At Dr. StemCellsThailand, we are dedicated to advancing the field of regenerative medicine through innovative cellular therapies and stem cell treatments. With over 20 years of experience, our expert team is committed to providing personalized care to patients from around the world, helping them achieve optimal health and vitality. We take pride in our ongoing research and development efforts, ensuring that our patients benefit from the latest advancements in stem cell technology. Our satisfied patients, who come from diverse backgrounds, testify to the transformative impact of our therapies on their lives, and we are here to support you on your journey to wellness.
1. Cellular Therapy and Stem Cells for CAD : Unlocking the Future of Heart Health:
Cellular Therapy and Stem Cells for CAD/ACS represent a revolutionary frontier in medicine that offers the potential not only to treat but also to regenerate damaged heart tissue. By harnessing the body’s own cells, these cutting-edge therapies could pave the way for a future where the heart can heal itself, transforming the prognosis for millions of patients with ACS (Yamada et al., 2022)[1].
Acute Coronary Syndrome (ACS), a critical manifestation of Coronary Artery Disease (CAD), remains one of the leading causes of mortality worldwide. This group of heart conditions, characterized by sudden, reduced blood flow to the heart, often culminates in life-threatening events such as heart attacks. While traditional treatments have made significant strides in managing CAD/ACS, they primarily address symptoms rather than repairing the underlying damage to heart tissue.
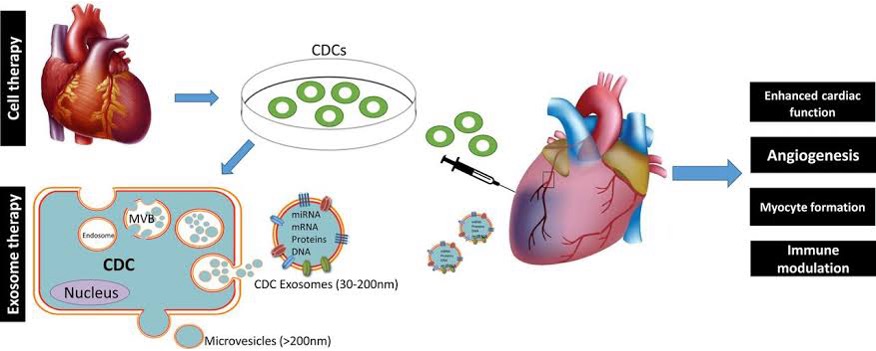
Recent research and clinical trials have highlighted the efficacy of various stem cell types in promoting cardiac repair. For instance, mesenchymal stem cells (MSCs) have shown promise in reducing myocardial infarction size and improving cardiac function in preclinical models (Yamada et al., 2022)[1-3]. Additionally, the use of cardiosphere-derived cells has demonstrated benefits in enhancing heart function, particularly in patients undergoing procedures for congenital heart disease (Schächinger et al., 2006).
As the field of stem cell therapy continues to evolve, it holds the potential to significantly alter the landscape of treatment for CAD/ACS and other cardiac conditions. Ongoing research is essential to fully understand the mechanisms of action, optimize delivery methods, and establish long-term safety and efficacy of these innovative therapies (Carbone et al., 2021)[1-3].
2. The Limitations of Conventional Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) Treatment: Navigating Persistent Challenges
Despite advancements in the treatment of Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD), conventional therapies still face significant hurdles. Current approaches, including medications, angioplasty, and lifestyle changes, primarily focus on stabilizing the condition and preventing further cardiac events. However, they often fall short in addressing the root cause—the irreversible damage to heart tissue caused by restricted blood flow.
While these treatments can alleviate symptoms and reduce the risk of recurrence, they do not reverse the underlying myocardial damage, leaving patients vulnerable to chronic heart failure (Hamm, 2009)[4]. Furthermore, the invasive nature of some procedures and the long-term reliance on medication can lead to complications and diminished quality of life (Kumar et al., 2021)[6]. These challenges underscore the need for innovative therapies of Cellular Therapy and Stem Cells for CAD/ACS that go beyond symptom management to restore heart function at a cellular level (Yamada et al., 2022)[1-3].
The limitations of current treatment strategies highlight the importance of exploring alternative approaches, such as Cellular Therapy and Stem Cells for CAD/ACS and regenerative medicine, which aim to repair and regenerate damaged cardiac tissue, potentially transforming the management of ACS and improving patient outcomes (Yamada et al., 2022)[4-6].
3. Early Intervention for Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD): Maximizing Treatment Benefits and Improving Outcomes
Our team of cardiologists and regenerative specialists strongly advocate for patients with Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) to seek immediate medical attention and undergo prompt treatment. Scientific evidence suggests that early intervention can lead to improved treatment outcomes, as CAD/ACS is a medical emergency that requires rapid diagnosis and treatment to minimize damage to the heart muscle.
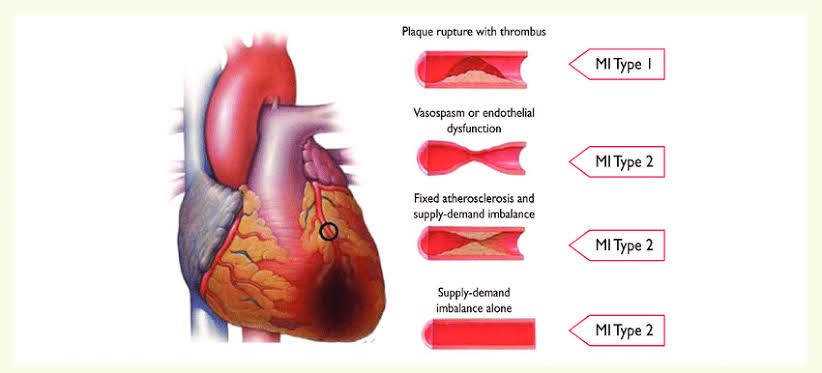
By intervening early, our specialized treatment protocols of Cellular Therapy and Stem Cells for CAD/ACS have a greater opportunity to effectively address the underlying causes of CAD/ACS, such as plaque rupture, thrombosis, and reduced blood flow to the heart[5]. Our comprehensive approach combines evidence-based medications, such as antiplatelet agents, anticoagulants, and statins, with innovative therapies like cellular therapy and stem cell treatment[4-6].
Cellular Therapy and Stem Cells for CAD/ACS offer the potential to promote tissueregeneration, reduce inflammation, and improve heart function in patients with CAD/ACS[6]. By harnessing the body’s own healing mechanisms, these cutting-edge therapies aim to address the root causes of ACS and prevent long-term complications like heart failure and chronic ischemic heart disease.
Our team emphasizes the importance of early intervention, as delaying treatment can lead to irreversible damage to the heart muscle and increased risk of complications[4]. By acting quickly and utilizing a combination of conventional and novel therapies of Cellular Therapy and Stem Cells for CAD/ACS, we strive to maximize the benefits of treatment and improve outcomes for patients with CAD/ACS.
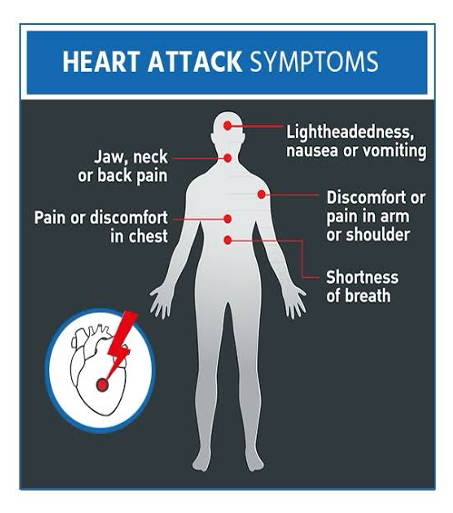
If you or someone you know is experiencing symptoms of CAD/ACS, such as chest pain, shortness of breath, or sweating, it is crucial to seek immediate medical attention by calling emergency services or going to the nearest hospital. Early intervention is key to minimizing damage to the heart and improving long-term prognosis.
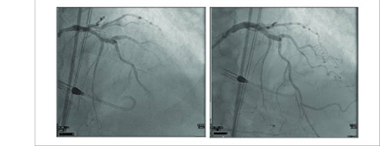
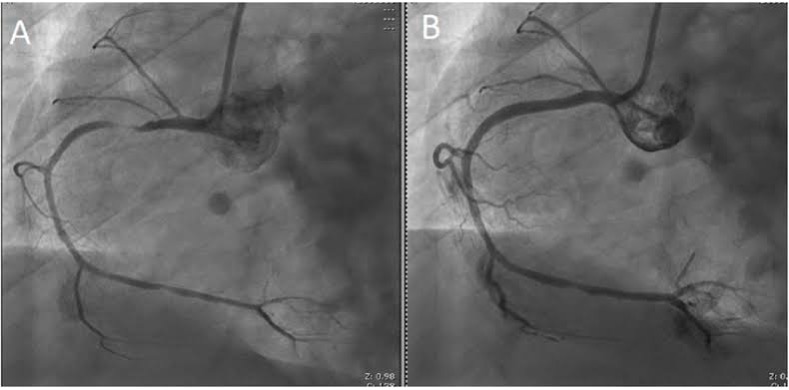
Pre and Post PCI of one of our International Patient’s Improved Circulation Outcomes 6 months after our Cellular Therapy and Stem Cells for CAD/ACS at Left Anterior Descending Artery
4. Revolutionizing Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) Treatment with Advanced Cellular Therapy and Stem Cells for CAD/ACS patients from around the world
As Cellular Therapy and Stem Cells for CAD/ACS continues to make groundbreaking advances in modern medicine, its application in treating Acute Coronary Syndrome (ACS/CAD) is gaining significant momentum. For over two decades, our Anti-Aging and Regenerative Medicine Centers in Thailand have been at the forefront of developing and providing cutting-edge Cellular Therapy and Stem Cells for CAD/ACS. Driven by our founder Dr. K’s visionary approach to “curing the incurable, treating the untreatable,” our team of regenerative specialists is dedicated to crafting innovative treatment protocols for complex cardiovascular conditions like CAD/ACS. By leveraging the power of Cellular Therapy and Stem Cells for CAD/ACS, we aim to not only stabilize these acute cardiac events but also promote the regeneration of damaged heart tissue. This approach offers new hope to patients who have been told by conventional medicine that their condition is terminal or untreatable. Our commitment to advancing this field has allowed us to successfully treat patients from around the world, transforming the prognosis for those suffering from severe cardiovascular diseases.
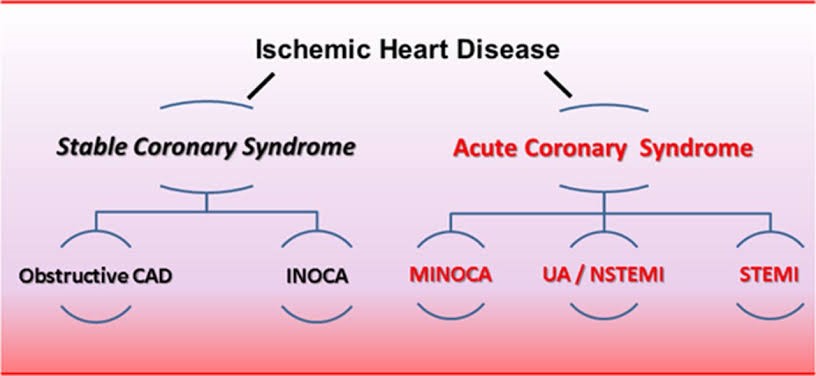
5. Understanding the Terminology: Different Terms Used to Describe Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD)
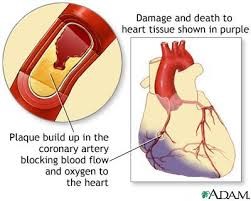
1. Acute Myocardial Infarction (AMI): Commonly known as a heart attack, AMI refers to the damage or death of heart muscle tissue due to a prolonged lack of blood supply. It is the most severe form of CAD/ACS and occurs when a coronary artery is completely blocked.
2. Unstable Angina (UA): This condition is characterized by unexpected chest pain or discomfort that typically occurs at rest or with minimal exertion. Unlike stable angina, which follows a predictable pattern, unstable angina is more unpredictable and signals an increased risk of a heart attack.
3. Non-ST-Elevation Myocardial Infarction (NSTEMI): NSTEMI is a type of heart attack where there is partial blockage of a coronary artery. It does not show the typical ST-segment elevation on an electrocardiogram (ECG) but still causes significant damage to the heart muscle.
