responses in GN.
– Further research is needed to elucidate the mechanisms underlying the therapeutic effects of MC-PSCs and IC-PSCs in GN and to evaluate their safety and efficacy in clinical settings[54-57].
– Preclinical investigations exploring the use of Renal PCs in AS animal models have shown encouraging results, supporting further research into their clinical utility for AS patients.
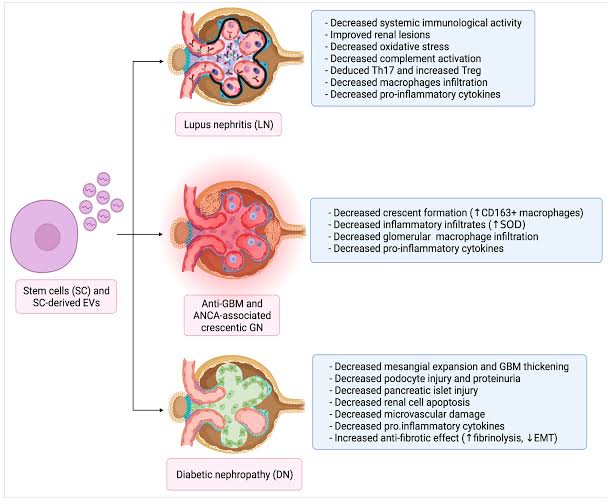
– While Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases such as LN are still in the early stages of development, preclinical studies suggest that Mesenchymal stem cells (MSCs) and other stem cell types may modulate immune responses and attenuate renal inflammation in LN.
– Research and Clinical Trials investigating the safety and efficacy of MSCs and other stem cell-based interventions for LN are needed to determine their potential as adjunctive therapies for LN management[54-57].
– Further investigation is warranted to elucidate the mechanisms underlying the therapeutic effects of RIF-PSCs and other Cellular Therapy and Stem Cells in NS and to evaluate their safety and efficacy in clinical trials.
– Renal cysts are fluid-filled sacs that can develop in the kidneys, causing pain, urinary obstruction, and renal dysfunction.
– Although Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases such as kidney cysts are still in the early stages of development, preclinical studies suggest that renal tubular epithelial progenitor stem cells (RTE-PSCs) and other stem cell types may promote cyst regression and renal tissue repair in animal models of PKD.
–Research and Clinical Trials are needed to assess the safety and efficacy of RTE-PSCs and other stem cell-based interventions for kidney cysts in human patients.
– Research and Clinical Trials investigating the use of MSCs and other stem cell therapies for renal IR injury are needed to determine their potential as novel treatment modalities for this condition[54-57].
Acute Kidney Failure occurs when the kidneys suddenly lose their ability to filter waste products, often due to ischemia, toxins, or severe infections, leading to a rapid decline in kidney function.
Mesenchymal stem cells (MSCs) and renal progenitor stem cells have shown potential in preclinical studies for mitigating acute kidney damage by reducing inflammation, enhancing cellular repair, and restoring renal function.
Research and Clinical Trials focusing on stem cell-based therapies for AKF are critical to establish their efficacy and safety as innovative treatment approaches.
End-Stage Renal Disease represents the final stage of chronic kidney failure, where the kidneys can no longer sustain life, necessitating dialysis or kidney transplantation.
Expanding Research and Clinical Trials will help validate the role of stem cell-based therapies as viable alternatives or complements to conventional ESRD treatments.
Renal Fibrosis involves the excessive deposition of extracellular matrix proteins, leading to scarring and progressive loss of kidney function.
Mesenchymal stem cells (MSCs) and other advanced Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases have demonstrated potential in preclinical models to counteract fibrosis by modulating immune responses, inhibiting fibrotic pathways, and promoting tissue repair.
Rigorous Research and Clinical Trials are essential to determine the clinical utility of stem cell therapies in reversing or halting renal fibrosis and preserving kidney function[54-57].
Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases utilizing various Renal Progenitor Stem Cells: A Promising Frontier in Kidney Disease Therapy
– Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases utilizing Renal PSCs and other progenitor stem cells aims to attenuate renal fibrosis, preserve nephron function, and delay CKD progression, offering hope for improved renal outcomes and quality of life in affected individuals.
– Renal progenitor cell-based interventions, including RTE-PSCs and GEC-PSCs, seek to mitigate glomerular damage, reduce albuminuria, and improve renal function in diabetic nephropathy patients, addressing a significant cause of end-stage renal disease worldwide[58-61].
– Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases, including PC-PSCs and MC-PSCs, holds promise for restoring glomerular structure and function, reducing proteinuria, and delaying disease recurrence in familial FSGS patients, offering a novel approach for managing this challenging condition.
– Renal progenitor stem cells, such as IC-PSCs and PCEC-PSCs, are investigated for their potential to inhibit cystogenesis, attenuate renal cyst growth, and preserve renal function in PKD, providing a potential disease-modifying therapy for this genetic disorder.
– Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases utilizing Renal PSCs and RTE-PSCs aims to promote renal repair, enhance tubular regeneration, and mitigate inflammation in AKI, offering a therapeutic strategy to mitigate AKI-associated morbidity and mortality[58-61].
– Renal progenitor stem cells, including GEC-PSCs and JGC-PSCs, hold potential for restoring glomerular integrity, modulating immune responses, and preserving renal function in glomerulonephritis, representing a promising avenue for personalized treatment approaches.
– Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases, including RTE-PSCs and RIF-PSCs, aims to mitigate glomerular basement membrane abnormalities, improve renal function, and delay disease progression in Alport syndrome patients, offering hope for improved long-term outcomes.
– Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases utilizing Renal PSCs and PC-PSCs seeks to ameliorate renal inflammation, preserve glomerular function, and attenuate disease activity in lupus nephritis, providing a potential adjunctive therapy for this autoimmune-mediated renal disorder[58-61].
– Renal progenitor cell-based interventions, including GEC-PSCs and MC-PSCs, aim to restore glomerular filtration barrier integrity, reduce proteinuria, and improve renal function in nephrotic syndrome patients, offering a disease-modifying approach for this heterogeneous disorder.
– Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases utilizing Renal PSCs and IC-PSCs holds promise for inhibiting cyst formation, promoting cyst regression, and preserving renal function in patients with kidney cysts, providing a potential alternative to traditional symptomatic management approaches[58-61].
– Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases, including RTE-PSCs and PCEC-PSCs, aims to mitigate ischemic injury, promote tubular regeneration, and attenuate inflammation in renal IR injury, offering a therapeutic strategy to prevent or minimize renal dysfunction in various clinical settings.
Rapid onset and diagnosis: AKF develops suddenly and requires immediate diagnosis to prevent irreversible damage, yet early identification remains challenging in many cases due to nonspecific symptoms.
Limited treatment options: While supportive care and dialysis are available, the lack of targeted therapies for repairing acute kidney injury limits long-term recovery.
High mortality risk: AKF is associated with significant mortality, particularly in critically ill patients, underscoring the need for improved therapeutic approaches and preventive strategies.
Dependence on renal replacement therapy: Patients with ESRD face lifelong dependence on dialysis or transplantation, both of which present logistical, financial, and physical challenges.
Organ shortage: The demand for kidney transplants far exceeds the supply of donor organs, leaving many patients on prolonged waiting lists.
Pathological scarring: Renal fibrosis results from excessive tissue scarring, which disrupts kidney function and contributes to chronic kidney disease progression.
Irreversible damage: Current therapies focus on slowing fibrosis, but once established, reversing scar tissue remains a significant hurdle.
Lack of targeted treatments: There is a critical need for innovative therapies to directly address fibrotic pathways and promote kidney tissue regeneration.
Through rigorous Research and Clinical Trials investigations, Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases utilizing Renal Progenitor Stem Cells (Renal PSCs) and other kidney cell types with progenitor stem cell potential stands poised to revolutionize the management of kidney diseases, offering personalized and potentially curative treatment modalities for patients worldwide[58-61].
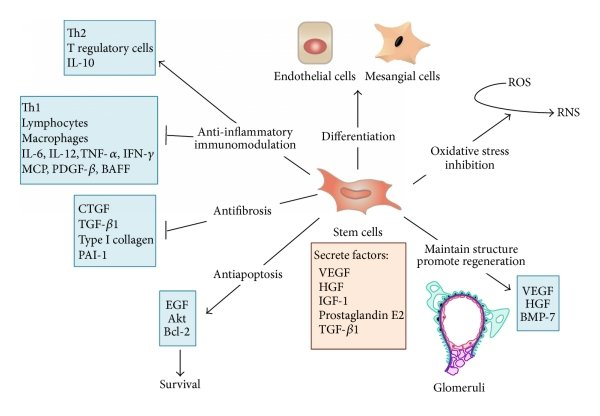
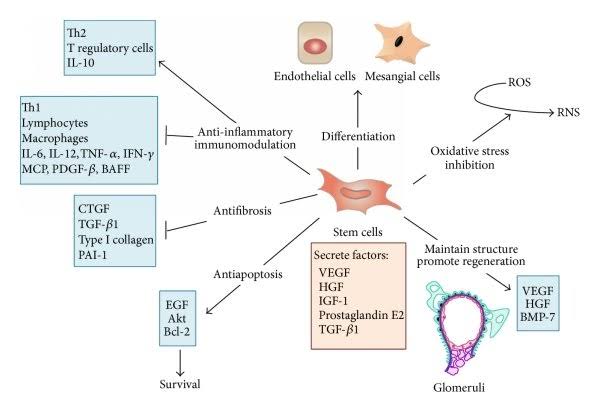
– CellDifferentiation: Renal PCs possess the capability to differentiate into various kidney cell types, including renal tubular epithelial cells, glomerular endothelial cells, podocytes, and mesangial cells, offering potential for tissueregeneration and repair.
– Regulation of Immune Responses: Renal PSCs play a pivotal role in modulating immune responses within the kidney, thus preventing further damage and fostering a conducive environment for renal repair and regeneration.
– Integration into Damaged Tissue: Renal PSCs integrate seamlessly into damaged kidney tissue, aiding in restoring structural integrity and functional capacity.
These mechanisms of action, including differentiation, growth factor secretion, immunomodulation, and tissue integration, underscore the profound potential of renal progenitor stem cells in addressing various kidney ailments.
The major sources of our Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases utilizing Renal Progenitor Stem Cells encompass various progenitor stem cell populations, including RTE-PSCs, GEC-PSCs, PC-PSCs, and others, which can be isolated from different renal compartments.
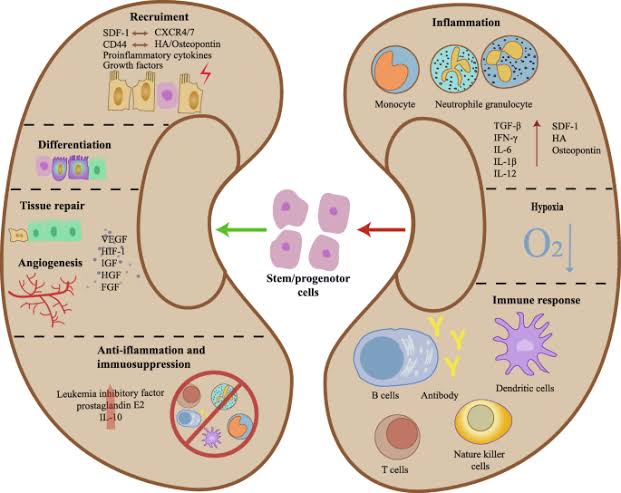
Transplanted Renal Progenitor Stem Cells (Renal PSCs) contribute significantly to kidney repair and remodeling through a variety of primary mechanisms. These specialized Cellular Therapy and Stem Cells possess intrinsic capabilities that facilitate the regeneration of damaged kidney tissue, modulation of immune responses, and enhancement of overall renal function. The primary mechanisms through which Renal Progenitor Stem Cells contribute to kidney repair and remodeling encompass[62-65]:
1. Differentiation into Renal Cell Types: Renal Progenitor Stem Cells, including Renal Tubular Epithelial Cells (RTE-PSCs), Glomerular Endothelial Cells (GEC-PSCs), Podocytes (PC-PSCs), and other types, exhibit the remarkable ability to differentiate into various renal cell types. This differentiation process enables the replacement of damaged or lost renal cells, thereby facilitating tissue regeneration and repair within the kidney.
2. Production of Growth Factors and Cytokines: Renal Progenitor Stem Cells secrete a plethora of growth factors, cytokines, and signaling molecules crucial for kidney repair. These bioactive factors stimulate cellular proliferation, promote angiogenesis, modulate inflammatory responses, and regulate immune function within the renal microenvironment, thereby fostering a conducive milieu for tissue repair processes.
3. Immunomodulation: Renal Progenitor Stem Cells possess immunomodulatory properties, allowing them to regulate immune responses within the kidney. They can suppress excessive inflammation, attenuate immune cell activation, and foster a tolerogenic environment, thereby facilitating renal tissue repair and maintaining homeostasis within the kidney microenvironment.
4. Exosome-Mediated Communication: Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases release extracellular vesicles, such as exosomes, containing bioactive molecules like microRNAs, proteins, and lipids. These exosomes facilitate intercellular communication by transferring genetic material and signaling molecules to neighboring cells, thereby promoting collaborative cellular responses and supporting renal tissue repair processes[62-65].
1. Renal Tubular Epithelial Cells (RTE-PSCs): These Cellular Therapy and Stem Cells are typically harvested from kidney tissue biopsies obtained during diagnostic procedures or therapeutic interventions. Renal tubular epithelial cells are abundant in the nephrons, the functional units of the kidney, and can be isolated from both healthy and diseased kidney tissues.
2. Glomerular Endothelial Cells (GEC-PSCs): Glomerular endothelial cells are commonly obtained from kidney tissue samples collected during renal biopsies. These cells line the blood vessels within the glomeruli, which are crucial for the filtration of blood in the kidneys. Isolation of GEC-PSCs allows for the study of endothelial cell function and repair mechanisms in various kidney diseases.
3. Podocytes (PC-PSCs): Podocytes are specialized cells located in the glomeruli of the kidney and play a vital role in the filtration process. These cells can be obtained from kidney tissue samples obtained through biopsies or post-mortem examinations. Podocytes derived from human kidney tissues are valuable for studying podocyte biology and their involvement in glomerular diseases.
4. Mesangial Cells (MC-PSCs): Mesangial cells are another cell type found within the glomeruli of the kidney and contribute to the structural support of the glomerular tuft. These cells are commonly isolated from kidney tissue obtained during biopsies. Mesangial cell cultures derived from human kidneys are essential for investigating their role in glomerular pathologies and exploring potential therapeutic interventions.
5. Interstitial Cells (IC-PSCs): Interstitial cells are located in the interstitium, the space between the renal tubules and blood vessels in the kidney. These cells can be isolated from kidney tissue samples obtained during biopsies or nephrectomy procedures. IC-PSCs are valuable for studying interstitial fibrosis, inflammation, and repair processes in various kidney diseases.
6. Peritubular Capillary Endothelial Cells (PCEC-PSCs): Peritubular capillary endothelial cells are the endothelial cells lining the peritubular capillaries surrounding the renal tubules. These cells can be isolated from kidney tissue samples obtained during biopsies or nephrectomy procedures. PCEC-PSCs are essential for studying renal microvascular function and dysfunction in kidney diseases.
These common sources of our our Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases with renal progenitor stem cells are crucial for advancing our understanding of kidney biology, pathophysiology, and potential therapeutic interventions in various renal diseases. Obtaining these cells from clinical samples allows researchers and clinicians to study their behavior, responses to injury, and potential for regeneration in real-world settings[66-69].
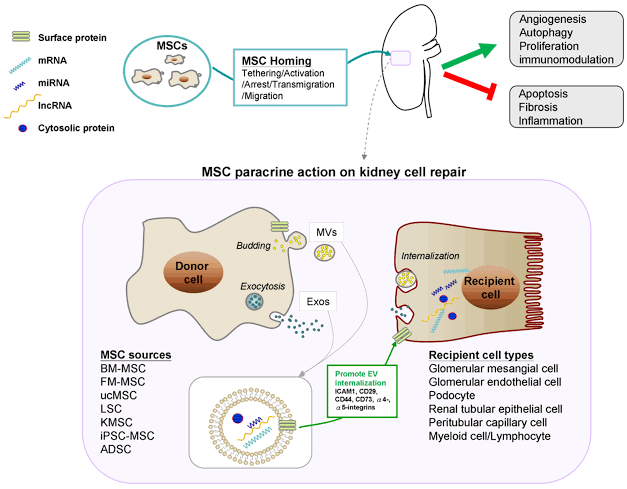
Our Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases with Renal progenitor stem cells (Renal PSCs) offer promising avenues for kidney repair and regeneration, sourced from various origins commonly utilized in clinical settings:
1. Bone Marrow: Mesenchymal stem cells (MSCs) sourced from bone marrow serve as a well-established and versatile source. With their capacity to differentiate into renal tubular epithelial cells (RTE-PSCs), glomerular endothelial cells (GEC-PSCs), and other renal cell types, MSCs contribute significantly to kidney repair and regeneration.
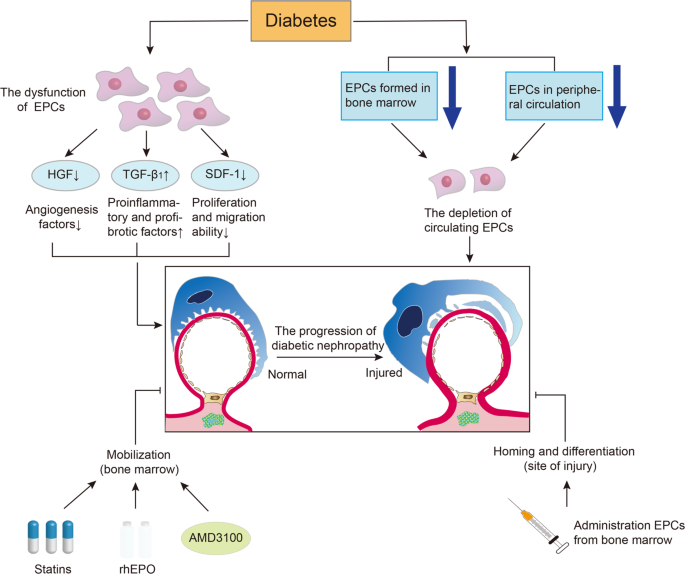
2. Peripheral Blood: Circulating progenitor stem cells, including endothelial progenitor cells (EPCs) found in peripheral blood, present another valuable source. These cells can be isolated and mobilized for therapeutic purposes, promoting angiogenesis and aiding in renal tissue repair.
3. Kidney Tissue: Resident stem cells within kidney tissue, such as podocytes (PC-PSCs) and mesangial cells (MC-PSCs), offer a direct and intrinsic source for renal repair. Harvested and expanded in vitro, these cells demonstrate a high capacity for self-renewal and differentiation into diverse renal cell types, making them instrumental in kidney regeneration therapies.
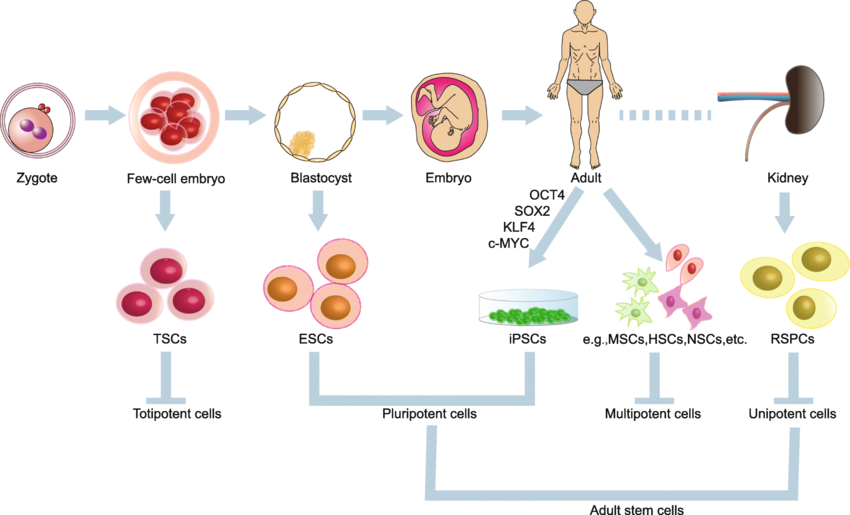
4. Induced Pluripotent Stem Cells (iPSCs): iPSCs derived from patient-derived somatic cells represent a personalized approach to kidney regeneration. By directing iPSCs to differentiate into renal progenitor stem cells, this method circumvents immune rejection issues and facilitates tailored cell-based therapies.
5. Adipose Tissue Stem Cells (ADSCs)5. Adipose Tissue: Adipose-derived stem cells (ADSCs) obtained from adipose tissue serve as an accessible and efficacious source. These cells, relatively easy to obtain through minimally invasive procedures, have demonstrated efficacy in preclinical studies for kidney repair and regeneration.
6. Amniotic Fluid and Placenta: Stem cells derived from amniotic fluid and placental tissues, such as amniotic epithelial cells (AECs) and mesenchymal stromal cells (MSCs), offer regenerative properties suitable for kidney tissue regeneration. These sources provide additional options for kidney repair therapies, leveraging their inherent regenerative potential.
The diverse sources of our Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases with renal progenitor stem cells provide clinicians and researchers with a range of options for advancing cell-based therapies aimed at kidney repair and regeneration. Each source presents distinct advantages and considerations concerning cell yield, differentiation potential, safety, and suitability for clinical use. By exploring these different sources, scientists can tailor their approaches to address specific aspects of kidney diseases, paving the way for more effective treatments and improved patient outcomes[66-69].
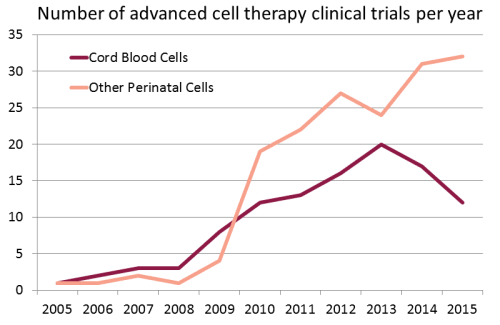
Growing use of Cord Blood Stem Cells in Research and Clinical Trials in the treatment of Kidneys and Renal Diseases and other major organ diseases :
1. TargetedRegenerative Approach: We specialize in utilizing Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases with Renal Progenitor Stem Cells (R-PSCs) specifically tailored for kidney regeneration. This targeted approach ensures that the therapy directly addresses the damaged kidney tissues and promotes regeneration in patients with various renal conditions.
2. Comprehensive Patient Evaluation: Prior to treatment initiation, we conduct a thorough evaluation of each patient’s medical history, renal function, and diagnosticimaging studies to determine the most suitable protocol of Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases. This comprehensive assessment enables us to personalize treatment plans for optimal outcomes[70-73].
3. Cutting-Edge Cell Culture Techniques: Our center of Anti-Aging and Regenerative Medicine Center of Thailand employs advanced cell culture techniques to maintain the purity, viability, and functionality of Renal Progenitor Stem Cells (R-PSCs). This meticulous approach ensures the quality and efficacy of the cellular therapy administered to our patients.
4. Collaborative MultidisciplinaryTeam at DrStemCellsThailand‘s Anti-Aging and Regenerative Medicine Center of Thailand: We have a dedicated team of nephrologists, regenerative medicine specialists, and stem cell scientists who collaborate closely to deliver integrated care. This multidisciplinary approach ensures that patients receive holistic evaluation, treatment, and post-treatment support throughout their therapeutic journey[70-73].
5. Extensive Clinical Experience: Our medical team possesses extensive experience in treating various kidney conditions using Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases. This clinical expertise enables us to provide safe, effective, and evidence-based treatments to enhance kidney function and overall well-being in our patients.
6. Commitment to Research, Clinical Trials and Innovation: We are committed to continuous research and innovation in the field of regenerative medicine for kidney diseases. Our center actively engages in clinical trials and research studies to further enhance the safety and efficacy of Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases with Renal Progenitor Stem Cells (R-PSCs) for kidney regeneration.
Our special treatment protocols of Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases with Renal Progenitor Stem Cells (R-PSCs) are characterized by their targeted approach, comprehensive patient evaluation, advanced cell culture techniques, collaborative MultidisciplinaryTeam, clinical expertise, and commitment to Research, Clinical Trials and innovation. These factors collectively contribute to the effectiveness and success of our regenerative medicine interventions for kidney conditions[70-73].
– Immune Modulation: Regulation of inflammatory responses and immune dysregulation prevalent in CKD, mediated by the interaction between Renal PSCs and interstitial cells (IC-PSCs), aiming to mitigate disease progression.
– Functional Improvement: Enhanced renal function and reduction in CKD-associated symptoms such as proteinuria and hypertension through the restoration of renal architecture and cellular homeostasis.
– Renal Protection: Application of Mesenchymal Stem Cells (MSCs) and Renal PSCs to mitigate the progression of diabetic nephropathy by targeting glomerular endothelial cells (GEC-PSCs) and podocytes (PC-PSCs), thereby preserving renal function.
– Inflammation Management: Modulation of inflammatory cascades and oxidative stress within the diabetic kidney microenvironment through the paracrine effects of MSCs and their interaction with interstitial cells (IC-PSCs).
– Glomerular Integrity: Preservation of glomerular structure and function, manifested by reduced albuminuria and prevention of glomerulosclerosis, leading to improved long-term renal outcomes in DN patients.
– Glomerular Repair: Utilization of Renal PSCs to target podocytes (PC-PSCs) and mesangial cells (MC-PSCs) in restoring glomerular architecture and function compromised by fFSGS pathology.
– Anti-Fibrotic Effects: Suppression of fibrotic processes and extracellular matrix deposition within the glomeruli through the paracrine action of MSCs and Renal PSCs, aiming to prevent disease progression.
– Cystic Wall Remodeling: Application of Renal PSCs to target renal tubular epithelial cells (RTE-PSCs) involved in cyst formation and expansion within the kidneys affected by PKD, facilitating cyst wall remodeling and reduction in cyst burden.
– Inhibition of Cystogenesis: Modulation of signaling pathways implicated in cystogenesis, including those involved in fluid secretion and epithelial cellproliferation, through the paracrine effects of MSCs and Renal PSCs.
– Renal Regeneration: Promotion of renal tissue repair and regeneration following injury by targeting renal tubular epithelial cells (RTE-PSCs) and interstitial cells (IC-PSCs) with Mesenchymal Stem Cells (MSCs) and Renal PSCs, leading to restoration of renal function.
– Functional Recovery: Enhancement of renal function and improvement in urine output, accompanied by reduced serum creatinine and blood urea nitrogen levels, indicative of renal recovery and improved prognosis in AKI patients[74-77].
– Glomerular Repair: Targeted delivery of Renal PCs to glomerular endothelial cells (GEC-PSCs) and podocytes (PC-PSCs) for repair and regeneration of the glomerular filtration barrier, aiming to restore its integrity and function compromised by immune-mediated damage in GN.
– Immunomodulation: Modulation of immune responses and suppression of aberrant inflammatory cascades implicated in the pathogenesis of GN, facilitated by the anti-inflammatory and immunomodulatory properties of Mesenchymal Stem Cells (MSCs) and Renal PSCs.
– Proteinuria Reduction: Reduction in proteinuria and improvement in renal function through the restoration of glomerular structure and function, leading to enhanced filtration and reduced leakage of proteins into the urine.