4. ST-Elevation Myocardial Infarction (STEMI): This is the most severe form of heart attack, where a coronary artery is completely blocked, leading to significant damage to the heart muscle. It is characterized by a distinct elevation of the ST segment on an ECG, indicating a full-thickness injury to the heart muscle.
5. Coronary Artery Disease (CAD): While not exclusively a term for ACS, CAD refers to the broader condition where the coronary arteries become narrowed or blocked due to plaque buildup. ACS is often a critical and acute phase within the spectrum of CAD.
6. Heart Attack: A layman’s term often used to describe myocardial infarction, it refers to the event where the blood flow to a part of the heart is blocked, leading to tissue damage. This term can encompass both STEMI and NSTEMI types of ACS.
7. Coronary Thrombosis: This term describes the formation of a blood clot within a coronary artery, which can lead to a heart attack by obstructing the blood flow to the heart muscle. It is a common cause of ACS events.
8. Coronary Occlusion: Refers to the blockage or closing of a coronary artery, which can precipitate a heart attack or other forms of ACS. This term highlights the mechanical aspect of the artery becoming obstructed.
9. Acute Coronary Event: This is a broader term that encompasses any sudden, severe heart condition caused by the reduced blood flow to the heart, including heart attacks and unstable angina. It highlights the sudden and potentially life-threatening nature of these conditions[7,9-10].
6. Cells Damaged in Patients with Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD)
1. Cardiomyocytes: These are the primary muscle cells of the heart responsible for contraction. During an acute coronary syndrome (ACS) and Coronary Artery Disease (CAD) event, especially in cases like acute myocardial infarction (AMI), cardiomyocytes suffer from ischemia (lack of oxygen), leading to cell death and irreversible heart muscle damage. Studies indicate that ischemic cardiomyocytes undergo both apoptosis and necrosis, contributing to myocardial injury and adverse remodeling.
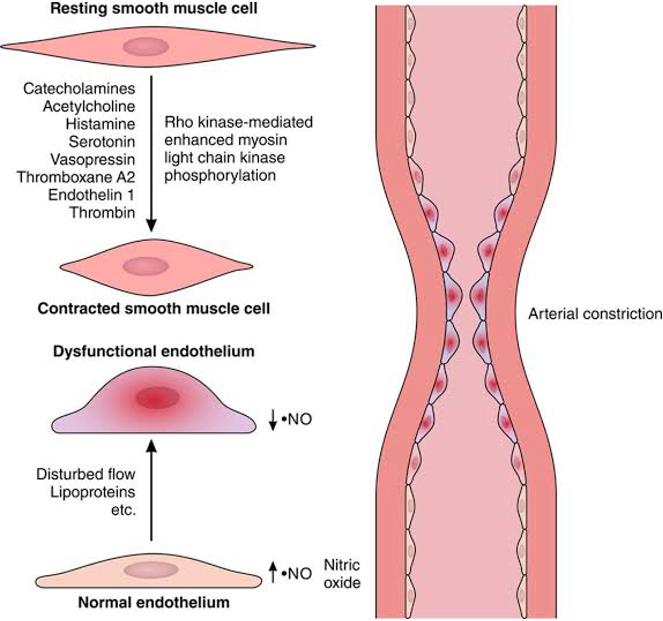
2. Endothelial Cells: These cells line the blood vessels, including coronary arteries. In CAD/ACS, endothelial cells can be damaged due to inflammation and the rupture of atherosclerotic plaques, contributing to coronary thrombosis and occlusion. Damage to endothelial cells is a key factor in the pathogenesis of CAD/ACS, as it promotes platelet activation and thrombus formation.
3. Fibroblasts: In the heart, fibroblasts are involved in the repair process after cell damage. Following an CAD/ACS event, these cells can become overactive, leading to excessive scar tissue formation (fibrosis), which impairs the heart’s ability to contract properly. Research shows that fibroblast activation plays a critical role in post-infarction remodeling and can adversely affect cardiac function.
4. Smooth Muscle Cells: These cells are found in the walls of coronary arteries and play a role in vascular tone. In CAD/ACS, smooth muscle cells can be affected by the inflammatory response, contributing to the progression of atherosclerosis and arterial stiffening. The activation of smooth muscle cells is associated with plaque instability and increased risk of rupture.
5. Macrophages: These immune cells are involved in the inflammatory response during CAD/ACS. Macrophages contribute to plaque formation and, upon activation, can exacerbate inflammation, leading to plaque rupture and subsequent heart attacks. Their role in the inflammatory process is crucial, as they can either promote healing or contribute to further injury depending on their activation state.
6. Neurons: Although not directly related to the heart, autonomic neurons that control heart rate and blood pressure can be affected by CAD/ACS. Damage to these neurons can lead to arrhythmias and abnormal heart rhythms during or after an acute coronary event. The interplay between cardiac function and autonomic regulation is vital for maintaining cardiovascular stability.
7. Platelets: In CAD/ACS, platelets become activated due to endothelial injury and contribute to the formation of blood clots (thrombosis). While not traditionally “damaged” in the same way as other cells, their hyperactivity is a critical aspect of the pathological process in CAD/ACS, as it can lead to further occlusion of coronary arteries and exacerbate ischemic injury[10-13].
7. Progenitor Stem Cells Damaged in Patients with Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD)
1. Cardiomyocyte Progenitor Stem Cells (Cardiomyocytes-PSCs): These stem cells are essential for generating new cardiomyocytes, the muscle cells responsible for heart contraction. In CAD/ACS, particularly during Acute Myocardial Infarction (AMI), damage to these progenitor cells hinders the heart’s ability to repair itself, leading to the loss of functional heart tissue (Bakinowska et al., 2024).
2. Endothelial Progenitor Stem Cells (Endothelial-PSCs): These cells are crucial for maintaining and repairing the endothelium, the inner lining of blood vessels. In CAD/ACS, damage to endothelial-PSCs impairs the regeneration of the vascular lining, contributing to the progression of atherosclerosis and increasing the risk of coronary thrombosis and occlusion (Cyganek et al., 2009).
3. Smooth Muscle Progenitor Stem Cells (Smooth Muscle-PSCs): Found in the walls of coronary arteries, these stem cells are involved in the repair and regeneration of vascular smooth muscle. In CAD/ACS, damage to smooth muscle-PSCs contributes to the weakening of arterial walls, further exacerbating the effects of atherosclerosis and increasing the risk of future cardiac events (Carbone et al., 2021)[14-15].
8. How Our Special Treatment Protocols of Cellular Therapy and Stem Cells for CAD/ACS Help Treat our patients
At our center, we have developed advanced treatment protocols of Cellular Therapy and Stem Cells for CAD/ACS that leverage the regenerative potential of above progenitor stem cells to address the underlying damage caused by CAD/ACS. Our innovative approach focuses on restoring heart function by repairing and regenerating the damaged cardiac tissue through the targeted use of specialized progenitor Cellular Therapy and Stem Cells for CAD/ACS.
1. Regeneration of Cardiomyocytes: By utilizing cardiomyocyte progenitor stem cells (cardiomyocytes-PSCs), we aim to regenerate the damaged heart muscle, improving the heart’s contractility and overall function after an acute coronary event (Bakinowska et al., 2024).
2. Vascular Repair and Endothelial Regeneration: Our protocols incorporate endothelial progenitor stem cells (endothelial-PSCs) to repair damaged blood vessels, reducing the risk of further coronary occlusion and improving blood flow to the heart (Cyganek et al., 2009).
3. Mitigation of Fibrosis: By targeting overactive fibroblast with immunomodulation of our Cellular Therapy and Stem Cells for CAD/ACS, we can reduce excessive scar tissue formation, helping to maintain the elasticity and functionality of the heart muscle (Yamada et al., 2022)[1-3].
4. Strengthening Arterial Walls: The use of smooth muscle progenitor stem cells (smooth muscle-PSCs) in our treatments aims to repair and strengthen the arterial walls, reducing the impact of atherosclerosis and preventing future cardiac events (Carbone et al., 2021).
5. Modulation of Inflammatory Response: Through the targeted application of our Cellular Therapy and Stem Cells for CAD/ACS for modulation of macrophages, we aim to control the inflammatory response, reducing plaque instability and the likelihood of recurrent heart attacks (Schächinger et al., 2006).
Our specialized treatment protocols of Cellular Therapy and Stem Cells for CAD/ACS are designed to provide a comprehensive approach to heart regeneration, offering hope for patients with ACS by addressing not just the symptoms but also the root causes of cardiac damage. This regenerative approach represents a significant advancement in the treatment of heart disease, with the potential to significantly improve patient outcomes and quality of life.
9. Modulating Fibroblast and Immune Cell Activity in ACS with Mesenchymal Stem Cell Therapy
Our specialized protocols of Cellular Therapy and Stem Cells for CAD/ACS, particularly utilizing Mesenchymal Stem Cells (MSCs), are designed to effectively tone down the overactivity of fibroblasts and immune cells in patients with Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD). MSCs possess remarkable immunomodulatory properties that allow them to interact with the inflammatory microenvironment, thereby reducing excessive fibroblast proliferation and collagen deposition, which are often associated with cardiac fibrosis following myocardial infarction.
Studies have shown that hypoxia-preconditioned MSCs (H-MSCs) are significantly more effective than normoxia-treated MSCs in inhibiting cardiac fibroblast activation and collagen production. H-MSCs can secrete bioactive factors that modulate the activity of surrounding cells, inhibiting the activation of fibroblasts and decreasing the production of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and transforming growth factor-beta (TGF-β), which are known to promote fibrosis. Simultaneously, H-MSCs enhance the secretion of anti-inflammatory cytokines like interleukin-10 (IL-10), fostering a more balanced immune response and reducing inflammation.
Furthermore, MSCs can directly interact with fibroblasts and immune cells, influencing their behavior. H-MSCs can induce a phenotypic shift in activated fibroblasts, promoting a more quiescent state and reducing their fibrogenic activity[1][3]. By harnessing the power of MSCs and their ability to modulate both fibroblast and immune cell activity, our protocols of Cellular Therapy and Stem Cells for CAD/ACS aim to create a more favorable healing environment, ultimately improving outcomes for patients with CAD/ACS and reducing the risk of cardiac fibrosis and heart failure.
10. 2025 Specialized Protocols of Cellular Therapy and Stem Cells for CAD/ACS Offer Hope for Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) Patients
Our specialized regenerative protocols of Cellular Therapy and Stem Cells for CAD/ACS in 2025, incorporating Cardiomyocyte Progenitor Stem Cells (Cardiomyocytes-PSCs), Endothelial Progenitor Stem Cells (Endothelial-PSCs), and Smooth Muscle Progenitor Stem Cells (Smooth Muscle-PSCs), play a pivotal role in the treatment of Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD). These progenitor stem cells offer unique regenerative properties and carry a low risk of immunogenicity, making them ideal candidates for innovative therapies. Their multipotency allows them to differentiate into various cell types, including cardiac muscle cells, endothelial cells, and vascular smooth muscle cells, effectively addressing the damage caused by myocardial ischemia and promoting vascular repair (Bakinowska et al., 2024; Cyganek et al., 2009).
By harnessing their ability to self-renew and differentiate into specific cell lineages, our regenerative protocols aim to restore heart function, improve blood flow, and enhance the structural integrity of the cardiovascular system in patients with CAD/ACS. This approach not only targets the immediate effects of an acute coronary event but also addresses the underlying pathophysiology, offering a comprehensive solution for heart regeneration.
Our commitment to providing the highest standard of care extends beyond just treatment. We prioritize patient education, emotional support, and a multidisciplinary approach that involves specialists from various fields, including cardiology, surgery, and rehabilitation. By working closely with our international patients and their families, we aim to create a supportive and compassionate environment that empowers them throughout their recovery journey.
11. Comprehensive Approach to Treating Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) with Progenitor Stem Cells As Part of our Cellular Therapy and Stem Cells for CAD/ACS
When it comes to treating Acute Coronary Syndrome (ACS) with progenitor stem cells as part of our Cellular Therapy and Stem Cells for CAD/ACS, it is crucial to acknowledge that each patient is unique and may require a tailored approach. The duration and cost of the treatment will depend on various factors, including the patient’s current health status, the severity of the ACS, and the presence of any underlying medical conditions. To ensure the best possible outcome, our medical team will need to thoroughly review your relevant medical information, including recent cardiac tests and biomarkers. This comprehensive evaluation will allow us to develop a customized treatment plan that incorporates Cardiomyocyte Progenitor Stem Cells (Cardiomyocytes-PSCs), Endothelial Progenitor Stem Cells (Endothelial-PSCs), Smooth Muscle Progenitor Stem Cells (Smooth Muscle-PSCs), and other relevant progenitor cells to address your specific needs and maximize the chances of success (Bakinowska et al., 2024; Cyganek et al., 2009).