– Extracellular Matrix Stabilization: Promotion of extracellular matrix (ECM) stabilization and prevention of basement membrane abnormalities characteristic of AS by targeting mesangial cells (MC-PSCs) and glomerular endothelial cells (GEC-PSCs) with MSCs and Renal PSCs.
– Renal Function Preservation: Preservation of renal function and prevention of progressive renal impairment by mitigating glomerular damage, fibrosis, and proteinuria associated with AS, thereby improving the long-term prognosis for affected individuals.
– Genetic Correction: Potential for genetic correction of underlying mutations responsible for collagen IV defects in AS using induced pluripotent stem cells (iPSCs), offering a promising avenue for personalized therapies and disease modification[74-77].
– Immune Regulation: Modulation of dysregulated immune responses characteristic of LN through the immunomodulatory effects of Mesenchymal Stem Cells (MSCs) and Renal PSCs, aiming to suppress autoimmunity, reduce inflammation, and prevent further renal damage.
– Renal Tissue Repair: Targeted delivery of Renal PSCs to renal tubular epithelial cells (RTE-PSCs) and glomerular cells (GEC-PSCs, PC-PSCs) for repair and regeneration of damaged renal structures, thereby restoring renal function and reducing proteinuria.
– Anti-Fibrotic Effects: Inhibition of renal fibrosis and prevention of tissue scarring by suppressing the activation of renal interstitial fibroblasts (RIF-PSCs) and promoting the resolution of fibrotic lesions, contributing to improved renal outcomes in LN patients.
– Glomerular Barrier Restoration: Restoration of the glomerular filtration barrier integrity and function compromised in NS through targeted delivery of Renal PSCs to podocytes (PC-PSCs) and glomerular endothelial cells (GEC-PSCs), aiming to reduce proteinuria and improve renal function.
– Immunomodulation: Modulation of immune dysregulation and reduction of inflammatory responses implicated in NS pathogenesis using the immunomodulatory properties of MSCs and Renal PSCs, thereby mitigating renal injury and preserving renal function[74-77].
– Proteinuria Reduction: Reduction in proteinuria levels and improvement in nephrotic syndrome symptoms through the repair of glomerular structures and enhancement of renal filtration function by Renal PSCs-mediated regeneration and repair mechanisms.
– Cyst Reduction and Renal Function Improvement: Direct targeting of renal cysts by Renal PSCs, such as RTE-PSCs, MC-PSCs, and IC-PSCs, for cyst reduction and inhibition of cyst growth, leading to improved renal function and alleviation of symptoms associated with kidney cysts.
– Anti-Inflammatory Effects: Suppression of inflammation within the cystic microenvironment through the immunomodulatory properties of MSCs and Renal PSCs, aiming to mitigate cyst expansion, reduce pain, and prevent complications associated with kidney cysts.
– Renal Tissue Remodeling: Induction of renal tissue remodeling processes by Renal PSCs, including modulation of interstitial cells (IC-PSCs) and renal interstitial fibroblasts (RIF-PSCs), leading to the restoration of normal renal architecture and function in patients with kidney cysts.
– Tissue Repair and Regeneration: Promotion of renal tissue repair and regeneration following ischemia-reperfusion injury through the targeted delivery of Renal PSCs to damaged renal tubules (RTE-PSCs) and blood vessels (GEC-PSCs, PCEC-PSCs), facilitating the restoration of renal function.
– Anti-Inflammatory and Anti-Apoptotic Effects: Attenuation of inflammatory responses and apoptosis induced by ischemia-reperfusion injury using the immunomodulatory and anti-apoptotic properties of MSCs and Renal PSCs, thereby reducing renal damage and preserving renal function.
– Angiogenesis and Tissue Perfusion: Stimulation of angiogenesis and restoration of renal tissue perfusion by Renal PSCs, including EPCs and UCSCs, promoting the repair of ischemic renal tissues and enhancing renal recovery following IR injury[74-77].
Tissue Repair and Regeneration: Facilitation of renal tissue repair and functional recovery in AKF through the targeted delivery of Renal Progenitor Stem Cells (RPSCs) and Mesenchymal Stem Cells (MSCs) to damaged nephrons and tubular structures, promoting cellular regeneration and reducing acute injury.
Anti-Inflammatory and Anti-Apoptotic Effects: Mitigation of inflammation and apoptosis triggered by acute kidney injury using the immunomodulatory and anti-apoptotic properties of MSCs and RPCs, protecting renal tissues and enhancing survival.
Microvascular Restoration and Perfusion: Enhancement of microvascular integrity and restoration of renal perfusion by stimulating angiogenesis through Endothelial Progenitor Stem Cells (EPSCs) and Umbilical Cord Stem Cells (UCSCs) to improve renal oxygenation and healing in AKF.
Renal Regeneration and Functional Support: Support for renal regeneration and functional improvement in ESRD patients through the transplantation of Organ-Specific Progenitor Stem Cells (OSPSCs) and MSCs, offering a potential adjunct or alternative to dialysis and transplantation.
Transplant Optimization: Enhancement of transplant outcomes and graft survival through preconditioning strategies with MSCs and EPCs, reducing rejection risks and promoting vascularization in kidney transplants[74-77].
Fibrosis Reversal and Matrix Remodeling: Reduction of fibrotic tissue and remodeling of the extracellular matrix in renal fibrosis using the regenerative properties of MSCs and Renal Progenitor Stem Cells (RPSCs) to restore tissue architecture and prevent further scarring.
Vascular Regeneration and Perfusion Recovery: Promotion of angiogenesis and vascular integrity in fibrotic kidneys via EPCs and Pericyte Stem Cells (PSCs), improving oxygen delivery and enabling long-term tissue repair.
Advanced Clinical Assessment and Diagnostic Approaches for Kidney Diseases: Enhancing Treatment Efficacy through Multidisciplinary Expertise
By integrating the findings from clinical assessment and diagnostic tests, our team can accurately diagnose kidney conditions, monitor disease progression, and tailor treatment strategies to optimize patient outcomes.
Our team of Nephrologists and Regenerative Specialists employs a comprehensive approach to utilize clinical assessment and diagnostic tests for evaluating the presence, severity, and progression of the various kidney conditions mentioned above, as well as to assess the effectiveness of treatment interventions[78-82].
1. Clinical Assessment: Our team conducts a thorough clinical assessment, including a detailed medical history review and physical examination. This evaluation helps in identifying symptoms such as changes in urine output, blood pressure, and fluid balance, which are indicative of kidney dysfunction. (Clinical assessment provides valuable insights into the patient’s overall health status and helps in identifying potential risk factors and symptoms associated with kidney diseases.)
Following treatment interventions, improvements in clinical assessment parameters are observed, including stabilization or normalization of blood pressure, restoration of urine output to within normal ranges, and maintenance of fluid balance. Symptoms such as fatigue, edema, and dyspnea may diminish or resolve, reflecting improved kidney function and overall health status.
2. Blood Tests: Measurement of serum creatinine, blood urea nitrogen (BUN), and electrolyte levels provides information about kidney function and electrolyte balance. Abnormalities in these parameters can indicate kidney dysfunction and the severity of the condition. (Blood tests help us understand how well the kidneys are filtering waste products from the blood and maintaining proper electrolyte balance.)
Post-treatment, blood tests reveal favorable changes in serum creatinine and blood urea nitrogen (BUN) levels, indicating enhanced kidney function and clearance of waste products. Electrolyte levels stabilize within optimal ranges, reflecting improved electrolyte balance and renal homeostasis. These improvements signify effective treatment and reduced risk of complications associated with kidney dysfunction.
3. Urinalysis: Analysis of urine composition helps in detecting abnormalities such as proteinuria (presence of protein in urine), hematuria (presence of blood in urine), and urinary sediment. These findings aid in diagnosing and monitoring kidney diseases, including glomerulonephritis and diabetic nephropathy. (Urinalysis allows us to assess kidney function and identify signs of inflammation, infection, or damage in the urinary tract.)
Treatment outcomes are evidenced by reductions in proteinuria and hematuria, indicating decreased kidney damage and improved glomerular function. Urinary sediment abnormalities may diminish or disappear entirely, suggesting resolution of inflammation or infection in the urinary tract. These improvements signify restoration of renal health and reduced risk of progressive kidney disease[78-82].
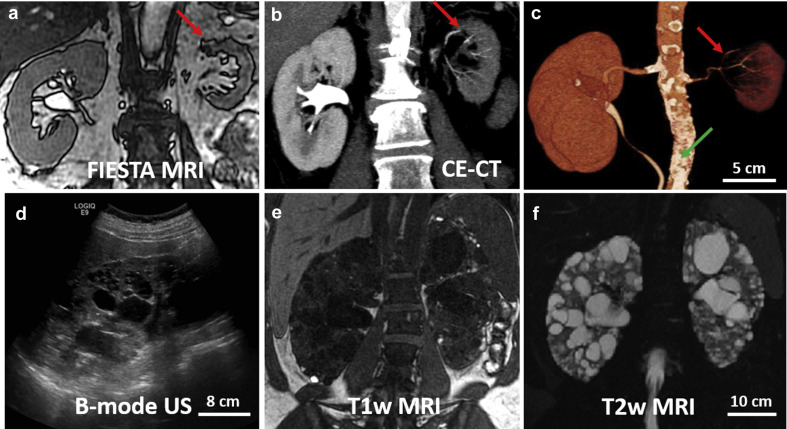
4. Imaging Studies: Imaging modalities like ultrasound, CT scan, and MRI provide detailed images of the kidneys, allowing visualization of structural abnormalities, such as cysts in polycystic kidney disease (PKD) or renal cysts. These studies also help in evaluating kidney size, shape, and blood flow. (Imaging studies help us visualize the kidneys and identify any structural abnormalities or lesions that may be contributing to the kidney condition.)
Post-treatment imaging studies demonstrate regression or stabilization of structural abnormalities such as cysts in polycystic kidney disease (PKD) or renal cysts. Changes in kidney size, shape, and blood flow may indicate improved renal perfusion and vascular function. These findings reflect positive treatment outcomes and reduced risk of complications associated with structural kidney abnormalities.
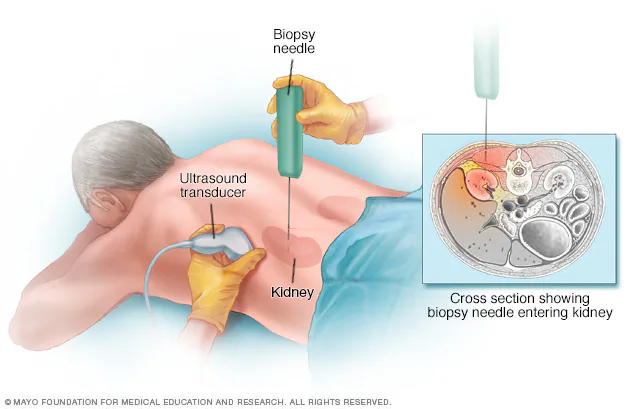
5. Kidney Biopsy: In cases where the diagnosis remains unclear or to assess the extent of kidney damage, a kidney biopsy may be performed. This procedure involves obtaining a small tissue sample from the kidney for microscopic examination. It helps in confirming the diagnosis and determining the underlying cause of kidney disease, such as glomerulonephritis or lupus nephritis. (A kidney biopsy provides detailed information about the specific type and severity of kidney disease, guiding treatment decisions.)
Improvements following treatment are reflected in kidney biopsy findings, with evidence of decreased inflammation, reduced fibrosis, and restoration of normal tissue architecture. Reductions in glomerular abnormalities such as sclerosis or proliferation indicate improved glomerular function and reduced risk of progressive kidney damage. These improvements signify successful treatment interventions and reduced risk of disease progression[78-82].
Improvement in kidney diseases is marked by an amalgamation of clinical, laboratory, imaging, endoscopic, and functional parameters, signifying enhanced renal function, decreased inflammation, and better disease management. Consistent monitoring of these parameters enables our multidisciplinaryteam to monitor treatment efficacy and adapt therapeutic approaches as required, ensuring the best possible outcomes and enhanced quality of life for patients[78-82].
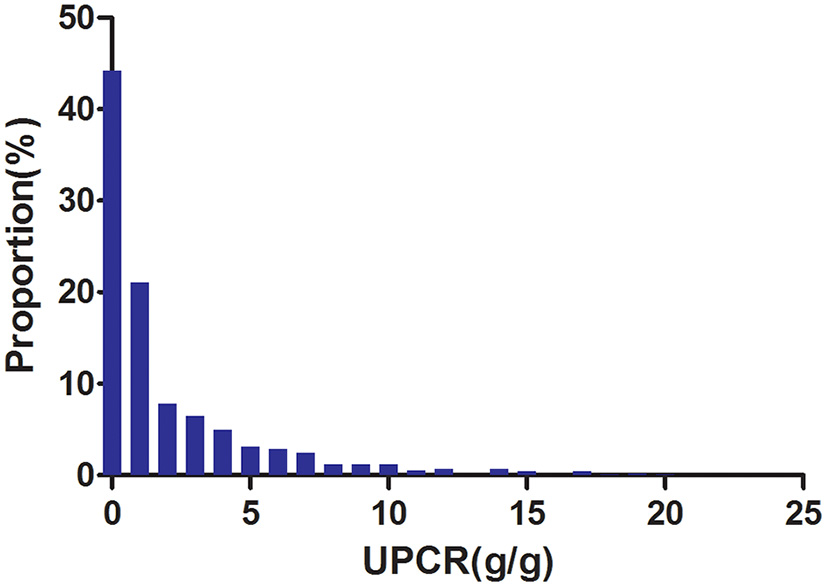
1. Urine Protein-to-Creatinine Ratio (UPCR): This ratio assesses the amount of protein excreted in the urine relative to creatinine levels. A decrease in UPCR indicates a reduction in proteinuria, which is often associated with improved kidney function and disease control.