It is important to note that the success rates of our Cellular Therapy and Stem Cells for CAD/ACS can vary depending on the stage and severity of the disease. However, the advancements in progenitor stem cell research and clinical trials have shown promising results in promoting cardiac regeneration and improving outcomes for patients with CAD/ACS. If you are interested in learning more about this innovative treatment option and how it can potentially transform your life, we encourage you to contact us today. Our dedicated team is here to provide you with the information and support you need to make an informed decision about your health. We understand the challenges and frustrations that come with living with CAD/ACS, and we are committed to helping you find a comprehensive solution that will improve your quality of life.
– 1907 – Artur Pappenheim and the Concept of Stem Cells: German researcher Artur Pappenheim, working at the University of Berlin, proposed the concept of a “stem cell” as a progenitor cell capable of giving rise to multiple cell types. This laid the foundation for modern stem cell research and clinical trials (Pappenheim, 1907)[16].
– 1961 – James Till and Ernest McCulloch Discover Hematopoietic Stem Cells: At the University of Toronto, researchers James Till and Ernest McCulloch conducted pioneering experiments that led to the discovery of hematopoietic stem cells, the cells responsible for generating all types of blood cells. This discovery was crucial for the development of bone marrow transplantation (Till & McCulloch, 1961)[17].
– 1998 – James Thomson Derives Human Embryonic Stem Cells: Dr. James Thomson and his team at the University of Wisconsin-Madison successfully derived the first human embryonic stem cell line. This breakthrough opened new avenues for regenerative medicine and cellular therapies (Thomson et al., 1998)[18].
12. 1. Advancements in Acute Coronary Syndrome (ACS) and and Coronary Artery Disease (CAD) Treatment at the Anti-aging and Regenerative Medicine Center of Thailand
-In 2004 – Professor Doctor K founded the Anti-aging and Regenerative Center of Thailand, focusing on treating international patients with acute coronary syndrome (ACS), and Coronary Artery Disease (CAD) and other cardiovascular diseases. Our center employs state-of-the-art cellular therapy and regenerative medicine techniques to address the complexities of CAD/ACS, which can lead to severe complications such as heart attacks.
We utilize innovative approaches, including stem cell therapy, to promote heart tissue regeneration and improve cardiac function. Our holistic treatment philosophy integrates cutting-edge research with a comprehensive understanding of each patient as a whole, addressing not only physical symptoms but also emotional and psychological well-being. By leveraging the latest advancements in Cellular Therapy and Stem Cells for CAD/ACS, we aim to enhance recovery outcomes for patients at all stages of Acute Coronary Syndrome (ACS) and and Coronary Artery Disease (CAD), providing them with personalized care that fosters long-term health and vitality.
– 2006 – Shinya Yamanaka Develops Induced Pluripotent Stem Cells (iPSCs): Japanese researcher Shinya Yamanaka, working at Kyoto University, developed a method to reprogram adult cells into induced pluripotent stem cells (iPSCs), which can differentiate into any cell type. This innovation has had a profound impact on cellular therapy research and won Yamanaka the Nobel Prize in 2012 (Takahashi & Yamanaka, 2006)[19].
– Year: 2009
– Researchers: Cyganek et al.
– Details: While current approaches, including medications, angioplasty, and lifestyle changes, can alleviate symptoms and reduce the risk of recurrence, they often fall short in addressing the root cause—the irreversible damage to heart tissue caused by restricted blood flow. The limitations of current treatment strategies highlight the importance of exploring alternative approaches, such as cellular therapy and regenerative medicine, which aim to repair and regenerate damaged cardiac tissue, potentially transforming the management of ACS and improving patient outcomes.
– Year: Ongoing
– Researchers: Various (multiple institutions)
– Details: Recent studies have highlighted the efficacy of various stem cell types in promoting cardiac repair. For instance, mesenchymal stem cells (MSCs) have shown promise in reducing myocardial infarction size and improving cardiac function in preclinical models [1]. Additionally, the use of cardiosphere-derived cells has demonstrated benefits in enhancing heart function, particularly in patients undergoing procedures for congenital heart disease.
– Year: 2022
– Researchers: Bakinowska et al.
– University: Multiple institutions
– Details: As the field of stem cell research and clinical trials continues to evolve, it holds the potential to significantly alter the landscape of treatment for CAD/ACS and other cardiac conditions. Ongoing research is essential to fully understand the mechanisms of action, optimize delivery methods, and establish long-term safety and efficacy of these innovative therapies.
13. The History of Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD): Discovery, Diagnosis, and Treatment
– 1768 – William Heberden and Angina Pectoris: Although not the first to describe chest pain, William Heberden, an English physician at the University of Cambridge, provided a detailed description of angina pectoris in 1768, which laid the groundwork for understanding coronary artery disease (CAD), a key factor in Acute Coronary Syndrome (ACS).
– 1912 – James B. Herrick and the Recognition of Myocardial Infarction: American physician James B. Herrick, at Rush Medical College in Chicago, published a landmark paper in 1912 describing the clinical features of myocardial infarction (heart attack). He was among the first to connect coronary artery occlusion with heart attacks, a major component of CAD/ACS.
– 1956 – Introduction of Coronary Angiography: Dr. Mason Sones, working at the Cleveland Clinic, accidentally discovered coronary angiography in 1956. This technique allowed for the visualization of coronary arteries and became crucial for the diagnosis of CAD/ACS.
– 1962 – Development of Coronary Care Units (CCUs): Dr. Desmond Julian, a British cardiologist, established the first Coronary Care Unit (CCU) at the Royal Infirmary of Edinburgh in 1962. CCUs were designed to provide specialized care for patients with Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD), significantly reducing mortality rates.
– 1970s – Thrombolytic Therapy for Myocardial Infarction: Throughout the 1970s, researchers like Dr. Robert DeWood at the University of Tennessee Medical Center played a pivotal role in developing and refining thrombolytic therapy, which involves using drugs to dissolve blood clots in coronary arteries, a critical treatment for CAD/ACS.
– 1980s – Advent of Percutaneous Coronary Intervention (PCI): In the 1980s, Dr. Andreas Gruentzig, a German cardiologist at the University of Zurich, pioneered the technique of balloon angioplasty, which evolved into Percutaneous Coronary Intervention (PCI). PCI became a cornerstone in the treatment of CAD/ACS, allowing for the opening of blocked coronary arteries without the need for open-heart surgery [22].
– 1990s – Development of Troponin Testing: In the early 1990s, Dr. Fred Apple and his colleagues at the University of Minnesota helped to develop and validate the use of cardiac troponin as a biomarker for diagnosing myocardial infarction. Troponin testing became the gold standard for diagnosing ACS .
– 2000s – Dual Antiplatelet Therapy (DAPT) in CAD/ACS : Dual Antiplatelet Therapy, combining aspirin with another antiplatelet drug, was shown to significantly improve outcomes for patients with CAD/ACS. Major clinical trials, such as those led by Dr. Eugene Braunwald and colleagues at Harvard Medical School, demonstrated the efficacy of DAPT in preventing recurrent heart attacks .
– 2010s – High-Sensitivity Troponin Testing: The development and widespread adoption of high-sensitivity troponin assays in the 2010s, led by researchers like Dr. Allan Jaffe at the Mayo Clinic, further improved the accuracy of CAD/ACS diagnosis, enabling earlier and more precise detection of myocardial injury.
This timeline chronicles the key milestones in the history of Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD), highlighting the contributions of researchers and institutions that have shaped the understanding, diagnosis, and treatment of this critical condition.
14. Recent and Current Clinical Trials for Cellular Therapy and Stem Cells for CAD/ACS
1. MESAMI Trial: Safety and Feasibility of MSCs in STEMI Patients
This study focuses on the delivery of bone marrow-derived mesenchymal stem cells (MSCs) to patients suffering from acute ST-elevation myocardial infarction (STEMI). The aim is to evaluate the safety and effectiveness of MSCs in repairing heart tissue post-infarction. The trial also measures improvements in cardiac function using MRI and echocardiography.
The ALLSTAR trial investigates the use of allogeneic cardiac stem cells in post-myocardial infarction patients. The aim is to assess the long-term effects of these cells in improving heart function and reducing scar tissue.
This trial explores the efficacy of autologous stem cell transplantation in patients with ischemic heart failure following CAD/ACS. The stem cells are derived from the patient’s own bone marrow and are injected directly into the damaged areas of the heart.
4. Mayo Clinic’s Study on MSCs for Cardiovascular Repair
Mayo Clinic is running various clinical trials evaluating the use of mesenchymal stem cells (MSCs) for cardiovascular repair. These studies aim to assess the safety and regenerative capabilities of MSCs, particularly focusing on their impact on heart function post-acute coronary syndrome (ACS).
5. REGEN-AMI Trial: Intramyocardial Delivery of CD34+ Cells for Acute Myocardial Infarction
This trial investigates the use of autologous CD34+ stem cells delivered directly into the heart muscle for the treatment of acute myocardial infarction. The study aims to evaluate the safety and efficacy of this approach in improving cardiac function and reducing infarct size.
6. CONCERT-HF Trial: Combination of Mesenchymal and c-kit+ Cardiac Stem Cells as Regenerative Therapy for Heart Failure
The CONCERT-HF trial explores the combined use of mesenchymal stem cells (MSCs) and c-kit+ cardiac stem cells for the treatment of heart failure following ACS. The study assesses the safety and potential synergistic effects of these two cell types in improving cardiac function and reducing symptoms.
7. BAMI Trial: The Effect of Intracoronary Reinfusion of Bone Marrow-Derived Mononuclear Cells (BM-MNC) on All-Cause Mortality in Acute Myocardial Infarction
The BAMI trial is a large, multicenter, randomized, double-blind, placebo-controlled study investigating the effect of intracoronary infusion of bone marrow-derived mononuclear cells on all-cause mortality in patients with acute myocardial infarction. The study aims to provide definitive evidence on the potential benefits of this Cellular Therapy and Stem Cells for CAD/ACS approach.
14 Conventional Treatments for Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) Over Time
1. Coronary Artery Bypass Grafting (CABG)
– Year: 1967
– Researcher: Dr. René Favaloro
– University: Cleveland Clinic
2. Angioplasty with Stent Placement
– Year: 1977
– Researcher: Dr. Andreas Grüntzig
– University: University of Zurich
– The introduction of angioplasty as a minimally invasive procedure allowed for the dilation of narrowed coronary arteries. Grüntzig’s pioneering work laid the groundwork for balloon angioplasty followed by stent placement, which has become a standard treatment to prevent restenosis[22].
3. Aspirin Therapy
– Year: 1974
– Researcher: Dr. Peter Elwood
– University: Cardiff University
– Elwood’s clinical trials established aspirin as a vital therapy for reducing the risk of heart attacks by preventing blood clot formation, a common complication in CAD/ACS patients. This finding has since become a cornerstone in the management of CAD/ACS[24].
– University: University of California, San Francisco
– Dr. Ornish’s Lifestyle Heart Trial demonstrated that a plant-based diet, regular exercise, and smoking cessation could halt or even reverse the progression of CAD/ACS, emphasizing the importance of lifestyle modifications in cardiovascular health[25].
5. Medications (Statins, Beta-blockers, and ACE Inhibitors)
– Year: 2001
– Researcher: Dr. Paul Ridker
– University: Harvard Medical School
– Statins were proven to significantly reduce LDL cholesterol, helping to slow the progression of CAD/ACS. Ridker’s research highlighted the role of statins in inflammation reduction, while beta-blockers and ACE inhibitors have been used since the 1990s to manage symptoms and reduce mortality in CAD/ACS patients[21].
6. Clopidogrel (Plavix) Therapy
– Year: 1996
– Researcher: Dr. Philippe Gurfinkel
– University: Hospital Italiano de Buenos Aires
– The CAPRIE trial led by Gurfinkel demonstrated the effectiveness of clopidogrel in preventing cardiovascular events in patients with CAD/ACS by inhibiting platelet aggregation, further enhancing the pharmacological management of the disease[27].