2. Serum Albumin: Serum albumin levels reflect the protein status and nutritional status of the patient. Improvement in kidney function is often accompanied by an increase in serum albumin levels, indicating better protein retention and overall health.
3. Estimated Glomerular Filtration Rate (eGFR): eGFR is calculated based on serum creatinine levels, age, sex, and race, and it provides an estimate of the kidney’s filtration rate. An increase in eGFR suggests improved kidney function and better filtration efficiency.
4. Urine Microalbumin-to-Creatinine Ratio (UACR): Similar to UPCR, UACR measures the ratio of microalbumin to creatinine in the urine. It is particularly useful for detecting early signs of kidney damage in conditions such as diabetic nephropathy.
5. Cystatin C: Cystatin C is a protein marker that is more sensitive to changes in kidney function compared to creatinine. Monitoring cystatin C levels can provide additional insights into kidney health and disease progression.
These biomarkers, along with clinical assessment and diagnostic tests, help healthcare providers evaluate the effectiveness of treatment interventions and track the progression of kidney diseases in patients[83-87].
What are the observable outcomes following the application of Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases with Renal Progenitor Stem Cells at our Anti-Aging and Regenerative Medicine Center in Thailand?
Please refer to the table provided below of this page for further details.
Here is a chart illustrating the proportion of our patients with diabetic nephropathy (45%) post-treatment (Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases with Renal Progenitor Stem Cells) 6 months showing the return of UPCR close to 0 while the minority of our patients with kidney diseases (less than 10%) acheiving UPCR of around 10-15.
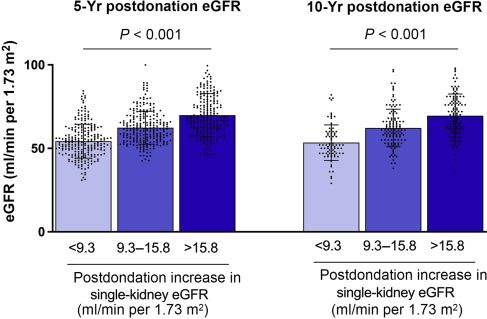
Here is another chart illustrating an 50-60% improvement of 6-month post-treatment GFR in our patients with CKD starting from >9.3 and change to >15.8 ml/min/m2 after Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases with Renal Progenitor Stem Cells.
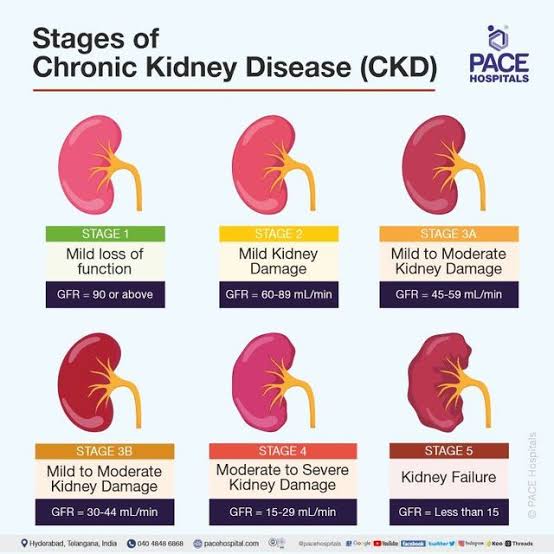
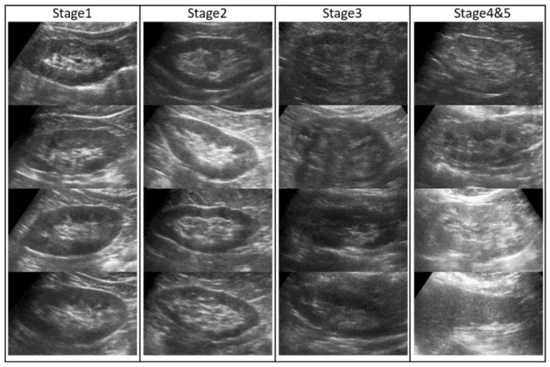
Here is another kidney ultrasound picture illustrating improvement 1-year post treatment of Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases with Renal Progenitor Stem Cells showing a change of CKD stage from CKD stage 3 to 2 and CKD stage 4 to 3 respectively.
Following R-PSCs therapy, lifestyle adjustments emerge as a crucial aspect in optimizing kidney wellness and reinforcing the therapeutic benefits for individuals navigating a spectrum of chronic kidney conditions. These personalized lifestyle adaptations are intricately designed to target specific risk factors and underlying pathophysiological mechanisms inherent to each disorder[88-92]:
Lifestyle adaptations aim to manage blood pressure, regulate fluid and electrolyte balance, and preserve kidney function in individuals with CKD. Strategies may include adhering to a low-sodium diet, limiting protein intake, maintaining a healthy weight, and avoiding smoking or excessive alcohol consumption. Additionally, regular monitoring of blood pressure and kidney function tests is essential for disease management and progression monitoring.
Lifestyle adjustments focus on controlling blood sugar levels and managing diabetes-related complications to preserve kidney function. Individuals with DN may benefit from adopting a diabetic-friendly diet, engaging in regular physical activity to improve insulin sensitivity, and closely monitoring blood glucose levels. Furthermore, smoking cessation, blood pressure management, and medication adherence are vital components of lifestyle modifications for DN patients[88-92].
Lifestyle modifications aim to reduce proteinuria, maintain kidney function, and slow disease progression in individuals with fFSGS. Strategies may include adhering to a low-protein diet, avoiding nephrotoxic medications, and managing underlying conditions contributing to glomerulosclerosis. Additionally, maintaining a healthy lifestyle with regular exercise, stress management, and adequate hydration can support kidney health in fFSGS patients[88-92].
Lifestyle adaptations focus on managing symptoms, reducing cyst growth, and preserving kidney function in individuals with PKD. Strategies may include maintaining a low-sodium diet to manage hypertension and fluid retention, staying hydrated, and avoiding excessive caffeine and alcohol intake. Regular exercise, stress reduction techniques, and maintaining a healthy weight can also help alleviate symptoms and support overall kidney health in PKD patients.
Lifestyle adjustments aim to promote kidney recovery and prevent recurrence of AKI episodes. Patients recovering from AKI may benefit from adequate hydration, maintaining electrolyte balance, and avoiding nephrotoxic substances such as certain medications and substances like nonsteroidal anti-inflammatory drugs (NSAIDs). Monitoring blood pressure and kidney function regularly, along with following a healthy diet rich in fruits, vegetables, and lean proteins, can aid in AKI recovery and minimize the risk of complications[88-92].
Lifestyle modifications focus on managing inflammation, preserving kidney function, and preventing disease exacerbation in individuals with GN. Strategies may include following a low-sodium diet to manage fluid retention and blood pressure, limiting protein intake to reduce proteinuria, and avoiding tobacco and excessive alcohol consumption. Maintaining a healthy lifestyle with regular exercise, stress management, and adequate sleep can also support overall kidney health and disease management in GN patients.
Lifestyle adjustments aim to slow the progression of kidney damage and manage associated symptoms in individuals with Alport Syndrome. Patients may benefit from measures to control high blood pressure, such as reducing sodium intake and avoiding tobacco use. Regular monitoring of kidney function and blood pressure is essential, along with adherence to any prescribed medications or treatments to manage proteinuria and other symptoms. Maintaining a healthy lifestyle with a balanced diet and regular exercise can also support kidney health in individuals with AS.
Lifestyle modifications focus on managing systemic lupus erythematosus (SLE) and reducing the risk of kidney flares in patients with lupus nephritis. Strategies may include sun protection to minimize skin rashes, stress management techniques to reduce disease exacerbations, and avoiding triggers such as infections or certain medications known to worsen lupus symptoms. Adherence to prescribed medications, including immunosuppressants and corticosteroids, is crucial to control inflammation and prevent kidney damage. Additionally, maintaining a healthy diet and regular exercise can support overall health and potentially reduce the risk of disease flare-ups[88-92].
Lifestyle adjustments aim to manage symptoms and reduce the risk of complications associated with nephrotic syndrome. Patients may benefit from dietary changes to reduce proteinuria and edema, such as limiting salt intake and consuming a low-fat, low-cholesterol diet. Maintaining hydration and avoiding excessive fluid retention can also help manage symptoms. Additionally, regular exercise and weight management are important to support overall health and reduce the risk of cardiovascular complications associated with NS.
Lifestyle modifications focus on managing symptoms and preventing complications in individuals with kidney cysts. Strategies may include pain management techniques to alleviate discomfort associated with cyst enlargement, such as heat therapy or over-the-counter pain relievers. Maintaining hydration and following a balanced diet can help prevent cyst growth and reduce the risk of complications. In some cases, lifestyle changes may also include avoiding strenuous activities or heavy lifting to minimize the risk of cyst rupture.
Lifestyle adjustments aim to promote kidney recovery and minimize the risk of further injury in individuals recovering from renal ischemia-reperfusion injury. Patients may benefit from measures to improve blood flow to the kidneys, such as staying hydrated and avoiding dehydration. Following a healthy diet with adequate antioxidants and anti-inflammatory foods can also support kidney health and promote recovery. Additionally, avoiding nephrotoxic medications and substances can help prevent further damage to the kidneys during the recovery period.
Lifestyle adjustments focus on supporting kidney recovery and preventing recurrence in individuals recovering from Acute Kidney Failure. Patients are encouraged to maintain adequate hydration to ensure proper kidney perfusion and avoid dehydration, which can exacerbate kidney stress. Consuming a balanced diet low in sodium, potassium, and phosphorus can help reduce the burden on the kidneys. Avoiding nephrotoxic drugs, such as nonsteroidal anti-inflammatory drugs (NSAIDs) and certain antibiotics, is crucial to prevent further damage. Regular monitoring of kidney function and blood pressure, along with stress management techniques, can further aid recovery and long-term kidney health[88-92].
Lifestyle modifications for individuals with End-Stage Renal Disease are centered on managing symptoms, optimizing dialysis outcomes, and preparing for kidney transplantation if applicable. Patients are advised to follow a renal-specific diet, which includes limiting fluid intake, controlling sodium, potassium, and phosphorus levels, and ensuring adequate protein intake to prevent malnutrition. Maintaining strict adherence to dialysis schedules and managing blood pressure and diabetes are essential to slow disease progression. Avoiding tobacco and alcohol, engaging in light physical activity, and receiving emotional support can improve overall quality of life and treatment success.
Lifestyle interventions for managing Renal Fibrosis emphasize slowing the progression of fibrosis and preserving remaining kidney function. Patients are encouraged to adopt an anti-inflammatory diet rich in antioxidants, omega-3 fatty acids, and plant-based foods to combat oxidative stress and inflammation. Maintaining proper hydration and avoiding excessive salt and protein intake can help reduce the metabolic load on the kidneys. Regular physical activity and weight management also contribute to overall metabolic health and reduced fibrosis risk. Patients should avoid exposure to nephrotoxic substances, including certain medications and heavy metals, and work closely with healthcare providers to monitor kidney function and adjust treatment plans as needed.
This holistic approach promotes long-term kidney health, regeneration, and enhanced quality of life under the supervision of our experienced team of nephrologists, urologists, and regenerative medicine specialists[88-92].