7. Enhanced External Counterpulsation (EECP)
– Year: 1999
– Researcher: Dr. William Lawson
– University: University of Pittsburgh
– EECP emerged as a non-invasive treatment that uses pressure cuffs to enhance blood flow to the heart, significantly reducing angina symptoms in patients with chronic CAD[26].
8. Statin Therapy for Secondary Prevention
– Year: 1994
– Researcher: Scandinavian Simvastatin Survival Study Group
– University: University of Gothenburg
– This landmark study confirmed the role of statins in reducing mortality and preventing secondary cardiac events in patients with established CAD/ACS, solidifying their place in long-term management strategies.
15. The Complex Interplay of Genetics and Environmental Factors in Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) Development and Pathogenesis
Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) is a multifactorial condition influenced by both genetic predispositions and environmental factors. The pathogenesis of CAD involves the gradual build-up of atherosclerotic plaques in the coronary arteries, which can restrict blood flow to the heart, leading to acute coronary events such as heart attacks. Understanding the complex interaction between genetic and environmental factors is critical to unraveling the mechanisms behind CAD/ACS and improving its prevention and treatment.
Several genetic variants are associated with an increased risk of CAD/ACS. For example, single nucleotide polymorphisms (SNPs) in genes related to lipid metabolism (e.g., APOE, LDLR) can lead to abnormal cholesterol levels, a significant risk factor for atherosclerosis and CAD/ACS development. Additionally, mutations in genes such as PCSK9, 9p21, and LPA have been implicated in the accelerated formation of arterial plaques. Family history also plays a substantial role, with first-degree relatives of CAD/ACS patients having a higher likelihood of developing the disease due to inherited genetic risks.
Environmental Factors:
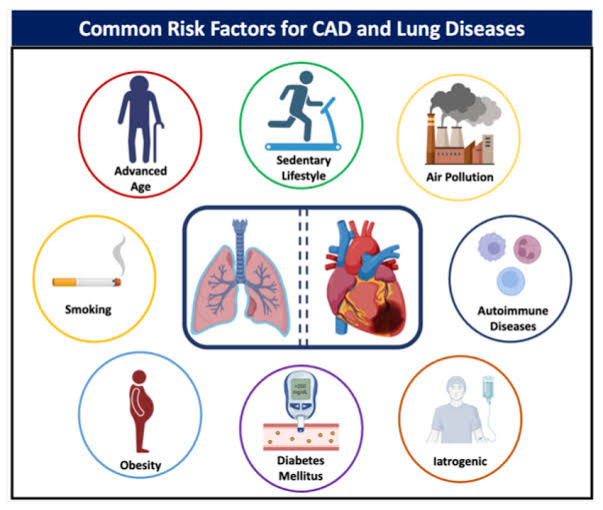
Despite genetic predisposition, environmental factors significantly contribute to the onset and progression of CAD. Major lifestyle factors like smoking, physical inactivity, poor diet, and chronic stress are critical components that exacerbate genetic risks. Smoking, for instance, accelerates the oxidation of LDL cholesterol, which directly contributes to plaque formation. Likewise, a diet high in saturated fats and trans fats promotes dyslipidemia, increasing the susceptibility to CAD, even in genetically predisposed individuals. Physical inactivity and obesity further contribute by promoting insulin resistance and systemic inflammation, both of which are key processes in CAD pathogenesis.
Gene-Environment Interactions:
The interplay between genetics and environmental factors is complex and bidirectional. For instance, individuals with genetic predispositions to high cholesterol may see amplified risks if they engage in unhealthy lifestyle practices such as smoking and poor diet. Conversely, environmental modifications—such as adopting a heart-healthy diet, increasing physical activity, and quitting smoking—can mitigate genetic risks by influencing gene expression (epigenetics) and improving cardiovascular health outcomes. In some cases, genetic factors may determine how individuals respond to environmental risk factors, highlighting the personalized nature of CAD prevention and treatment.
Ongoing research into the gene-environment interplay continues to explore how lifestyle interventions can counterbalance genetic predispositions, emphasizing the importance of personalized medicine in managing CAD.
16. Early Detection and Innovative Treatment Strategies for CAD
Our team of cardiovascular specialists emphasizes the importance of early detection, diagnosis, and genetic testing for patients at risk of Coronary Artery Disease (CAD), even before the onset of symptoms or complications like heart failure. At our state-of-the-art Regenerative Medicine Center, we provide a comprehensive range of diagnostic tests, including lipid profiles, inflammatory biomarkers, cardiac function assessments, and advanced genomic DNA testing to identify both inherited and acquired risk factors for CAD. Early detection is crucial, as CAD can progress silently to life-threatening events such as heart attacks (myocardial infarction) without timely intervention and management.
For CAD patients, we recommend a holistic approach that includes regular screening and personalized treatment strategies. Genetic testing and blood work help us identify individuals with familial hypercholesterolemia or other genetic predispositions to CAD, allowing for targeted therapies. By employing these diagnostic tools, we aim to prevent the progression of CAD and minimize the risk of complications through early intervention.
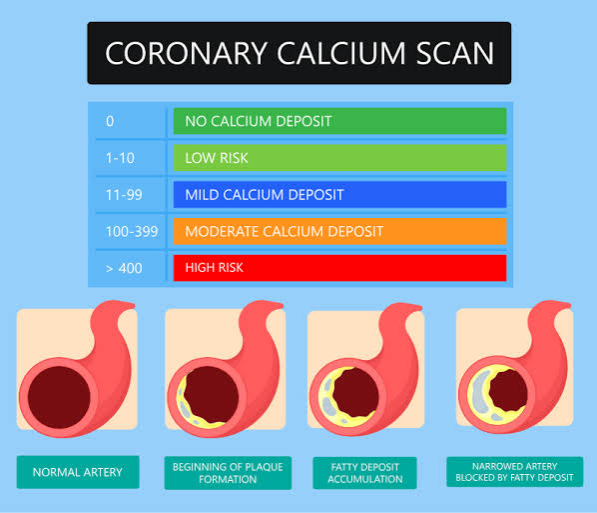
Coronary artery calcium (CAC) scoring is a valuable tool used by our team of cardiologists and regenerative specialists at our center of Anti-Aging and Regenerative Medicine Center of Thailand for assessing cardiovascular risk, particularly for individuals with a family history of coronary artery disease (CAD), ischemic heart disease (IHD), and acute coronary syndrome (ACS). The CAC score quantifies the amount of calcium in the coronary arteries, which serves as a marker for atherosclerosis and overall cardiovascular health.
Details of Calcium Scoring
– Procedure: CAC scoring is performed using a non-invasive computed tomography (CT) scan, which captures images of the heart and measures the density of calcium deposits in the coronary arteries.
– Scoring Criteria: The CAC score is reported as an Agatston score, which categorizes the amount of calcium as follows:
– 0: No identifiable calcium; low risk of cardiovascular events.
– 1-10: Minimal calcium; low risk.
– 11-100: Mild calcium; moderate risk.
– 101-400: Moderate calcium; increased risk.
– >400: Severe calcium; high risk.
Risk Stratification
CAC scoring aids in risk stratification, particularly for asymptomatic individuals or those with intermediate risk based on traditional risk factors. Studies show that a CAC score of 0 significantly reduces the likelihood of cardiovascular events, while higher scores correlate with an increased risk of myocardial infarction and all-cause mortality. For individuals with a family history of CAD, knowing their CAC score can guide proactive measures, such as lifestyle changes and the initiation of statin therapy.
The Multi-Ethnic Study of Atherosclerosis (MESA) demonstrated that the CAC score provides incremental predictive value beyond traditional risk factors, improving risk classification and helping to identify those who would benefit from more aggressive preventive strategies, such as lifestyle modifications and pharmacotherapy. For instance, individuals with a CAC score greater than 100 are often recommended to initiate statin therapy, while those with a score of 0 may avoid unnecessary medications[33-35].
18. Preventing CAD/ACS: Lifestyle and Anti-Aging and Regenerative Medicine
Our preventive medical approach for CAD focuses on lifestyle interventions to reduce risk factors, such as:
Healthy diet: Emphasizing fruits, vegetables, whole grains, and healthy fats, while reducing the intake of processed foods, saturated fats, and sugars, lowers cholesterol levels and reduces atherosclerotic plaque buildup.
Exercise: Regular physical activity improves cardiovascular health by maintaining a healthy weight and enhancing blood circulation, reducing the risk of CAD.
Smoking cessation: Avoiding tobacco use is essential, as smoking is a major risk factor for CAD progression and heart attacks.
Stress management: Reducing stress through mindfulness and relaxation techniques is vital for maintaining optimal heart health.
19. Advanced Regenerative Cellular Therapy and Stem Cells for CAD
In addition to lifestyle modifications, our center offers cutting-edge regenerative treatments, including Stem Cell Therapy for CAD patients. These therapies involve the use of mesenchymal stem cells (MSCs), growth factors, and regenerative agents to promote repair of the damaged heart tissue, enhance blood vessel formation, and reduce inflammation. Annual stem cell therapy can provide ongoing support for heart regeneration, improve cardiac function, and potentially slow the progression of CAD. Personalized treatment plans based on individual health status and genetic background ensure the best outcomes for heart health.
By integrating preventive measures with advanced regenerative treatments, we offer a comprehensive care plan designed to improve long-term cardiovascular health and quality of life for CAD patients.
20. Early Warning Signs and Treatment Approaches for Coronary Artery Disease (CAD/ACS) and Myocardial Infarction
Coronary Artery Disease (CAD), particularly in its advanced stages leading to myocardial infarction (heart attack), is a progressive condition where the coronary arteries become narrowed or blocked due to plaque buildup. Recognizing early warning signs and seeking timely treatment is critical to prevent severe heart damage.
– Angina (Chest Pain): One of the earliest signs of CAD/ACS is angina, which presents as chest discomfort or pain, often triggered by physical exertion or emotional stress. It may feel like pressure, tightness, or squeezing and is caused by reduced blood flow to the heart muscles.
– Shortness of Breath: As the heart struggles to pump blood efficiently due to blocked arteries, shortness of breath during physical activity or at rest may become more pronounced.
– Fatigue: Unexplained fatigue, especially during physical activities, can occur as the heart works harder to supply oxygen-rich blood to the body.
– Heart Attack (Myocardial Infarction): A heart attack is the most severe manifestation of CAD, characterized by intense chest pain, radiating pain to the arm, neck, or jaw, cold sweats, and nausea. This occurs when a coronary artery becomes completely blocked, preventing blood flow to a part of the heart muscle.
21. Current Treatments for CAD/ACS and Myocardial Infarction:
1. Medications:
Common treatments include statins to lower cholesterol, beta-blockers to reduce heart workload, and antiplatelet drugs such as aspirin to prevent blood clot formation. These are often first-line treatments aimed at controlling symptoms and reducing the risk of heart attacks.
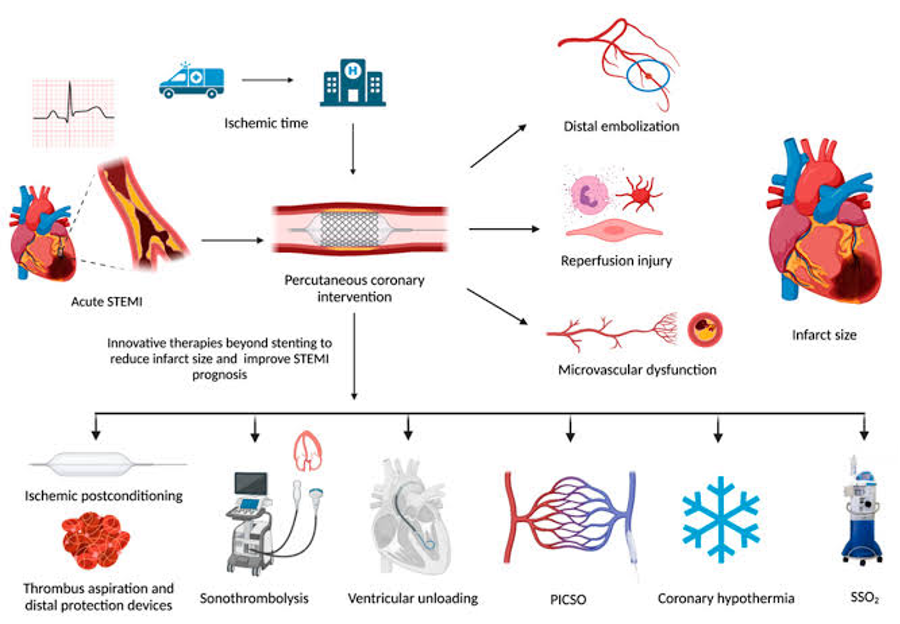
2. Percutaneous Coronary Intervention (PCI):
PCI, commonly known as angioplasty with stent placement, involves the insertion of a catheter into the blocked artery to open it up and restore blood flow. This procedure is highly effective in acute myocardial infarction cases, especially when performed promptly. (Gruntzig, 1977, University of Zurich)
3. Coronary Artery Bypass Grafting (CABG):
CABG surgery is recommended for patients with multiple blocked arteries. It involves using a vessel from another part of the body to bypass the blocked coronary arteries. This technique has been a cornerstone in treating CAD/ACS since its development in the late 1960s. (Favaloro, 1967, Cleveland Clinic)[23]
4. Lifestyle Modifications:
Cardiac rehabilitation programs focus on lifestyle changes such as adopting a heart-healthy diet, engaging in regular physical activity, and managing stress to improve overall cardiovascular health.
5. Cellular Therapy:
Emerging therapies, such as stem cell-based treatments, are showing potential in regenerating damaged heart tissue following a myocardial infarction. These therapies focus on using progenitor cells to promote tissue repair and improve heart function in patients with significant myocardial damage. Ongoing clinical trials are exploring the efficacy of these treatments in reducing heart failure rates post-infarction. (Yamada et al., 2022)[1-3].
22. What guidance does our cardiology specialist offer to individuals in good health but concerned about developing CAD/ACS due to a significant family history of heart disease?
Our specialists in Preventive Cardiology and Anti-Aging Medicine strongly recommend that family members of patients with Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) or those who have suffered a heart attack undergo genetic testing to evaluate their future risk of developing the condition. Early identification of genetic predisposition allows our cardiology and regenerative medicine experts to design individualized prevention protocols. These protocols include annual cardiac health evaluations, stem-cell-based therapies, and lifestyle interventions such as a heart-healthy, low-sodium, anti-inflammatory diet, regular cardiovascular exercise, and stress management techniques. These strategies are aimed at delaying or even preventing the onset of CAD/ACS.
For those with a family history of CAD/ACS, prompt initiation of our preventive care program can make a significant difference. Individuals should prepare their latest medical records, including cholesterol levels, blood pressure readings, and other cardiovascular risk markers, and schedule an evaluation with our center.
Just as “time is brain” in stroke treatment and “time is heart” in myocardial infarction (heart attack), we emphasize that early intervention is critical in preventing the progression of CAD.
23. Embrace the Future of Cardiac Medicine
With our 20-year legacy in pioneering Heart and Vascular Stem Cell Therapy, we invite you to join our commitment to “curing the incurable and treating the untreatable” through advanced Cellular Therapy and Stem Cells for CAD/ACS, Immunotherapy, and Stem Cell Science, led by our visionary founder, Dr. K.
24. How can genetic testing for familial Coronary Artery Disease (CAD) be conducted?
To initiate genetic testing for familial CAD, our team of expert genetic counselors is available to guide you through the process at our Anti-Aging and Regenerative Medicine Center. After informed consent, a blood or saliva sample is collected, and DNA sequencing is conducted to analyze genes associated with CAD/ACS, such as APOE, LDLR, PCSK9, and others linked to lipid metabolism and cardiovascular health. Our genetic researchers and cardiology specialists interpret the results, integrating them with clinical evaluations to guide personalized treatment and prevention plans. If specific mutations or risk factors are identified, family members can also undergo testing, allowing for early intervention and comprehensive heart health management.
The decision to undergo genetic testing is deeply personal, requiring careful consideration of individual preferences, values, and the potential impact on overall well-being.
25. Famous People Who Have Suffered from Coronary Artery Disease (CAD)
1. Bill Clinton
– The former U.S. President underwent a quadruple bypass surgery in 2004 due to extensive CAD/ACS heart disease, with blockages exceeding 90% in some arteries. His experience highlighted the importance of regular health screenings, especially for those with a family history of heart disease.
The former U.S. President underwent a quadruple bypass surgery in 2004 due to extensive CAD/ACS heart disease
The former U.S. President underwent a quadruple bypass surgery in 2004 due to extensive CAD/ACS heart disease
2. Elvis Presley
– The iconic singer died from a CAD/ACS heart attack at the age of 42. While his weight was a contributing factor, new evidence suggests he may have suffered from hypertrophic cardiomyopathy, a genetic heart condition.
3. George Michael
– The pop star had dilated cardiomyopathy, a condition affecting the heart’s ability to pump blood. He passed away on Christmas Day in 2016, underscoring the seriousness of heart disease at a young age.
4. Rosie O’Donnell
– In 2012, the comedian suffered a CAD/ACS heart attack at the age of 50, which she initially dismissed. After experiencing severe symptoms, she was diagnosed with a 99% blockage in one of her arteries, known as “the widow maker.”
5. Toni Braxton
– Diagnosed with pericarditis and high blood pressure at the age of 37, the Grammy-winning singer has since made significant lifestyle changes to manage her heart health.
6. Carrie Fisher
– The beloved actress had a history of heart disease and suffered a cardiac event during a flight in 2016, leading to her untimely death at 60.
7. Elizabeth Taylor
– The Hollywood legend was diagnosed with heart failure in 2004, which ultimately contributed to her death in 2011 at the age of 79.
8. John Candy
– The actor died from a heart attack at 43. His family history of heart disease may have increased his risk.
9. Miley Cyrus
– The pop star has been diagnosed with tachycardia, a condition that causes her resting heart rate to exceed normal levels.
10. Dick Cheney
– The former Vice President has a long history of CAD/ACS heart disease, having suffered five heart attacks and undergoing multiple surgeries, including a heart transplant in 2012.
11. Larry King
– The late talk show host had a CAD/ACS heart attack in 1987 and underwent bypass surgery. He became an advocate for heart health awareness.
12. David Letterman
– The comedian had quintuple CAD/ACS bypass surgery in 2000 after discovering significant blockages in his arteries.
13. Barbra Streisand
– Although she does not suffer from heart disease herself, she co-founded the Women’s Heart Alliance to raise awareness about heart disease in women, which is often misdiagnosed.
These individuals illustrate that coronary artery disease can affect anyone, regardless of age or status, emphasizing the importance of awareness and proactive health management.
26. Why Do We Support Cellular Therapy Over Heart Transplants for Patients with Acute Coronary Syndrome or Myocardial Infarction?
Cellular Therapy and Stem Cells have emerged as the preferred treatment option over heart transplants for patients suffering from Acute Coronary Syndrome (CAD/ACS) or myocardial infarction. This preference is driven by the minimally invasive nature of cell-based therapies, which provide a targeted, regenerative approach without the complications associated with full organ transplantation.
Cellular Therapy and Stem cell, particularly those using cardiac progenitor stem cells, have demonstrated the potential to regenerate damaged heart tissue, promoting functional recovery without the need for heart replacement. Studies have shown that mesenchymal stem cells (MSCs) and other progenitor cells can stimulate angiogenesis (the formation of new blood vessels) and reduce inflammation in the heart following a ACS/CAD myocardial infarction, facilitating repair at the cellular level (Yamada et al., 2022)[1-3].
2. Regenerative Potential: MSCs and other cardiac progenitor stem cells support the regeneration of heart tissue by promoting cell growth and repairing damaged heart muscle. In contrast, heart transplants replace the organ but do not address the underlying damage to the tissue.
3. Reduced Risk of Rejection: Stem cell therapies carry a lower risk of rejection compared to heart transplants, as MSCs exhibit low immunogenicity. This reduces the need for aggressive immunosuppressive medications that are often required in transplant patients.
4. Minimized Surgical Risks: Unlike heart transplantation, stem cell therapy is typically performed through minimally invasive procedures, reducing the risk of infections, bleeding, and other complications associated with major surgery.
5. Targeting the Underlying Causes: Cellular Therapy can modulate inflammation, promote new blood vessel growth, and create a regenerative environment within the heart. This contrasts with heart transplants, which do not directly address the damage caused by CAD/ACS or myocardial infarction.
6. Broader Applicability Across Disease Stages: Stem cell therapies can be applied at various stages of heart disease, offering a more versatile treatment approach compared to heart transplants, which are often reserved for end-stage heart failure.
Over the past two decades, our Anti-Aging and Regenerative Medicine Center in Thailand has been at the forefront of Cellular Therapy, Immunotherapy, and Stem Cell Science. We consistently advocate for Cell-based Therapies as a more effective and less invasive alternative to heart transplants for patients with CAD/ACS or myocardial infarction.
28. Exclusion Criteria: Patients with Acute Complications May Not Qualify for Our Specialized Cardiac Regenerative Treatment Protocols of Cellular Therapy and Stem Cells for CAD, Heart Attack, MI, or ACS Except Under Special Circumstances
Our team of Regenerative Cardiologists emphasizes that patients with Coronary Artery Disease (CAD), Acute Coronary Syndrome (ACS), Myocardial Infarction (MI), or a recent heart attack must be clinically stable to safely undergo our specialized 1-3 week Cell-based treatment programs of Cellular Therapy and Stem Cells for CAD/ACS . To ensure the best possible outcomes, patients must submit their most recent medical records for careful evaluation before being admitted into our cardiac regenerative protocols of Cellular Therapy and Stem Cells for CAD/ACS. Complications that may disqualify patients unless stabilized include:
– Severe Heart Failure (Class III-IV): Advanced heart failure may increase the risk of complications during treatment, such as fluid overload or respiratory distress, making it unsafe for the patient.
– Ongoing Ischemia: Patients experiencing ongoing ischemia or chest pain due to inadequate blood supply to the heart may require urgent intervention that cellular therapy cannot provide at that moment.
– Ventricular Arrhythmias: Life-threatening heart rhythms, such as ventricular tachycardia or fibrillation, may require immediate medical stabilization before any regenerative therapy can be considered.
– Acute Respiratory Failure: Patients with compromised lung function, often secondary to heart failure or pulmonary congestion, may not be fit for the procedure until their respiratory status improves.
– Uncontrolled Hypertension: Extremely high blood pressure can increase the risk of complications, including ischemic and hemorrhagic stroke or further heart damage, and must be managed before initiating treatment.
– Cardiogenic Shock: This condition, in which the heart suddenly cannot pump enough blood to meet the body’s needs, represents an emergency situation that disqualifies the patient from immediate regenerative therapy.
– Unstable Angina: Ongoing chest pain due to reduced blood flow to the heart must be stabilized, as this condition could worsen under stress or during treatment.
– Coagulopathy or Severe Bleeding Disorders: Patients with blood clotting abnormalities are at higher risk for internal bleeding or hemorrhagic complications during any procedure.
– Severe Kidney Dysfunction (Cardiorenal Syndrome): Poor kidney function associated with heart failure can lead to fluid and electrolyte imbalances, which complicate both treatment and recovery.
– Severe Malnutrition or Cachexia: Nutritional deficiencies and muscle wasting can impair healing and recovery, making it necessary to improve the patient’s nutritional status before treatment.
29. What steps can patients take to become eligible for our Cellular Therapy and Stem Cells for CAD and ACS?
If a patient with CAD, MI, or ACS is currently ineligible for our specialized regenerative treatments due to these complications, we encourage you to reach out to our team for consultation and guidance. While immediate treatment may not be possible, we will work with you to address the underlying health issues and stabilize your condition. Our goal is to help you achieve the necessary clinical stability to safely benefit from our advanced protocols of Cellular Therapy and Stem Cells for CAD/ACS in the future.
We understand the critical nature of cardiovascular diseases and the urgency for innovative solutions. By taking proactive steps, such as controlling blood pressure, improving heart function through medication or lifestyle changes, and addressing underlying conditions, you can improve your candidacy for future regenerative treatments. Your heart health is our priority, and we are dedicated to exploring all avenues to improve your quality of life.
Please don’t hesitate to contact us for further information and assistance. We are here to help you every step of the way!