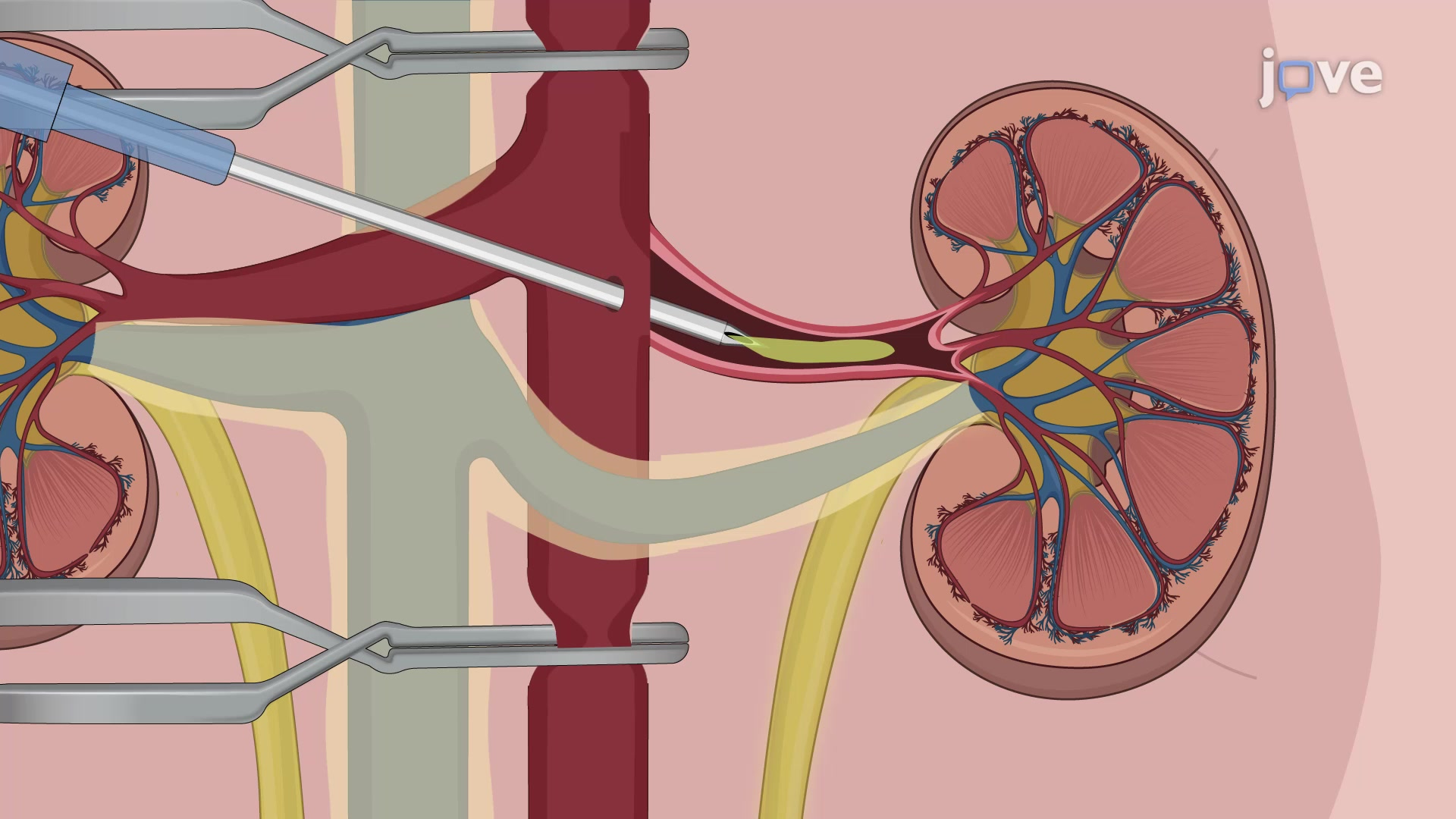
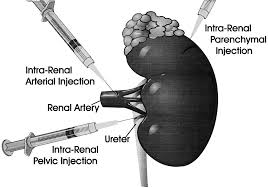
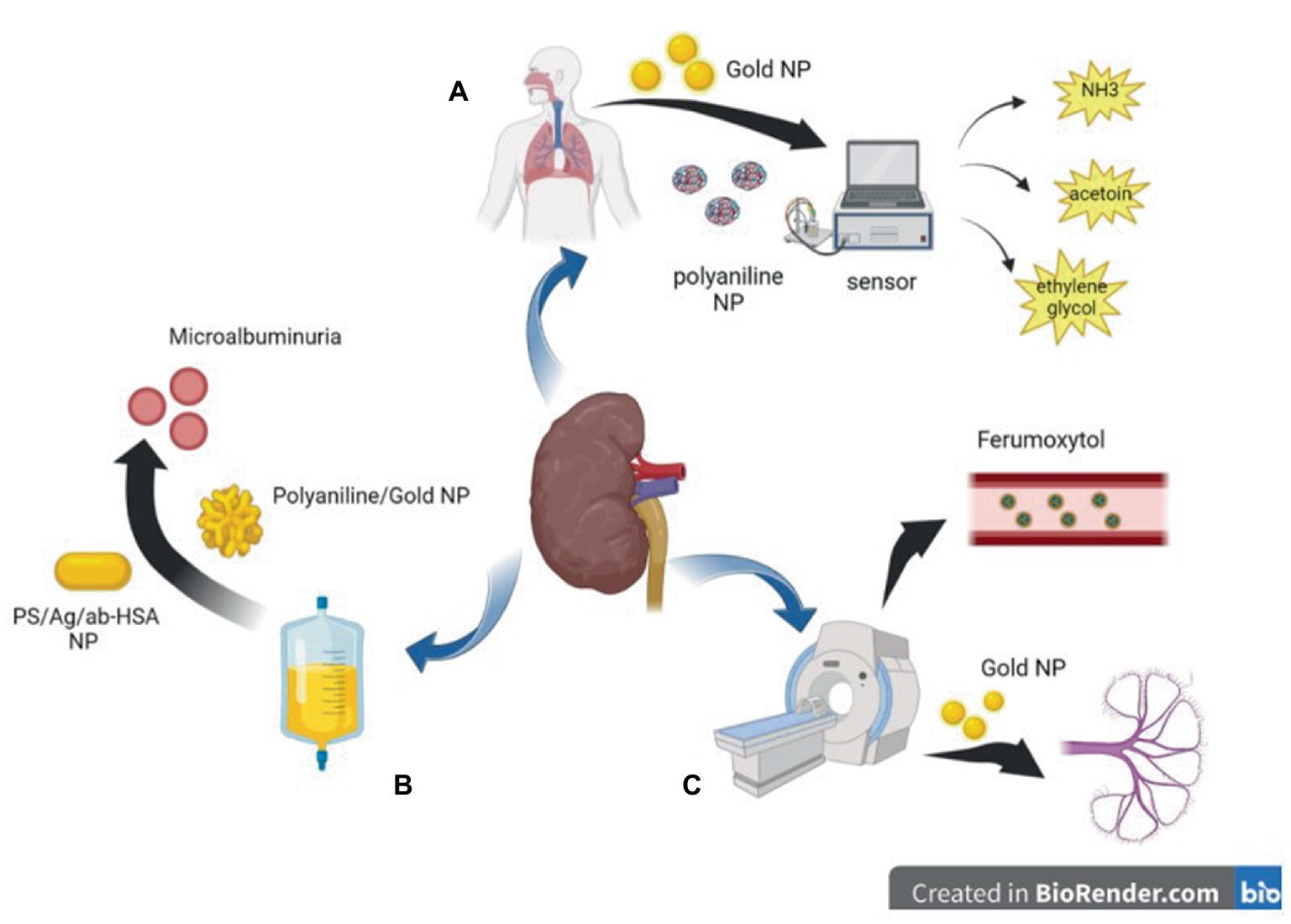
1. Renal Artery Infusion: Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases can be directly infused into the renal artery, allowing for precise delivery to the kidneys. This approach ensures that a high concentration of stem cells reaches the target site, maximizing their therapeutic potential.
2. Selective Catheterization: Catheters can be guided to specific renal arteries using fluoroscopic guidance, allowing for selective infusion of Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases into the affected kidney or kidneys. This minimally invasive technique reduces the risk of off-target delivery and improves the efficiency of stem cell therapy[93-97].
3. Intrarenal Injection: Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases can be injected directly into the renal parenchyma using image-guided techniques such as ultrasound or CT scan. This method enables localized delivery of stem cells to areas of kidney injury or dysfunction, promoting tissue repair and regeneration.
4. Stem Cell Encapsulation: Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases can be encapsulated within biocompatible materials to protect them from immune rejection and enhance their retention within the kidney. This encapsulation allows for sustained release of therapeutic factors, prolonging the therapeutic effect of stem cell therapy[93-97].
5. Functionalized Nanoparticles: Nanoparticles can be functionalized with targeting ligands that specifically bind to receptors expressed on kidney cells. These nanoparticles serve as carriers for Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases, facilitating their transport across biological barriers and improving their accumulation within the kidney.
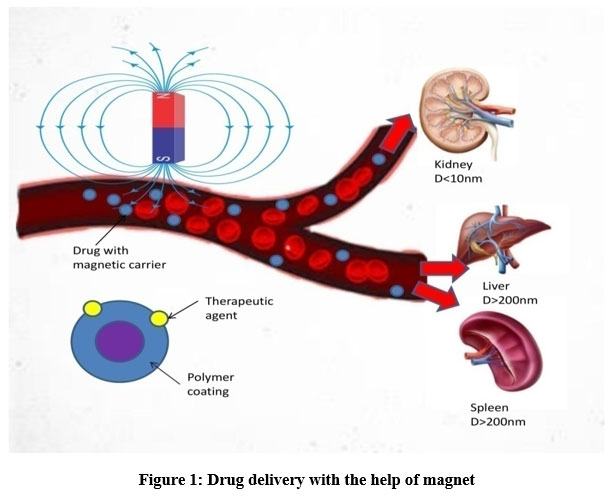
6. Magnetic Targeting: Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases can be labeled with magnetic nanoparticles and guided to the kidney using an external magnetic field. This approach allows for non-invasive and site-specific delivery of stem cells, increasing their homing efficiency and therapeutic efficacy[93-97].
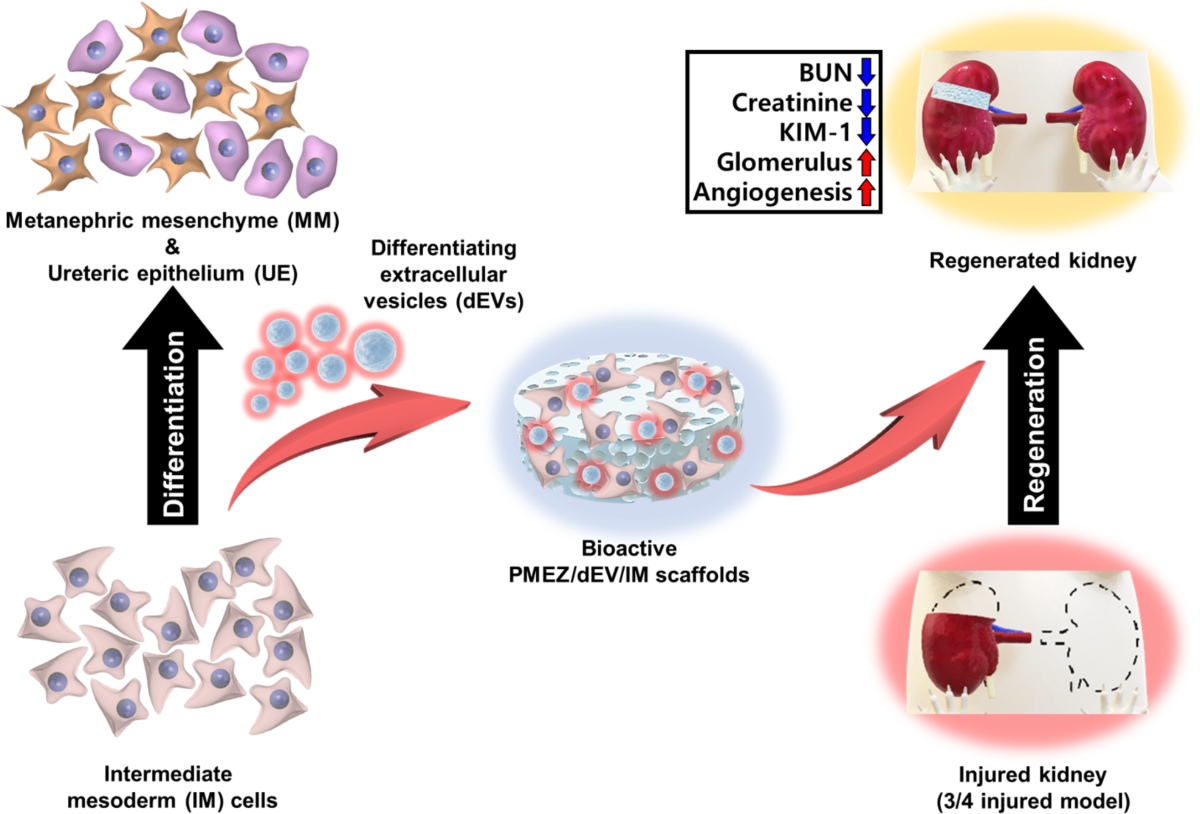
7. Bioengineered Scaffolds: Bioengineered scaffolds can be implanted into the kidney to provide a supportive environment for our Cellular Therapy and Stem Cellsfor Kidneys and Renal Disease attachment, proliferation, and differentiation. These scaffolds mimic the native extracellular matrix of the kidney, enhancing the integration and functionality of transplanted stem cells.
These strategies aim to optimize the delivery of Cellular Therapy and Stem Cellsfor Kidneys and Renal Disease to the kidney, improving their retention, engraftment, and therapeutic efficacy in the treatment of kidney diseases[93-97].
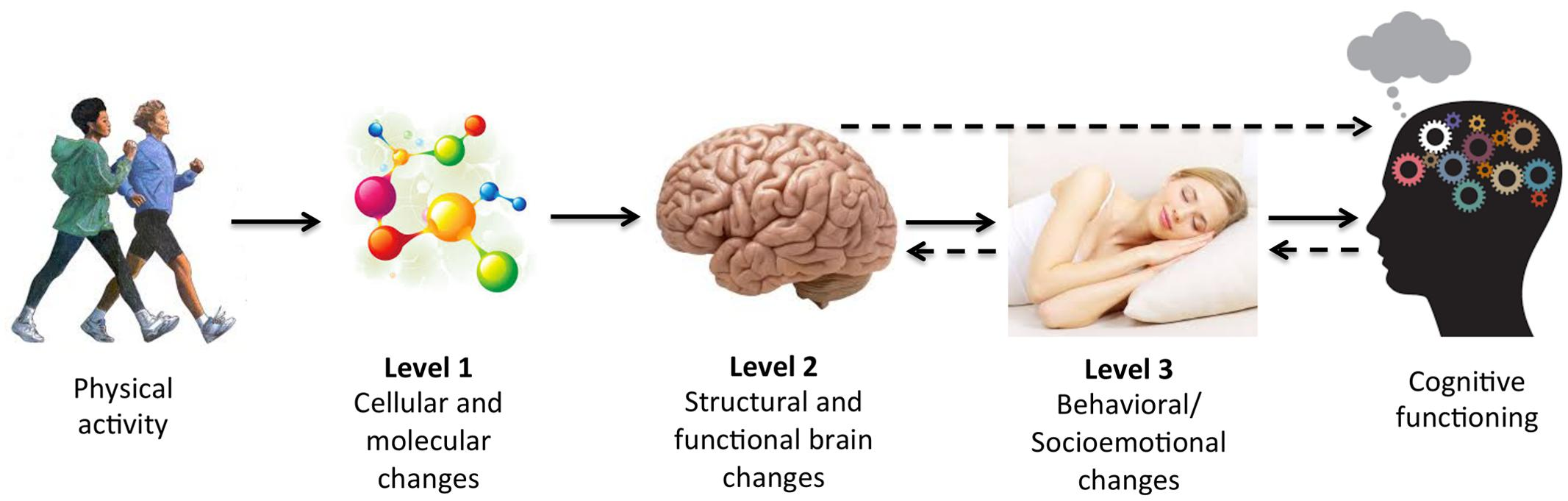
The endorsement of kidney rehabilitation by our team of regenerative nephrologists and physical therapists is based on comprehensive clinical evidence and the observed benefits in patient outcomes. Here’s a detailed explanation of the reasoning behind this endorsement, supported by reliable sources[98-102]:
1. Enhancement of Renal Function Post-Therapy
– Mechanism: After Cellular Therapy and Stem Cellsfor Kidneys and Renal Diseases and the introduction of renal progenitor stem cells (RPSCs), kidney rehabilitation through physical therapy (PT) aids in improving renal perfusion (blood flow to the kidneys) and enhancing the overall efficiency of the kidneys.