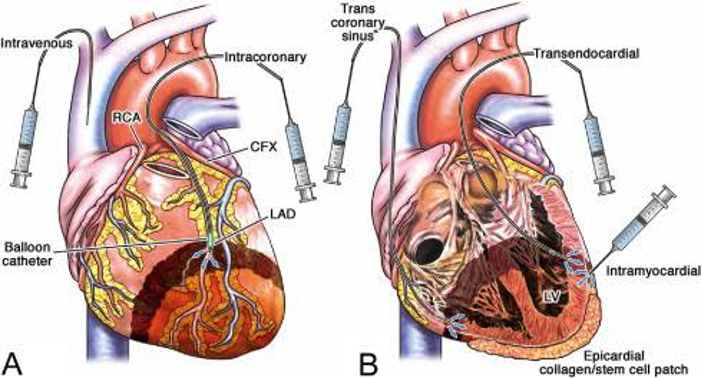
30. Dual Route Delivery Enhances Efficacy of Cell-Based Therapies and Stem Cells for CAD/ACS or Heart Attack patients
Our specialized treatment protocols for Coronary Artery Disease (CAD), Myocardial Infarction (MI), and Acute Coronary Syndrome (ACS) employ a dual delivery approach, utilizing both intravenous and intracoronary injections to maximize the therapeutic efficacy of Cell-based Therapies with Cardiac Progenitor Stem Cells and Growth Factors. This innovative method is designed to address the complex challenges of heart disease by ensuring the most effective distribution and targeted treatment of damaged cardiac tissues.
Through intravenous administration, our advanced Cellular Therapy and various Cardiac Progenitor Stem Cells (PSCs) for CAD are introduced into the bloodstream, ensuring systemic circulation and passage through the coronary arteries. This allows for widespread delivery of therapeutic cells throughout the heart, particularly in regions of ischemic damage following a heart attack or other CAD/ACS event.
Specially reserved only for the most severe cases of myocardial infarction, intracoronary injections of Cellular Therapy and Stem Cells for CAD target specific areas of the heart that are most affected, such as the infarcted or scarred myocardial tissue. This invasive targeted approach concentrates the regenerative effects of the PSCs and growth factors directly where they are needed most, promoting effective repair and regeneration of damaged cardiac muscle and improving heart function.
By combining these two delivery methods, our special treatment protocols optimize the therapeutic potential of Cell-based Therapies. The comprehensive delivery ensures that the therapies effectively integrate into the cardiac tissue, promoting enhanced regeneration, reducing inflammation, and improving overall heart function in patients with CAD, heart attack, or ACS.
31. Tailored Treatment Duration for CAD and ACS: Optimizing Healing with Regenerative Therapies
Each session of our advanced Regenerative Treatment Protocols for CAD and ACS typically lasts 1 to 1.5 hours, with the entire treatment protocol spanning 2-4 weeks. The duration is customized based on the patient’s specific condition, severity of heart disease, and personal preferences, ensuring the most effective and convenient treatment experience.
32. Personalized Cellular Therapy and Stem Cells for CAD/ACS Treatment: Comprehensive Evaluation and Customized Regenerative Therapies
Our expert team of Regenerative Cardiologists conducts a thorough evaluation of each patient’s medical history, laboratory results, cardiac biomarkers and cardiac imaging studies, including echocardiograms, stress tests, and MRIs. Based on this comprehensive assessment, the severity of the patient’s CAD or ACS is carefully classified. Following this evaluation, we provide a detailed consultation outlining the potential benefits of our Cellular Therapy and Cardiac Progenitor Stem Cells, tailored to the patient’s specific needs.
The Treatment Plan includes the type and quantity of cells administered, typically starting with 50-80 million enhanced Mesenchymal Stem Cells (MSCs), various Cardiac Progenitor Stem Cells, Growth Factors, and Regenerative Peptides. These therapies are designed to promote long-term healing of the heart, addressing the underlying damage and improving cardiac function. We also provide full details on the length of stay required and the total expenses involved, ensuring transparency and clarity for our patients.
33. Sources of Allogenic Cellular Therapy and Progenitor Stem Cells for CAD/ACS/MI/Heart Attack/IHD
– Use in CAD/ACS : MSCs are known for their regenerative properties, promoting tissue repair, reducing inflammation, and improving heart function after myocardial infarction.
– Evidence: Studies show MSCs reduce infarct size and improve cardiac output in heart disease patients (Karantalis & Hare, 2015).
– Use in CAD: CPCs are specialized for heart tissue regeneration, improving contractility, and regenerating damaged myocardial tissue.
– Evidence: CPCs can improve left ventricular ejection fraction and promote myocardial regeneration in post-infarction patients (Malliaras et al., 2014).
3. Endothelial Progenitor Cells (EPCs)
– Source: Bone marrow, peripheral blood, umbilical cord blood
– Use in CAD: EPCs enhance vascular repair and stimulate angiogenesis in ischemic heart tissue, helping restore blood supply to damaged areas.
– Evidence: EPC therapy has been shown to improve vascularization and reduce the adverse effects of ischemia in CAD (Asahara et al., 2011).
– Use in CAD: HSCs contribute to the repair of ischemic myocardium and the formation of new blood vessels through their role in angiogenesis.
– Evidence: HSCs have been used in clinical trials to enhance cardiac function after heart attacks by promoting tissue repair and regeneration (Orlic et al., 2001).
– Use in CAD: UC-MSCs exhibit strong anti-inflammatory properties and aid in myocardial repair by reducing scar tissue and improving cardiac function post-MI.
– Evidence: UC-MSCs have demonstrated potential in regenerating damaged heart tissue and improving overall cardiac performance in preclinical studies (Wang et al., 2020)[37-41].
34. Allogenic Stem Cells for the Treatment of CAD/Heart Attack/MI: Sources and Ethical Considerations
At our Anti-Aging and Regenerative Medicine Center of Thailand, we utilize allogenic stem cells from ethically sourced and reliable origins for treating Coronary Artery Disease (CAD), Acute Coronary Syndrome (ACS), and heart attacks (myocardial infarction, MI). Our cellular therapies include progenitor stem cells obtained either from the patient or through ethically sourced donations. In particular, we leverage stem cells from umbilical cord blood, placenta, amniotic fluid, and dental pulp—all obtained after the healthy delivery of a child.
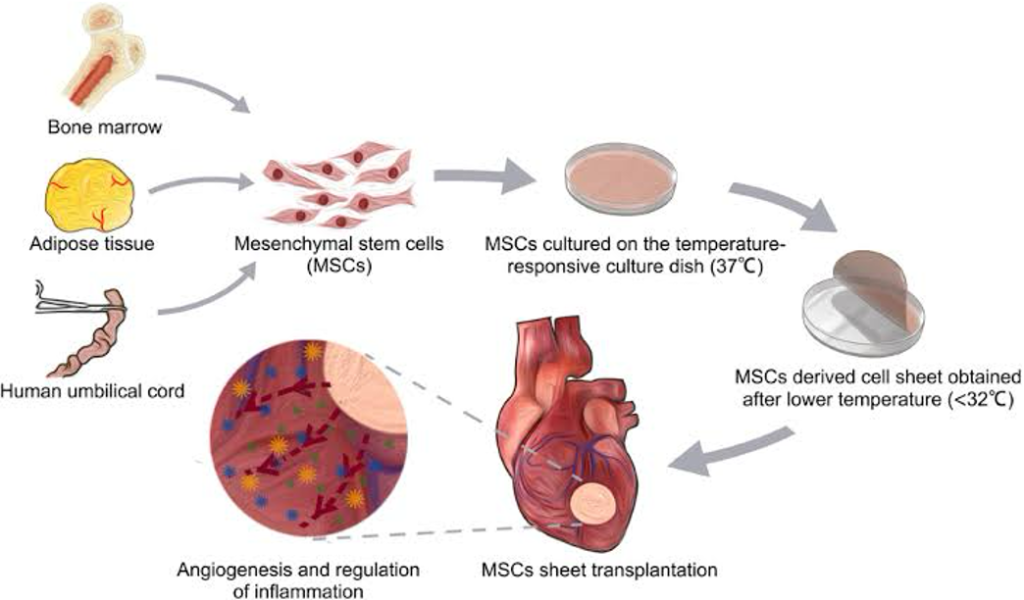
These valuable tissues, often discarded as medical waste, offer a rich source of stem cells that can be stored or donated for regenerative therapies. Umbilical cord blood and placental tissues are particularly rich in hematopoietic and mesenchymal stem cells (MSCs), which have been shown to support tissue repair, reduce inflammation, and promote angiogenesis—critical in restoring heart function after a heart attack. Amniotic fluid also contains a variety of stem cells capable of differentiating into multiple cell types, facilitating myocardial repair in cases of ischemic heart disease.
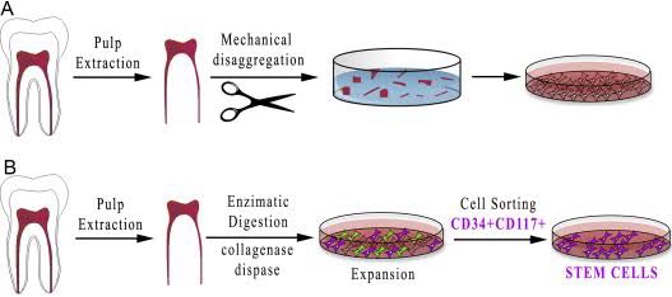
In addition, we utilize stem cells from dental pulp, which contains mesenchymal stem cells that exhibit powerful regenerative capabilities, especially in tissue repair and cardiovascular health. These cells can be harvested from healthy dental tissue, offering an alternative source for stem cell-based therapies aimed at cardiac regeneration and repair of damaged heart tissue following a heart attack[42-46].
35. Ethical Commitment to Cellular Therapy for Heart Disease
Our center is firmly committed to the ethical use of stem cells in the treatment of CAD and related conditions. We strictly prohibit the use of embryonic stem cells (ESCs) or any stem cells sourced from animals, such as those derived from sheep or cows. Our therapies rely exclusively on human-derived, ethically sourced stem cells, ensuring safety, efficacy, and respect for medical ethics in the application of regenerative medicine.
We believe that the future of heart disease treatment lies in safe, human-derived, allogenic stem cell therapies that focus on restoring heart function and reducing the long-term effects of ischemic heart disease through natural, minimally invasive methods.
36. Expected Timeline for Benefits of Cellular Therapy in the Treatment of CAD, IHD, ACS, and Heart Attack
Our specialized protocols of Cellular Therapy and Stem Cells for Coronary Artery Disease (CAD), Ischemic Heart Disease (IHD), Acute Coronary Syndrome (ACS), and heart attack (myocardial infarction, MI) frequently result in significant improvements shortly after treatment initiation. Many patients experience initial benefits after the first or second session, during which they receive infusions of 20-30 million enhanced Mesenchymal Stem Cells (MSCs) in combination with Cardiac Progenitor Stem CellsGrowth Factors and Peptides. These cells target damaged heart tissue, facilitating myocardial regeneration, reducing inflammation, and promoting angiogenesis to enhance blood flow.
The regenerative effects of the therapy typically progress over the following months. Notable improvements in cardiac function—such as increased ejection fraction, reduced chest pain, and better exercise tolerance—are frequently observed at the 2-, 4-, and 6-month intervals post-therapy, with lasting benefits over time. These improvements contribute to enhanced quality of life, a reduced risk of recurrent myocardial infarctions, and slowed progression of CAD/ACS and IHD.
For sustained benefits, our Cardiac Regeneration Protocols of Stem Cells for CAD/IHD are most effective when paired with lifestyle changes and participation in cardiac rehabilitation programs. These programs emphasize exercise, dietary modifications, stress management, and smoking cessation, which are essential for maximizing the potential of Cellular Therapy to restore heart function and prevent future cardiovascular events. Long-term commitment to this holistic approach optimizes the outcomes of Cellular Therapy, offering patients a comprehensive path to heart recovery and improved survival.
37. Comprehensive Approach to Treating Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) with Progenitor Stem Cells for Heart Diseases
When it comes to treating Acute Coronary Syndrome (ACS) and Coronary Artery Disease (CAD) with progenitor stem cells, it is crucial to acknowledge that each patient is unique and may require a tailored approach. The duration and cost of the treatment will depend on various factors, including the patient’s current health status, the severity of the CAD/ACS, and the presence of any underlying medical conditions. To ensure the best possible outcome, our medical team will need to thoroughly review your relevant medical information, including recent cardiac tests and biomarkers. This comprehensive evaluation will allow us to develop a customized treatment plan that incorporates Cardiomyocyte Progenitor Stem Cells (Cardiomyocytes-PSCs), Endothelial Progenitor Stem Cells (Endothelial-PSCs), Smooth Muscle Progenitor Stem Cells (Smooth Muscle-PSCs), and other relevant progenitor cells to address your specific needs and maximize the chances of success (Bakinowska et al., 2024; Cyganek et al., 2009).