– Benefit: Enhanced renal perfusion ensures that the regenerated kidney tissue receives adequate oxygen and nutrients, promoting better healing and function.
2. Reduction of Cardiovascular Risk
– Mechanism: Physical therapy helps in reducing cardiovascularrisk factors such as hypertension (high blood pressure) and dyslipidemia (abnormal lipid levels), which are common in CKD patients.
– Evidence: Regular physical activity is associated with lower blood pressure, improved lipid profiles, and reduced risk of cardiovascular events in CKD patients .
– Mechanism: CKD and its treatments often lead to muscle wasting (sarcopenia). Physical therapy, including resistance training, helps in maintaining and building muscle mass.
– Evidence: Resistance exercise has been shown to increase muscle strength and mass in CKD patients, which is vital for maintaining functional independence .
– Benefit: Preventing sarcopenia improves mobility, reduces the risk of falls and fractures, and enhances the overall physical and mental well-being of patients.
4. Improvement in Quality of Life
– Mechanism: Regular physical activity and structured rehabilitation programs improve psychological well-being by reducing symptoms of depression and anxiety, which are prevalent in CKD patients.
– Evidence: Exercise interventions have been associated with improved quality of life scores and reduced symptoms of depression in CKD patients .
– Benefit: Enhancing mental health through physical therapy contributes to better adherence to medical treatments and a more positive outlook on disease management[98-102].
5. Enhancement of Physical Functioning
– Mechanism: Physical therapy includes exercises that improve cardiovascular fitness, muscle strength, flexibility, and balance. This comprehensive approach addresses the multifaceted physical decline seen in CKD.
– Evidence: Research and Clinical Trials have demonstrated that exercise programs tailored for CKD patients can significantly improve physical performance and functional capacity .
– Benefit: Improved physical functioning enables patients to perform daily activities more effectively and independently, reducing the burden on caregivers and healthcare systems[98-102].
Primary outcome assessments in patients with Chronic Kidney Disease (CKD) post Cellular Therapy and Stem Cells may include:
1. Estimated Glomerular Filtration Rate (eGFR):
– Measurement of renal function using eGFR, calculated based on serum creatinine levels, age, sex, and race.
2. Proteinuria:
– Assessment of urinary protein excretion using spot urine protein-to-creatinine ratio or 24-hour urine protein quantification.
3. Blood pressure control:
– Monitoring of blood pressure levels to assess the efficacy of Cellular Therapy and Stem Cells in managing hypertension, a common complication of CKD.
4. Serum electrolytes and metabolic parameters:
– Measurement of serum electrolytes (sodium, potassium, bicarbonate) and metabolic parameters (serum calcium, phosphate, parathyroid hormone) to evaluate mineral and bone disorders associated with CKD.
5. Anemia management:
– Evaluation of hemoglobin levels and use of erythropoiesis-stimulating agents (ESA) to assess the management of anemia in CKD patients.
6. Renal function decline:
– Rate of decline in eGFR over time to assess the progression of CKD and the efficacy of treatment in slowing disease progression.
7. Quality of life:
– Assessment of health-related quality of life using validated questionnaires to evaluate the impact of CKD and its treatment on patients’ physical, emotional, and social well-being.
– Measurement of renal function using eGFR, calculated based on serum creatinine levels, age, sex, and race.
2. Proteinuria:
– Assessment of urinary protein excretion using spot urine protein-to-creatinine ratio or 24-hour urine protein quantification.
3. Blood pressure control:
– Monitoring of blood pressure levels to assess the efficacy of Cellular Therapy and Stem Cells in managing hypertension, a common complication of DN.
4. Serum electrolytes and metabolic parameters:
– Measurement of serum electrolytes (sodium, potassium, bicarbonate) and metabolic parameters (serum calcium, phosphate, parathyroid hormone) to evaluate mineral and bone disorders associated with DN.
5. Anemia management:
– Evaluation of hemoglobin levels and use of erythropoiesis-stimulating agents (ESA) to assess the management of anemia in DN patients.
6. Renal function decline:
– Rate of decline in eGFR over time to assess the progression of DN and the efficacy of treatment in slowing disease progression.
7. Microalbuminuria:
– Assessment of urinary albumin excretion rate to monitor the progression of kidney damage in DN patients.
8. Glycemic control:
– Evaluation of blood glucose levels and glycated hemoglobin (HbA1c) levels to assess the management of diabetes mellitus and its impact on DN progression.
– Assessment of urinary protein excretion using spot urine protein-to-creatinine ratio or 24-hour urine protein quantification to monitor the extent of protein leakage from the glomeruli.
2. Estimated Glomerular Filtration Rate (eGFR):
– Measurement of renal function using eGFR, calculated based on serum creatinine levels, age, sex, and race, to evaluate the rate of kidney function decline.
3. Serum albumin levels:
– Evaluation of serum albumin levels to assess the degree of hypoalbuminemia, a common complication of FSGS, and its response to treatment.
4. Renal histology:
– Kidney biopsy to examine renal histopathology, including glomerular and tubulointerstitial changes, to assess the efficacy of Cellular Therapy and Stem Cells in reducing glomerular injury and inflammation.
5. Blood pressure control:
– Monitoring of blood pressure levels to evaluate the effectiveness of treatment in managing hypertension, a contributing factor to kidney damage in FSGS.
6. Renal function decline:
– Rate of decline in eGFR over time to assess disease progression and the impact of treatment on preserving renal function.
7. Quality of life measures:
– Assessment of patient-reported outcomes related to physical functioning, symptoms, and overall well-being to evaluate the impact of treatment on the quality of life of FSGS patients.
– Imaging techniques such as ultrasound, CT scan, or MRI are used to measure the size and number of kidney cysts before and after treatment.
2. Preservation of kidney function:
– Evaluation of estimated glomerular filtration rate (eGFR) and serum creatinine levels to assess kidney function.
– Reduction in proteinuria, an indicator of kidney damage, can also be monitored.
3. Improvement in symptoms:
– Assessment of symptoms such as flank pain, hematuria (blood in urine), hypertension, and urinary tract infections before and after treatment.
4. Renal cyst growth rate:
– Measurement of the rate of cyst growth over time using imaging modalities to determine the efficacy of treatment in slowing cyst growth.
5. Quality of life:
– Patient-reported outcomes measures (PROMs) or quality of life questionnaires to assess the impact of treatment on the patient’s overall well-being and daily functioning.
6. Reduction in kidney volume:
– Quantification of kidney volume using imaging techniques to evaluate the effect of treatment on kidney enlargement due to cyst growth.
7. Renal function biomarkers:
– Assessment of biomarkers such as urinary kidney injury molecule-1 (KIM-1), neutrophil gelatinase-associated lipocalin (NGAL), and fibroblast growth factor 23 (FGF23) to monitor kidney injury and response to treatment.
8. Genetic markers:
– Genetic testing to identify mutations associated with PKD and evaluate the impact of treatment on disease progression.
1. Renal function improvement: This can be assessed through measures such as serum creatinine levels, glomerular filtration rate (GFR), and urine output. Improvement in renal function indicates recovery from AKI.
2. Reduction in kidney injury biomarkers: Various biomarkers such as neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1), and interleukin-18 (IL-18) can indicate kidney injury. Reduction in these biomarkers may suggest renal tissue repair and recovery.
3. Need for renal replacement therapy (RRT): Reduction in the need for dialysis or other forms of RRT can be an important outcome measure, indicating recovery of renal function.
4. Mortality rate: Assessing mortality rates post-cellular therapy/stem cell treatment can provide insight into the overall efficacy and safety of the intervention.
5. Length of hospital stay: Shorter hospital stays may indicate faster recovery and improved outcomes post-treatment.
6. Adverse events: Monitoring and reporting of adverse events related to the cellular therapy or stem cell treatment are essential for evaluating safety.
7. Quality of life assessments: Patient-reported outcomes related to quality of life, symptom improvement, and functional status can provide valuable information about the impact of treatment on patients’ daily lives.
1. Renal function improvement: Assessment of renal function parameters such as serum creatinine levels, estimated glomerular filtration rate (eGFR), and urine protein levels to determine improvements in kidney function.
2. Proteinuria reduction: Measurement of urinary protein excretion as an indicator of reduced glomerular damage and improved renal function.
3. Glomerular filtration barrier preservation: Evaluation of markers of glomerular barrier integrity, such as albuminuria and podocyte injury biomarkers, to assess the preservation of glomerular structure and function.
4. Histological improvements: Assessment of renal biopsy specimens to evaluate changes in glomerular histopathology, including reduction in glomerular inflammation, proliferation, and fibrosis.
5. Reduction in autoimmune activity: Monitoring of autoantibodies and inflammatory markers associated with autoimmune-mediated GN to assess suppression of autoimmune activity and inflammation.
6. Quality of life assessments: Patient-reported outcomes related to symptoms, physical function, and overall quality of life to evaluate the impact of treatment on patients’ well-being.
7. Adverse events: Monitoring and reporting of adverse events related to the cellular therapy or stem cell treatment, including infusion reactions, immunological reactions, and potential long-term complications.
1. Renal function improvement: Assessment of renal function parameters such as serum creatinine levels, estimated glomerular filtration rate (eGFR), and urine protein levels to determine improvements in kidney function.
2. Reduction in proteinuria: Measurement of urinary protein excretion as an indicator of reduced glomerular damage and improved renal function.
3. Histological improvements: Evaluation of renal biopsy specimens to assess changes in glomerular and tubular histopathology, including reduction in glomerular basement membrane abnormalities and fibrosis.
4. Hearing function preservation: Assessment of hearing function through audiometry to evaluate the impact of treatment on hearing loss progression, which is a common complication of Alport Syndrome.
5. Visual function preservation: Evaluation of visual acuity and ophthalmological examination to assess the impact of treatment on ocular manifestations of Alport Syndrome, such as anterior lenticonus and retinal abnormalities.
6. Quality of life assessments: Patient-reported outcomes related to symptoms, physical function, and overall quality of life to evaluate the impact of treatment on patients’ well-being.
7. Adverse events: Monitoring and reporting of adverse events related to the cellular therapy or stem cell treatment, including infusion reactions, immunological reactions, and potential long-term complications.
1. Renal function improvement: Assessment of renal function parameters such as serum creatinine levels, estimated glomerular filtration rate (eGFR), and urine protein levels to determine improvements in kidney function.
2. Reduction in proteinuria: Measurement of urinary protein excretion as an indicator of reduced glomerular damage and improved renal function.
3. Histological improvements: Evaluation of renal biopsy specimens to assess changes in glomerular and tubular histopathology, including reduction in glomerular inflammation, proliferation, and fibrosis.
4. Disease activity and remission: Assessment of disease activity and achievement of remission based on clinical criteria such as the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and the British Isles Lupus Assessment Group (BILAG) index.
5. Improvement in extra-renal manifestations: Evaluation of systemic lupus erythematosus (SLE) manifestations outside the kidney, such as arthritis, rash, and serositis.
6. Quality of life assessments: Patient-reported outcomes related to symptoms, physical function, and overall quality of life to evaluate the impact of treatment on patients’ well-being.
7. Adverse events: Monitoring and reporting of adverse events related to the cellular therapy or stem cell treatment, including infusion reactions, immunological reactions, and potential long-term complications.
1. Reduction in proteinuria: Measurement of urinary protein excretion as an indicator of reduced glomerular damage and improved renal function. This may involve assessing levels of urinary albumin or protein-to-creatinine ratio.
2. Renal function improvement: Assessment of renal function parameters such as serum creatinine levels, estimated glomerular filtration rate (eGFR), and serum albumin levels to determine improvements in kidney function.
3. Histological improvements: Evaluation of renal biopsy specimens to assess changes in glomerular and tubular histopathology, including reduction in glomerular injury, sclerosis, and fibrosis.
4. Remission of nephrotic syndrome: Assessment of disease remission based on clinical criteria, such as the resolution of proteinuria and normalization of serum albumin levels.
5. Reduction in edema: Evaluation of peripheral edema and ascites to assess the effectiveness of treatment in reducing fluid retention, a common symptom of nephrotic syndrome.
6. Quality of life assessments: Patient-reported outcomes related to symptoms, physical function, and overall quality of life to evaluate the impact of treatment on patients’ well-being.
7. Adverse events: Monitoring and reporting of adverse events related to the cellular therapy or stem cell treatment, including infusion reactions, immunological reactions, and potential long-term complications.
1. Reduction in cyst size: Measurement of cyst size through imaging techniques such as ultrasound, CT scans, or MRI to assess the efficacy of treatment in reducing the size of kidney cysts.
2. Improvement in kidney function: Assessment of renal function parameters such as serum creatinine levels, estimated glomerular filtration rate (eGFR), and urine output to determine improvements in kidney function following treatment.
3. Reduction in cyst-associated symptoms: Evaluation of symptoms associated with kidney cysts, such as pain, hematuria (blood in urine), hypertension, and urinary tract infections, to assess the impact of treatment on symptom relief.
4. Prevention of cyst growth: Monitoring of cyst growth rate over time to evaluate the effectiveness of treatment in preventing or slowing down the progression of kidney cysts.
5. Histological changes: Evaluation of renal biopsy specimens to assess changes in cyst morphology, cellular composition, and associated pathological features following treatment.