It is important to note that the success rates of stem cell therapy for CAD/ACS can vary depending on the stage and severity of the disease. However, the advancements in progenitor stem cell research have shown promising results in promoting cardiac regeneration and improving outcomes for patients with CAD/ACS. If you are interested in learning more about this innovative treatment option and how it can potentially transform your life, we encourage you to contact us today. Our dedicated team is here to provide you with the information and support you need to make an informed decision about your health. We understand the challenges and frustrations that come with living with CAD/ACS, and we are committed to helping you find a comprehensive solution that will improve your quality of life.
38. What Sets Apart Our Specialized Protocols of Cellular Therapy and Stem Cells for Treating Coronary Artery Disease (CAD) and Acute Coronary Syndrome (ACS) ?
At our state-of-the-art Anti-Aging and Regenerative Medicine Center, we stand at the forefront of innovation in the treatment of Coronary Artery Disease (CAD) and Acute Coronary Syndrome (ACS). Our approach integrates advanced Cellular Therapy and various Cardiac Progenitor Stem Cells, offering a cutting-edge, holistic solution for patients with all types of cardiovascular conditions. Our team of cardiologists and regenerative medical specialists has over 20 years of experience, and we design specialized protocols that go beyond symptom management to actively promote hearttissueregeneration, particularly for patients who seek our intervention promptly after diagnosis.
Timing is critical in cardiovascular care, and patients who begin our treatment early experience optimal outcomes. Unlike conventional treatments that primarily manage symptoms or repair damage through invasive procedures like bypass surgery or angioplasty, our regenerative protocols aim to heal damaged heart tissue and reverse the effects of CAD and ACS. By utilizing stem cells, including cardiomyocyte progenitor stem cells (cardiomyocytes-PSCs), endothelial progenitor stem cells (endothelial-PSCs), and smooth muscle progenitor stem cells (smooth muscle-PSCs), we target the root cause of the disease and promote new tissue growth, angiogenesis, and the restoration of healthy cardiac function.
Our holistic approach doesn’t just treat the heart as an isolated organ, but considers the patient’s entire body, mind, soul, and spirit. We believe that true healing is achieved when all aspects of a patient’s well-being are addressed. Our protocols are designed to optimize both mental and physical health, preparing patients to fully benefit from Cellular Therapy and Progenitor Stem Cells. A healthy mental state, in combination with a prepared and responsive body, enhances therapeutic outcomes and ensures the best possible results in terms of heart function recovery and overall health.
By integrating cardiac fibroblast progenitor stem cells (cardiac fibroblast-PSCs) and vascular progenitor stem cells (vascular-PSCs) into our protocols, we not only repair damaged heart tissue but also regenerate the vascular structures critical to preventing future cardiovascular events. This comprehensive, personalized treatment plan addresses the entire spectrum of CAD and ACS, offering a more promising alternative to traditional invasive methods.
Our team has successfully treated countless patients, guiding them through this regenerative journey. We emphasize that each individual is more than just their diagnosis, and that a proactive, holistic, and regenerative approach to heart health can lead to significantly improved outcomes.
39. Mechanisms of Action of Cellular Therapy and Cardiac Progenitor Stem Cells in CAD/MI Treatment
Cellular therapy and cardiac progenitor stem cells have emerged as promising interventions for Coronary Artery Disease (CAD), ischemic heart disease (IHD), and myocardial infarction (MI). These therapies aim to regenerate damaged heart tissue, improve heart function, and reduce the extent of ischemic injury. Below are the key mechanisms of action and strategies to optimize their therapeutic efficacy for clinical applications:
1. Mesenchymal Stem Cells (MSCs) and Their Role in Cardiac Repair
MSCs are multipotent stem cells known for their ability to differentiate into various cell types, including cardiomyocytes, endothelial cells, and smooth muscle cells, which are essential for heart tissue repair. MSCs act through:
– Paracrine signaling: MSCs release growth factors and cytokines that promote angiogenesis, reduce inflammation, and enhance tissue regeneration.
– Modulation of immune response: MSCs can suppress harmful inflammatory responses after a heart attack, protecting the heart from further damage【25†source】【26†source】.
– Differentiation into cardiac-like cells: Though limited, MSCs can differentiate into cardiomyocytes and vascular cells, contributing to the structural repair of the myocardium.
2. Cardiac Progenitor Cells (CPCs)
CPCs are specialized stem cells that reside in the heart and have the ability to differentiate into various cell types of the myocardium, including cardiomyocytes, endothelial cells, and smooth muscle cells. Their mechanisms include:
– Cardiomyocyte regeneration: CPCs can replace lost or damaged cardiomyocytes after MI, aiding in myocardial tissue restoration.
– Enhancing contractile function: By regenerating functional heart tissue, CPCs can improve the contractility of the heart, which is often compromised in CAD patients.
– Supporting angiogenesis: CPCs promote the formation of new blood vessels, improving blood flow to ischemic regions of the heart【25†source】.
3. Endothelial Progenitor Cells (EPCs)
EPCs contribute primarily to vascular repair and the formation of new blood vessels (angiogenesis). After a heart attack or ischemic event, EPCs are recruited to the site of injury to:
– Revascularize ischemic tissue: EPCs promote the formation of new blood vessels in the heart, restoring blood flow to oxygen-deprived areas.
– Reduce endothelial dysfunction: By repairing damaged blood vessels, EPCs help restore the integrity of the vascular endothelium, which is essential for normal heart function【25†source】.
4. Optimization of Stem Cell Therapies for Clinical Use
– Cell sourcing and delivery: To maximize efficacy, stem cells can be sourced from autologous (patient’s own) or allogeneic (donor) tissue. Autologous cells reduce the risk of immune rejection, while allogeneic cells offer more standardized and readily available options. Delivery methods include direct intracoronary infusion or injection into the myocardium to ensure targeted treatment.
– Preconditioning of stem cells: Enhancing the therapeutic potential of stem cells can be achieved by preconditioning them with hypoxia, growth factors, or genetic modifications. This process increases their survival, paracrine activity, and regenerative capabilities after transplantation【26†source】.
– Combining with biomaterials: Scaffolds or hydrogels can be used in conjunction with stem cells to provide structural support, improve cell retention, and enhance tissue integration in the heart【25†source】.
5. Challenges and Future Directions
Despite the promise of stem cell therapy for CAD and MI, there are still challenges related to optimizing the delivery, survival, and differentiation of stem cells in the harsh environment of the injured heart. Ongoing research focuses on genetic engineering, using exosomes derived from stem cells, and combining stem cells with bioactive molecules to enhance therapeutic outcomes.
Cellular Therapy and Stem cells for CAD, particularly involving MSCs, CPCs, and EPCs, offer substantial potential in regenerating damaged heart tissue, promoting angiogenesis, and improving heart function in CAD and MI patients. Future clinical applications will likely benefit from advances in optimizing cell delivery, preconditioning, and the use of supportive biomaterials【25†source】【26†source】.
40. Types of Stem Cells Used in the Treatment of Coronary Artery Disease (CAD), Acute Myocardial Infarction (AMI), and Acute Coronary Syndrome (ACS)
– General Description: BMDCS are a type of adult stem cell obtained from the bone marrow. They have the ability to differentiate into various cell types, including cardiomyocytes, and are used to repair damaged heart tissue.
– Institution: Cleveland Clinic
– Researcher: Dr. Roberto Bolli
– Year: 2005
– Dosage: 100 million cells injected
– Type of Model: Clinical trial involving patients with heart failure post-AMI
– Outcome: Improved left ventricular function and reduced scar size, demonstrating the potential of BMDCS in cardiac repair.
– General Description: MSCs are multipotent stem cells found in various tissues, including bone marrow and adipose tissue. They are known for their regenerative properties and ability to modulate immune responses.
– Institution: Mayo Clinic
– Researcher: Dr. Joshua M. Hare
– Year: 2012
– Dosage: 200 million cells injected
– Type of Model: Phase I clinical trial in patients with ischemic heart disease
– Outcome: Enhanced cardiac function and improved quality of life, with a favorable safety profile.
– General Description: UC-MSCs are derived from the Wharton’s jelly of the umbilical cord. They are abundant, easily accessible, and have shown promise in cardiac regeneration due to their immunomodulatory properties.
– Institution: University of California, San Diego
– Researcher: Dr. C. Richard Contag
– Year: 2014
– Dosage: 150 million cells injected
– Type of Model: Preclinical study in a porcine model of myocardial ischemia
– Outcome: Significant improvement in myocardial perfusion and reduced infarct size, indicating their potential for cardiac repair.
4. Cardiosphere-Derived Cells (CDCs)
– General Description: CDCs are a type of cardiac stem cell derived from heart tissue. They have the ability to differentiate into cardiomyocytes and promote cardiac regeneration.
– Institution: University of Miami
– Researcher: Dr. Joshua Hare
– Year: 2013
– Dosage: 20 million cells injected
– Type of Model: Phase II clinical trial in patients with heart failure
– Outcome: Improved heart function and reduced symptoms of heart failure, supporting the use of CDCs in cardiac therapies.
– General Description: iPSCs are reprogrammed somatic cells that exhibit pluripotency, allowing them to differentiate into any cell type, including cardiomyocytes. They hold great potential for personalized regenerative therapies.
– Institution: Stanford University
– Researcher: Dr. Shinya Yamanaka
– Year: 2016
– Dosage: Varies based on differentiation protocols
– Type of Model: Preclinical studies using animal models
– Outcome: Successful generation of functional cardiomyocytes from iPSCs, paving the way for future clinical applications in CAD and AMI.
6. Epicardial Stem Cells
– General Description: Epicardial stem cells are derived from the epicardium, the outer layer of the heart. They play a role in heart development and repair and are being explored for their regenerative capabilities.
– Institution: University of Pennsylvania
– Researcher: Dr. John A. Chute
– Year: 2018
– Dosage: 50 million cells injected
– Type of Model: Clinical trial in patients with ischemic heart disease
– Outcome: Promoted cardiac repair and improved function, demonstrating the potential of epicardial cells in regenerative therapies[47-52].
These various types of stem cells represent promising avenues for the treatment of coronary artery disease, acute myocardial infarction, and acute coronary syndrome, with ongoing research aimed at optimizing their use for cardiac repair and regeneration.
41. Exosome Cellular Therapy and Stem cells for CAD/AMI/ACS
Patients with coronary artery disease (CAD), myocardial infarction (MI), and acute coronary syndrome (ACS) can benefit substantially from our Cellular Therapy and Stem Cell treatments, complemented by Exosomes. These approaches represent a sophisticated alternative to traditional treatments, which primarily focus on symptom management and revascularization, rather than addressing the underlying causes of cardiovascular disease by harnessing the regenerative potential of Stem Cells.
Cellular Therapy and Stem Cell Treatments
Stem cells, particularly mesenchymal stem cells (MSCs) and cardiac progenitor cells, exhibit the ability to differentiate into various cardiac cell types, including cardiomyocytes, endothelial cells, and smooth muscle cells. This capability allows for the replenishment of damaged myocardial structures, thereby targeting the root causes of cardiovascular deficits. Studies have shown that cellular therapy and stem cells for CAD, ACS, AMI can lead to functional improvements in animal models of myocardial infarction and chronic ischemic heart disease, suggesting their potential for human applications as well [53][54][55].
Role of Exosomes
Exosomes derived from stem cells serve as crucial mediators of paracrine signaling. They orchestrate a cascade of molecular events that promote cardioprotection, angiogenesis, and modulate immune responses. By activating endogenous repair mechanisms and secreting cardiotrophic factors, these exosomes facilitate the reconstruction of cardiac tissue, which can lead to accelerated recovery and measurable improvements in cardiac function. Research indicates that stem cells for CAD, particularly when enhanced with exosomes, can surpass the limitations of conventional interventions in treating cardiovascular disease-induced myocardial damage and dysfunction [54][55][56].
The integration of our Cellular Therapy and Stem Cells for CAD, MI, ACS, alongside Exosomes, presents a promising avenue for improving outcomes in patients with heart diseases of all types and stages. This approach not only addresses immediate symptoms but also fosters long-term cardiac recovery and functional restoration, marking a significant advancement in cardiovascular disease management strategies [54-56].