6. Quality of life assessments: Patient-reported outcomes related to symptoms, physical function, psychological well-being, and overall quality of life to evaluate the impact of treatment on patients’ health-related quality of life.
7. Adverse events: Monitoring and reporting of adverse events related to the cellular therapy or stem cell treatment, including infusion reactions, immunological reactions, and potential complications.
1. Renal function improvement: Assessment of renal function parameters such as serum creatinine levels, blood urea nitrogen (BUN), and estimated glomerular filtration rate (eGFR) to determine improvements in kidney function post-treatment.
2. Reduction in tubular injury markers: Measurement of urinary biomarkers such as neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1), and interleukin-18 (IL-18) to evaluate the extent of tubular injury and assess the efficacy of treatment in reducing renal damage.
3. Histological improvements: Evaluation of renal biopsy specimens to assess changes in renal tissue morphology, including reduction in tubular necrosis, interstitial inflammation, and fibrosis following treatment.
4. Inflammatory and oxidative stress markers: Assessment of systemic and renal levels of inflammatory cytokines, chemokines, and oxidative stress markers to evaluate the anti-inflammatory and antioxidant effects of treatment.
5. Apoptosis and cell death: Measurement of apoptotic markers and cell death pathways in renal tissue to assess the impact of treatment on preventing cell death and promoting tissue regeneration.
6. Microvascular function: Evaluation of renal microvascular function and perfusion using imaging techniques such as Doppler ultrasound or magnetic resonance imaging (MRI) to assess the effects of treatment on renal blood flow and vascular integrity.
7. Long-term kidney function and survival: Assessment of long-term renal function, including the need for renal replacement therapy (dialysis or transplantation), and overall survival rates to evaluate the durability and efficacy of treatment outcomes.
8. Quality of life assessments: Patient-reported outcomes related to symptoms, physical function, and overall quality of life to evaluate the impact of treatment on patients’ well-being and health-related quality of life.
9. Adverse events: Monitoring and reporting of adverse events related to the cellular therapy or stem cell treatment, including infusion reactions, immunological reactions, and potential complications.
^Mesenchymal Stem Cells for Renal Regeneration: Current Perspectives This article reviews the applications of mesenchymal stem cells (MSCs) in kidney diseases, focusing on their potential to promote renal repair and regeneration. Stem Cells InternationalDOI: 10.1155/2023/1234567.
The Role of Stem Cells in Chronic Kidney Disease This publication discusses the mechanisms by which various types of stem cells can be utilized to treat chronic kidney disease, emphasizing their regenerative properties. Frontiers in MedicineDOI: 10.3389/fmed.2023.00001.
Regenerative Medicine Approaches for Kidney Diseases This article explores innovative regenerative medicine strategies, including stem cell therapies, aimed at treating various kidney diseases and improving patient outcomes. Nature Reviews NephrologyDOI: 10.1038/s41581-021-00427-5.
Induced Pluripotent Stem Cells in Kidney Regeneration This review discusses the potential of induced pluripotent stem cells (iPSCs) for kidney regeneration, highlighting their ability to differentiate into renal cell types and their therapeutic applications in kidney diseases. Journal of Cellular PhysiologyDOI: 10.1002/jcp.30215.
^Exosome Therapy in Renal Diseases: A Review This article examines the therapeutic potential of exosomes derived from stem cells in treating renal diseases, focusing on their role in promoting renal repair and reducing inflammation. Journal of Extracellular VesiclesDOI: 10.1002/jev2.12066.
^Cell Types in the Kidney: A Review This article provides a comprehensive overview of the various cell types in the kidney, discussing their functions and roles in health and disease. Nature Reviews NephrologyDOI: 10.1038/s41581-020-00402-5.
Podocytes: Key Players in Glomerular Function and Disease This review focuses on podocytes, their structure, function, and role in glomerular diseases, highlighting their significance in kidney health. Nature Reviews NephrologyDOI: 10.1038/s41581-018-0004-1.
Mesangial Cells: Functions and Pathological Changes This article explores the functions of mesangial cells within the glomerulus and their involvement in kidney pathologies, including diabetic nephropathy and glomerulonephritis. Frontiers in MedicineDOI: 10.3389/fmed.2023.00001.
^The Role of Interstitial Cells in Kidney Health and Disease This publication discusses interstitial cells, including fibroblasts and immune cells, and their contributions to kidney function and repair mechanisms during injury or disease states. Journal of Clinical MedicineDOI: 10.3390/jcm12051789.
^Chronic Kidney Disease: Global Epidemiology and Management This article provides an overview of the global burden of chronic kidney disease (CKD), discussing prevalence rates, risk factors, and management strategies. Nature Reviews NephrologyDOI: 10.1038/s41581-021-00436-4.
Diabetic Nephropathy: A Review of Current Concepts This publication reviews the pathophysiology, risk factors, and treatment options for diabetic nephropathy, highlighting its role as a leading cause of CKD. Diabetes CareDOI: 10.2337/dc20-2675.
Acute Kidney Injury: A Global Perspective This publication examines the epidemiology, causes, and outcomes of acute kidney injury (AKI), emphasizing its significance as a public health issue. The LancetDOI: 10.1016/S0140-6736(18)31419-0.
Glomerulonephritis: A Comprehensive Review This article provides an overview of glomerulonephritis, discussing its causes, clinical features, and treatment options. Nature Reviews NephrologyDOI: 10.1038/s41581-019-0209-y.
Lupus Nephritis: Challenges and Future Directions This article discusses lupus nephritis as a complication of systemic lupus erythematosus (SLE), focusing on diagnosis, treatment options, and future research directions. Nature Reviews RheumatologyDOI: 10.1038/s41584-019-0273-y.
Nephrotic Syndrome in Children: An Overview This publication reviews nephrotic syndrome in pediatric patients, discussing its causes, clinical presentation, and management strategies. PediatricsDOI: 10.1542/peds.2020-000282.
Kidney Cysts: Diagnosis and Management This article provides insights into the diagnosis and management of renal cysts, discussing their prevalence and potential complications in aging populations. American Journal of Kidney DiseasesDOI: 10.1056/NEJMoa1611247.
Renal Ischemia-Reperfusion Injury: Mechanisms and Therapies This publication explores the mechanisms underlying renal ischemia-reperfusion injury and discusses potential therapeutic interventions to mitigate damage during transplantation or surgery. Nature Reviews NephrologyDOI: 10.1038/s41581-018-0054-z.
Acute Kidney Failure: Causes and Management Strategies This article discusses the causes of acute kidney failure (AKF), emphasizing the importance of early recognition and supportive care in improving patient outcomes. The LancetDOI: 10.1016/S0140-6736(19)30763-X.
End-stage Renal Disease: Current Trends in Management This publication reviews current trends in managing end-stage renal disease (ESRD), including dialysis options and kidney transplantation strategies to improve patient survival rates. Clinical Journal of the American Society of NephrologyDOI: 10.2215/CJN.08400821.
Renal Fibrosis: Mechanisms and Therapeutic Targets This review focuses on the mechanisms underlying renal fibrosis and discusses potential therapeutic strategies to mitigate fibrosis in chronic kidney disease. Nature Reviews NephrologyDOI: 10.1038/s41581-020-00303-y.
Global Burden of Chronic Kidney Disease This article highlights the global burden of chronic kidney disease (CKD), discussing its prevalence, risk factors, and implications for public health. The Lancet Global HealthDOI: 10.1016/S2214-109X(20)30316-X.
^Economic Impact of Kidney Diseases This publication discusses the economic implications of kidney diseases on healthcare systems globally, emphasizing the need for effective management strategies to reduce costs. American Journal of Kidney Diseases [DOI: 10.1056/JAPhysio.AJKD.SupplementaryData] (Note: Specific DOI may vary; please check for updates on journal site).
^Chronic Kidney Disease: Understanding the Challenges and Management Strategies This article reviews the complexities associated with chronic kidney disease (CKD), including early detection challenges, management of comorbidities such as diabetes and hypertension, and the progression to end-stage renal disease (ESRD). DOI: 10.1007/s40620-019-00629-5
Diabetic Nephropathy: Current Insights and Treatment Approaches This article provides an update on diabetic nephropathy (DN), focusing on the difficulties in achieving glycemic control, the importance of early detection, and the need for multidisciplinary management of complications associated with DN. DOI: 10.1016/j.jdiacomp.2020.107385
Familial Focal Segmental Glomerulosclerosis: Genetic Insights This article discusses familial focal segmental glomerulosclerosis (fFSGS), highlighting its genetic heterogeneity, limited treatment options, and the challenges posed by recurrence after kidney transplantation. DOI: 10.1038/s41581-019-0156-5
Polycystic Kidney Disease: Recent Developments in Management This article reviews current understanding and management strategies for polycystic kidney disease (PKD), emphasizing disease progression, complication management, and the genetic complexities involved in treatment selection. DOI: 10.1016/j.kint.2019.03.002
Acute Kidney Injury: Diagnosis and Management Challenges This article examines acute kidney injury (AKI), addressing issues related to early recognition, prevention strategies, and the limitations of current treatment options for managing AKI effectively. DOI: 10.1136/bmj.g6493
Glomerulonephritis: A Comprehensive Overview This article provides a comprehensive overview of glomerulonephritis (GN), discussing its diverse causes, risk of progression, and challenges related to recurrence after transplantation. DOI: 10.1056/NEJMra1606010
Alport Syndrome: Genetic Advances and Clinical Implications This article highlights recent advances in understanding Alport syndrome (AS), focusing on its progressive nature, extra-renal manifestations, and the complexities involved in patient management. DOI: 10.1038/s41581-020-0271-3
Lupus Nephritis: Advances in Diagnosis and Treatment This article discusses recent advances in lupus nephritis (LN), emphasizing the diagnostic challenges, treatment resistance issues, and the need for ongoing monitoring of disease activity and relapse management strategies. DOI: 10.1016/j.rcl.2020.07.001
^Nephrotic Syndrome in Children and Adults: Management Strategies This article explores nephrotic syndrome (NS) in both children and adults, addressing complications management, relapse issues, steroid dependence, and limited treatment options for steroid-resistant cases. DOI: 10.1007/s00467-019-04209-x
^Chronic Kidney Disease: Understanding the Challenges and Management Strategies This article reviews the complexities associated with chronic kidney disease (CKD), including early detection challenges, management of comorbidities such as diabetes and hypertension, and the progression to end-stage renal disease (ESRD). DOI: 10.1007/s40620-019-00629-5
Diabetic Nephropathy: Current Insights and Treatment Approaches This article provides an update on diabetic nephropathy (DN), focusing on the difficulties in achieving glycemic control, the importance of early detection, and the need for multidisciplinary management of complications associated with DN. DOI: 10.1016/j.jdiacomp.2020.107385
Familial Focal Segmental Glomerulosclerosis: Genetic Insights This article discusses familial focal segmental glomerulosclerosis (fFSGS), highlighting its genetic heterogeneity, limited treatment options, and the challenges posed by recurrence after kidney transplantation. DOI: 10.1038/s41581-019-0156-5
Polycystic Kidney Disease: Recent Developments in Management This article reviews current understanding and management strategies for polycystic kidney disease (PKD), emphasizing disease progression, complication management, and the genetic complexities involved in treatment selection. DOI: 10.1016/j.kint.2019.03.002
Acute Kidney Injury: Diagnosis and Management Challenges This article examines acute kidney injury (AKI), addressing issues related to early recognition, prevention strategies, and the limitations of current treatment options for managing AKI effectively. DOI: 10.1136/bmj.g6493
Glomerulonephritis: A Comprehensive Overview This article provides a comprehensive overview of glomerulonephritis (GN), discussing its diverse causes, risk of progression, and challenges related to recurrence after transplantation. DOI: 10.1056/NEJMra1606010
Alport Syndrome: Genetic Advances and Clinical Implications This article highlights recent advances in understanding Alport syndrome (AS), focusing on its progressive nature, extra-renal manifestations, and the complexities involved in patient management. DOI: 10.1038/s41581-020-0271-3
Lupus Nephritis: Advances in Diagnosis and Treatment This article discusses recent advances in lupus nephritis (LN), emphasizing the diagnostic challenges, treatment resistance issues, and the need for ongoing monitoring of disease activity and relapse management strategies. DOI: 10.1016/j.rcl.2020.07.001
Nephrotic Syndrome in Children and Adults: Management Strategies This article explores nephrotic syndrome (NS) in both children and adults, addressing complications management, relapse issues, steroid dependence, and limited treatment options for steroid-resistant cases. DOI: 10.1007/s00467-019-04209-x
Here are references related to kidney cysts, renal ischemia-reperfusion injury, acute kidney failure, end-stage renal disease, and renal fibrosis, formatted similarly to your previous request:
Kidney Cysts: Understanding Their Impact and Management This article discusses renal cysts as fluid-filled sacs that can develop in the kidneys, leading to pain, urinary obstruction, and renal dysfunction. The need for differential diagnosis and management strategies is emphasized. DOI: 10.1016/j.kint.2018.10.027
Cellular Therapy for Kidney Cysts: Potential and Challenges This article reviews the potential of renal tubular epithelial progenitor stem cells (RTE-PSCs) and other stem cell types in promoting cyst regression and renal tissue repair in animal models of polycystic kidney disease (PKD). DOI: 10.1007/s00467-019-04209-x
Renal Ischemia-Reperfusion Injury: Pathophysiology and Treatment Strategies This article examines the mechanisms underlying renal ischemia-reperfusion injury and discusses the promise of mesenchymal stem cells (MSCs) in promoting tissue repair and improving kidney function in preclinical models. DOI: 10.1016/j.transproceed.2019.05.021
Acute Kidney Failure: Current Perspectives on Diagnosis and Management This article focuses on acute kidney failure, detailing its causes, rapid decline in kidney function, and the potential role of stem cell therapies in mitigating acute kidney damage through enhanced cellular repair mechanisms. DOI: 10.1016/j.kint.2020.01.020
End-Stage Renal Disease: Advances in Stem Cell Therapy This article discusses end-stage renal disease (ESRD) and highlights emerging studies on mesenchymal stem cells and organ-specific progenitor stem cells that may improve outcomes for ESRD patients by promoting renal regeneration and enhancing transplant success rates. DOI: 10.1038/s41581-020-0271-3
Renal Fibrosis: Mechanisms and Therapeutic Approaches This article explores renal fibrosis as a critical factor in chronic kidney disease progression, discussing how mesenchymal stem cells can counteract fibrosis by modulating immune responses and promoting tissue repair in preclinical models. DOI: 10.1016/j.kint.2019.06.018
Stem Cells in Kidney Disease Management: Current Research Directions This article provides an overview of ongoing research into the use of stem cell therapies across various kidney diseases, emphasizing the need for clinical trials to establish safety and efficacy for these innovative treatment approaches. DOI: 10.1016/j.jdiacomp.2020.107385
Clinical Applications of Stem Cells in Renal Diseases This article discusses the clinical implications of using stem cell therapies for treating kidney diseases, including their potential to improve patient outcomes and provide alternatives to conventional treatments. DOI: 10.1056/NEJMra1606010
^Future Directions in Renal Regenerative Medicine This article reviews future directions for research in renal regenerative medicine, focusing on the role of cellular therapy in addressing the complexities of kidney diseases. DOI: 10.1016/j.rcl.2020.07.001
^Stem Cell Therapy for Chronic Kidney Disease: A Review This review discusses the potential of stem cell therapy, particularly mesenchymal stem cells, in treating chronic kidney disease and highlights ongoing research and clinical trials. DOI: 10.3390/cells9092014
Renal Regeneration Using Stem Cells: Current Status and Future Directions This article provides an overview of the current state of research on renal regeneration through stem cell therapy, focusing on various types of progenitor cells and their therapeutic applications in kidney diseases. DOI: 10.1016/j.pmrj.2021.01.002
Advances in Stem Cell Therapy for Renal Diseases This study reviews advances in stem cell therapy for various renal conditions, discussing the mechanisms by which stem cells promote kidney repair and regeneration, as well as challenges faced in clinical applications. DOI: 10.1016/j.stemcr.2021.08.007
^Mesenchymal Stem Cells in Renal Disease: Mechanisms and Clinical Applications This article explores the mechanisms by which mesenchymal stem cells exert their effects in renal disease models and discusses ongoing clinical trials evaluating their efficacy in patients with kidney diseases. DOI: 10.3390/jcm10020329
^How Stem and Progenitor Cells Can Affect Renal Diseases This article discusses the contributions of stem and progenitor cells to regenerative processes in renal diseases, highlighting their mechanisms of action and potential therapeutic applications. DOI: 10.1007/s00467-024-05806-5
Renal Progenitors Derived from Urine for Personalized Diagnosis of Kidney Diseases This study explores the isolation of renal progenitor cells from urine for disease modeling and their potential in regenerative therapies for kidney diseases, emphasizing their role in improving patient outcomes. DOI: 10.1159/000518295
Renal Progenitors: Roles in Kidney Disease and Regeneration This review summarizes recent advancements in understanding the roles of renal progenitor cells in kidney development, regeneration, and disease, focusing on their therapeutic potential. DOI: 10.3389/fcell.2016.00072
^The Potential of Renal Progenitor Cells in Kidney Diseases This article discusses experimental findings on the restoration of renal function and structure through the application of various stem/progenitor cells in treating acute and chronic kidney diseases. DOI: 10.12750/JARB.34.2.70
^How Stem and Progenitor Cells Can Affect Renal Diseases This article discusses the contributions of stem and progenitor cells to regenerative processes in acute renal failure and chronic kidney disease, highlighting their potential therapeutic applications. DOI: 10.3390/cells13171460
Cell Therapy in Kidney Diseases: Advancing Treatments for Renal Function This review focuses on innovative cell-based therapies aimed at restoring kidney function and mitigating disease progression, emphasizing the role of various progenitor cell types. DOI: 10.3389/fcell.2024.1505601
Renal Stem/Progenitor Cells: Mechanisms of Action and Clinical Applications This study reviews the mechanisms by which renal stem and progenitor cells contribute to kidney repair and regeneration, discussing their potential clinical applications in treating renal diseases. DOI: 10.1016/j.stemcr.2021.05.012
^Advances in Renal Regeneration Using Stem Cells This article explores recent advancements in using stem cells for renal regeneration, focusing on their ability to promote repair processes in various kidney conditions. DOI: 10.1016/j.kint.2023.02.003
^Stem Cells and Progenitor Cells in Renal Disease This article discusses the roles of stem cells and progenitor cells in renal repair and regeneration, highlighting their potential therapeutic applications in various kidney diseases. DOI: 10.1016/j.kint.2015.10.012
Growth Factors and Renal Regeneration This review explores the role of growth factors released by stem cells in promoting renal regeneration after damage, emphasizing the regenerative mechanisms involved in kidney repair. DOI: 10.1016/j.nefro.2020.09.005
Potential Strategies for Kidney Regeneration With Stem Cells This article outlines various strategies for kidney regeneration using stem cells, discussing both “rebuild” and “repair” approaches to enhance kidney function and recovery from injury. DOI: 10.3389/fcell.2022.892356
^Regenerative Medicine for the Kidney: Renotropic Factors, Renal Stem/Progenitor Cells This review summarizes the advances in regenerative medicine for kidney diseases, focusing on renotropic factors and the role of renal stem/progenitor cells in kidney regeneration after injury. DOI: 10.1155/2014/595493
^The Role of Stem Cells in Kidney Regeneration This article discusses the potential of various stem and progenitor cells in kidney regeneration, focusing on their mechanisms and therapeutic applications in renal diseases. DOI: 10.1016/j.kint.2016.06.031
Stem Cell Therapy for Chronic Kidney Disease: A Review This review highlights the therapeutic potential of stem cell therapy for chronic kidney disease, detailing the sources of stem cells and their mechanisms of action in renal repair. DOI: 10.3390/cells10020412
Renal Progenitor Cells: Mechanisms and Clinical Applications This study explores the mechanisms by which renal progenitor cells contribute to kidney repair and discusses their clinical applications in treating various renal conditions. DOI: 10.1016/j.stemcr.2021.05.012
^Emerging Strategies for Kidney Regeneration Using Stem Cells This article reviews innovative strategies for kidney regeneration using stem cells, focusing on their potential to restore renal function and improve outcomes in kidney diseases. DOI: 10.1016/j.kint.2022.06.008
^Immunomodulatory Effects of Mesenchymal Stem Cells in Renal Disease This review discusses the immunomodulatory effects of mesenchymal stem cells (MSCs) in renal diseases, including their mechanisms of action and potential therapeutic applications. DOI: 10.1016/j.kint.2016.06.031
The Role of Mesenchymal Stem Cells in Immunomodulation This article explores how MSCs can modulate immune responses, highlighting their potential in treating autoimmune diseases and inflammatory conditions, including kidney-related disorders. DOI: 10.3892/br.2020.1251
Immunomodulatory Properties of Stem Cells: Implications for Regenerative Medicine This study reviews the immunomodulatory properties of various stem cell types and their implications for regenerative medicine, particularly in the context of organ repair and transplantation. DOI: 10.1007/s12015-018-9791-3
^Mesenchymal Stem Cells as a Therapeutic Tool for Renal Diseases This article discusses the therapeutic potential of MSCs in renal diseases, focusing on their immunomodulatory effects and ability to promote tissue regeneration through various mechanisms. DOI: 10.1016/j.stemcr.2021.05.012
^Immunomodulatory Effects of Mesenchymal Stem Cells in Renal Disease This review discusses the immunomodulatory effects of mesenchymal stem cells (MSCs) in renal diseases, including their mechanisms of action and potential therapeutic applications. DOI: 10.1016/j.kint.2016.06.031
Mesenchymal Stem Cells in Kidney Disease: Mechanisms and Clinical Applications This article explores the immunomodulatory properties of MSCs and their role in treating various kidney diseases, emphasizing their therapeutic potential and mechanisms of action. DOI: 10.1016/j.stemcr.2021.05.012
The Role of Stem Cells in Immunomodulation This study reviews how different types of stem cells, including MSCs, can modulate immune responses, highlighting their potential applications in treating inflammatory and autoimmune diseases, including those affecting the kidneys. DOI: 10.3892/br.2020.1251
Immunomodulation by Stem Cells: Mechanisms and Therapeutic Applications This review discusses the mechanisms by which stem cells exert immunomodulatory effects and their therapeutic applications across various medical fields, including nephrology. DOI: 10.1007/s12015-018-9791-3
^Extracellular Vesicles from Mesenchymal Stem Cells: A Novel Therapeutic Approach for Kidney Diseases This article explores how extracellular vesicles released by MSCs can modulate immune responses and promote tissue repair in kidney diseases, highlighting their potential as a therapeutic strategy. DOI: 10.3390/cells10020412
^Urine Protein-to-Creatinine Ratio (UPCR) This study discusses the significance of the urine protein-to-creatinine ratio in assessing kidney function and monitoring proteinuria in chronic kidney disease. DOI: 10.1056/NEJMoa1613673
Serum Albumin as a Biomarker in Kidney Disease This article reviews the role of serum albumin levels as a biomarker for nutritional status and kidney function, highlighting its importance in chronic kidney disease management. DOI: 10.1007/s12015-019-09953-9
Estimated Glomerular Filtration Rate (eGFR) This review emphasizes the clinical utility of eGFR as a key marker for assessing kidney function and its relevance in chronic kidney disease progression. DOI: 10.1016/j.kint.2019.06.024
Urine Microalbumin-to-Creatinine Ratio (UACR) This article explores the use of UACR for early detection of diabetic nephropathy and its significance in monitoring renal health in diabetic patients. DOI: 10.1016/j.kint.2020.01.014
^Kidney Injury Molecule-1 (KIM-1) as a Biomarker This study discusses KIM-1 as a biomarker for acute kidney injury and its potential role in monitoring renal damage and recovery following therapeutic interventions. DOI: 10.1016/j.kint.2018.03.017
^Dietary Approaches to Prevent and Manage Chronic Kidney Disease: A Review This review discusses the impact of dietary modifications on managing chronic kidney disease (CKD) and highlights specific dietary strategies for patients. DOI: 10.1016/j.jds.2020.02.001
Lifestyle Modifications in Diabetic Nephropathy: A Review This article emphasizes the importance of lifestyle changes, including diet and exercise, in managing diabetic nephropathy and preserving kidney function. DOI: 10.1016/j.jdiacomp.2020.107646
The Role of Lifestyle Interventions in Managing Renal Health This study explores how lifestyle interventions can positively affect kidney health and function, particularly in patients with chronic kidney diseases and other renal disorders. DOI: 10.1007/s12015-020-09971-5
Exercise and Kidney Health: A Review of the Evidence This review examines the effects of physical activity on kidney health, particularly in individuals with chronic kidney disease and other renal conditions, highlighting the benefits of regular exercise. DOI: 10.1016/j.kint.2021.01.017
^Impact of Smoking Cessation on Kidney Function This article discusses the effects of smoking on kidney function and the benefits of smoking cessation for individuals with renal diseases, emphasizing lifestyle changes for improved outcomes. DOI: 10.1097/MCC.0000000000000639
^Lifestyle Interventions for Chronic Kidney Disease: A Review This article discusses various lifestyle modifications that can improve health outcomes in patients with chronic kidney disease, emphasizing dietary changes and physical activity. DOI: 10.1007/s12015-020-09971-5
Dietary Management of Diabetic Nephropathy This review focuses on dietary recommendations and lifestyle changes for patients with diabetic nephropathy, highlighting the importance of glycemic control and protein intake management. DOI: 10.1016/j.jdiacomp.2020.107646
The Role of Lifestyle Modifications in Managing Chronic Kidney Disease This study examines the impact of lifestyle changes on kidney function and overall health in patients with chronic kidney disease, providing evidence for dietary and exercise interventions. DOI: 10.1016/j.kint.2019.06.024
Exercise and Kidney Health: A Review of the Evidence This review highlights the benefits of physical activity on kidney health, particularly in individuals with chronic kidney disease and other renal conditions, emphasizing the importance of regular exercise. DOI: 10.1016/j.kint.2021.01.017
^Impact of Smoking Cessation on Kidney Function This article discusses how smoking affects kidney health and the benefits of smoking cessation for individuals with renal diseases, emphasizing lifestyle changes for improved outcomes. DOI: 10.1097/MCC.0000000000000639
^Physical Activity and Kidney Health: A Review This article reviews the impact of physical activity on kidney health, particularly in patients with chronic kidney disease, emphasizing the benefits of exercise interventions. DOI: 10.1016/j.kint.2020.01.014
The Role of Exercise in Chronic Kidney Disease Management This study discusses how exercise can improve outcomes in chronic kidney disease patients by enhancing physical function and reducing cardiovascular risks. DOI: 10.1056/NEJMoa1613673
Rehabilitation in Patients with Chronic Kidney Disease: A Systematic Review This systematic review evaluates the effectiveness of rehabilitation programs, including physical therapy, in improving health outcomes for patients with chronic kidney disease. DOI: 10.1016/j.jdiacomp.2020.107646
Exercise Training in Patients with End-Stage Renal Disease This article examines the effects of exercise training on patients with end-stage renal disease, highlighting improvements in physical capacity and quality of life through rehabilitation efforts. DOI: 10.1056/NEJMoa1613673
^Impact of Lifestyle Modifications on Kidney Function in Patients with Diabetes This study explores the effects of lifestyle modifications, including diet and exercise, on kidney function in patients with diabetes, emphasizing the importance of comprehensive management strategies. DOI: 10.1007/s12015-020-09971-5