42. Types of Coronary Artery Disease, Acute Coronary Syndrome, Myocardial Infarction, and Ischemic Heart Disease
Coronary artery disease (CAD), acute coronary syndrome (ACS), myocardial infarction (MI), and ischemic heart disease (IHD) are closely related conditions that involve the reduction of blood flow to the cardiac muscle due to atherosclerotic plaque buildup in the arteries of the heart. There are several types of these conditions, each with its own characteristics and implications.
Coronary Artery Disease Types
1. Obstructive Coronary Artery Disease
– Caused by gradual plaque buildup in the coronary arteries, leading to narrowing and reduced blood flow
– Can progress to a complete blockage, resulting in a heart attack
– Symptoms include chest pain, shortness of breath, and fatigue
2. Nonobstructive Coronary Artery Disease
– Caused by problems other than plaque buildup, such as artery spasms or dissection
– Can still cause symptoms like chest pain and shortness of breath
– More common in women
3. Spontaneous Coronary Artery Dissection (SCAD)
– Sudden tearing of the coronary artery wall, leading to a partial or complete blockage
– Often presents as a heart attack
– Symptoms vary but may include chest pain, shortness of breath, and nausea
Acute Coronary Syndrome Types
1. Unstable Angina
– Chest pain that occurs at rest or with minimal exertion
– A type of heart attack where the artery is partially blocked
– Causes damage to a portion of the heart muscle
– Symptoms may be similar to unstable angina
3. ST-Elevation Myocardial Infarction (STEMI)
– A severe type of heart attack where the artery is completely blocked
– Causes extensive damage to the heart muscle
– Requires immediate treatment to restore blood flow
Myocardial Infarction Types
1. STEMI
– Caused by a complete blockage of a coronary artery
– Requires immediate treatment to restore blood flow and minimize damage
2. NSTEMI
– Caused by a partial blockage of a coronary artery
– Causes damage to a portion of the heart muscle
– Symptoms may be similar to unstable angina
Ischemic Heart Disease Types
1. Stable Angina
– Chest pain that occurs with exertion and is relieved by rest
– Caused by a partially blocked artery
– Symptoms are predictable and consistent
2. Unstable Angina
– Chest pain that occurs at rest or with minimal exertion
– Caused by a partially blocked artery
– Requires immediate medical attention
3. Myocardial Infarction
– A heart attack caused by a complete or partial blockage of a coronary artery
– Causes damage to the heart muscle
– Requires immediate treatment to restore blood flow and minimize damage
Understanding the different types of CAD, ACS, MI, and IHD is crucial for accurate diagnosis, appropriate treatment, and effective management of these conditions. Early recognition of symptoms and prompt medical intervention can significantly improve outcomes for patients[56.1-59].
43. Common Causes of Coronary Artery Disease (CAD), Acute Coronary Syndrome (ACS), Atherosclerosis, and Heart Attack
Coronary artery disease (CAD), acute coronary syndrome (ACS), atherosclerosis, and heart attacks are interrelated conditions primarily driven by similar risk factors and underlying mechanisms. Understanding these causes is crucial for prevention and management.
1. Atherosclerosis
– Description: Atherosclerosis is the buildup of fatty deposits (plaque) in the arterial walls, leading to narrowing and hardening of the arteries. This process restricts blood flow and can ultimately result in heart attacks.
– Causes:
– High levels of low-density lipoprotein (LDL) cholesterol
– Inflammation
– High blood pressure
– Smoking
2. High Blood Pressure (Hypertension)
– Description: Chronic high blood pressure can damage arteries over time, making them more susceptible to plaque buildup and atherosclerosis.
– Impact: It is often termed the “silent killer” because it typically presents no symptoms until significant damage has occurred.
– Description: Diabetes leads to high blood sugar levels, which can damage blood vessels and accelerate atherosclerosis.
– Impact: Individuals with diabetes are at a significantly higher risk of developing CAD and experiencing heart attacks compared to those without diabetes.
6. Obesity
– Description: Excess body weight contributes to other risk factors such as high blood pressure, high cholesterol, and diabetes.
– Impact: Obesity increases the workload on the heart and can lead to heart failure and other cardiovascular complications.
7. Sedentary Lifestyle
– Description: Lack of physical activity contributes to obesity and other cardiovascular risk factors.
– Impact: Regular exercise helps maintain a healthy weight, lowers blood pressure, and improves cholesterol levels, reducing the risk of CAD.
– Description: Chronic stress may lead to unhealthy coping mechanisms such as poor diet, smoking, or excessive alcohol consumption.
– Impact: Stress can also trigger physiological responses that increase heart rate and blood pressure, contributing to heart disease.
9. Family History
– Description: A family history of heart disease can increase an individual’s risk due to genetic factors.
– Impact: While genetics cannot be changed, awareness can lead to proactive management of modifiable risk factors.
10. Sleep Apnea
– Description: This condition, characterized by interrupted breathing during sleep, is associated with high blood pressure and arrhythmias.
– Impact: Sleep apnea can lead to increased cardiovascular risk, including CAD and heart attacks.
Understanding these common causes can help individuals make informed lifestyle choices and seek appropriate medical interventions to reduce their risk of CAD, ACS, and heart attacks[60-62].
44. Stages of Coronary Artery Disease (CAD), Ischemic Heart Disease (IHD), and Acute Coronary Syndrome (ACS)
Coronary artery disease (CAD), ischemic heart disease (IHD), and acute coronary syndrome (ACS) progress through several stages, reflecting the severity of the disease and the extent of arterial blockage. Understanding these stages is crucial for early detection and intervention.
Stages of Coronary Artery Disease (CAD)
1. Initial Stage (Endothelial Dysfunction)
– Description: The process begins with damage to the endothelial lining of the coronary arteries, often due to risk factors such as high cholesterol, hypertension, and smoking. This damage leads to increased permeability and inflammation.
– Impact: Endothelial dysfunction is a precursor to atherosclerosis, allowing LDL cholesterol to infiltrate the arterial wall.
2. Fatty Streak Formation
– Description: Accumulation of lipid-laden macrophages (foam cells) occurs, forming fatty streaks in the arterial wall. This stage is often asymptomatic.
– Impact: Fatty streaks are the earliest visible signs of atherosclerosis and indicate the beginning of plaque development.
3. Plaque Development
– Description: Over time, fatty streaks evolve into more complex atherosclerotic plaques consisting of lipids, inflammatory cells, and fibrous tissue. Plaques can be stable or unstable.
– Impact: Stable plaques may cause narrowing of the artery, while unstable plaques are prone to rupture, leading to acute events.
4. Narrowing of the Artery (Obstructive CAD)
– Description: As plaques grow, they narrow the coronary arteries, reducing blood flow to the heart muscle. This stage can lead to symptoms such as angina (chest pain) during exertion.
– Impact: Significant narrowing (over 50%) can lead to ischemia, where the heart muscle does not receive enough oxygen-rich blood.
5. Acute Coronary Syndrome (ACS)
– Description: ACS encompasses unstable angina and myocardial infarction (heart attack). It occurs when a plaque ruptures, leading to the formation of a blood clot that can completely block blood flow.
– Impact: This stage requires immediate medical intervention to restore blood flow and minimize heart damage.
Stages of Ischemic Heart Disease (IHD)
1. Stable Angina
– Description: Characterized by predictable chest pain or discomfort during physical activity or stress, stable angina indicates that the heart is not receiving enough blood due to narrowed arteries.
– Impact: Symptoms are relieved by rest or nitroglycerin.
2. Unstable Angina
– Description: This stage involves sudden chest pain that occurs at rest or with minimal exertion and may last longer than stable angina.
– Impact: Unstable angina is a medical emergency and can precede a heart attack.
3. Myocardial Infarction (Heart Attack)
– Description: A heart attack occurs when blood flow to a part of the heart is blocked for an extended period, causing damage to the heart muscle.
– Impact: Symptoms may include severe chest pain, shortness of breath, and other signs of distress.
Understanding the stages of CAD, IHD, and ACS is vital for recognizing symptoms, seeking timely medical assistance, and implementing preventive measures. Early detection and management can significantly improve outcomes and reduce the risk of severe complications[63-64].
45. Prognosis of Coronary Artery Disease (CAD), Ischemic Heart Disease (IHD), Acute Coronary Syndrome (ACS), and Heart Attack
The prognosis of CAD, IHD, ACS, and heart attacks varies significantly based on several factors, including the severity of the disease, the presence of comorbid conditions, and the effectiveness of treatment strategies. Understanding these prognostic factors is crucial for patient management and improving outcomes.
1. Coronary Artery Disease (CAD)
– Early Stages: In the initial stages of CAD, patients may remain asymptomatic, but the disease can progress silently. Early detection through screening can lead to lifestyle modifications and medical management, which can significantly improve prognosis.
– Advanced Stages: As CAD progresses, patients may experience angina and other symptoms. The prognosis at this stage depends on the extent of arterial blockage and the presence of collateral circulation. Patients with stable angina generally have a better prognosis than those with unstable angina or advanced CAD.
2. Ischemic Heart Disease (IHD)
– Stable IHD: Patients with stable IHD often have a favorable prognosis with appropriate management, including lifestyle changes and pharmacotherapy. Regular follow-up and monitoring are essential for maintaining heart health.
– Unstable IHD: The prognosis for patients with unstable angina or recent myocardial infarction is more guarded. These patients are at higher risk for recurrent events and require aggressive treatment strategies, including revascularization procedures.
3. Acute Coronary Syndrome (ACS)
– Unstable Angina: Patients presenting with unstable angina have a higher risk of progression to myocardial infarction. The prognosis improves with timely intervention, such as angioplasty or coronary artery bypass grafting (CABG).
– Myocardial Infarction: The prognosis following a heart attack depends on various factors, including the size of the infarct, the time to treatment, and the patient’s overall health. Early intervention is critical in minimizing heart damage and improving long-term outcomes. Patients who receive prompt treatment often have better prognoses.
4. Heart Attack
– Immediate Prognosis: The immediate prognosis after a heart attack is influenced by the extent of myocardial damage and the success of reperfusion therapy. Patients with larger infarcts or complications such as heart failure or arrhythmias have a poorer prognosis.
– Long-term Prognosis: Long-term outcomes depend on cardiac rehabilitation, lifestyle changes, and adherence to medication regimens. Patients who engage in cardiac rehabilitation and maintain a heart-healthy lifestyle can significantly improve their prognosis and quality of life.
The prognosis for CAD, IHD, ACS, and heart attacks is multifaceted and influenced by the disease stage, treatment effectiveness, and patient adherence to lifestyle modifications. Early detection and intervention are key to improving outcomes and reducing the risk of severe complications.
46. How Cellular Therapy and Cardiac Progenitor Stem Cells Improve Prognosis of CAD, IHD, ACS, and Heart Attack
Cellular therapy, particularly the application of various cardiac progenitor stem cells, has emerged as a promising strategy for improving the prognosis of patients with coronary artery disease (CAD), ischemic heart disease (IHD), acute coronary syndrome (ACS), and heart attacks. These therapies aim to regenerate damaged heart tissue and restore cardiac function through several mechanisms.
Mechanisms of Action
1. Regeneration of Myocardial Tissue: Cardiac progenitor stem cells (CPCs) possess the ability to differentiate into cardiomyocytes, endothelial cells, and smooth muscle cells. This differentiation is crucial for repairing the damaged myocardial tissue following ischemic events, thereby improving heart function and reducing the risk of heart failure.
2. Angiogenesis: CPCs promote the formation of new blood vessels in the heart through a process called angiogenesis. By enhancing blood supply to ischemic areas, these cells help to restore oxygen delivery and nutrient supply to the heart muscle, which is vital for recovery after a heart attack.
3. Paracrine Effects: Cardiac progenitor cells secrete various growth factors and cytokines that have protective and regenerative effects on the heart. These paracrine factors can reduce inflammation, inhibit apoptosis (cell death), and stimulate the proliferation of resident cardiac cells, further aiding in tissue repair.
4. Improvement of Cardiac Function: Clinical studies have shown that the administration of CPCs can lead to significant improvements in left ventricular ejection fraction (LVEF) and overall cardiac function. For instance, patients receiving CPC therapy after myocardial infarction have reported better functional outcomes and quality of life.
5. Reduction of Scar Formation: By promoting tissue regeneration and reducing inflammation, CPCs can limit the extent of scar formation following a heart attack. This is crucial, as excessive scar tissue can lead to further complications, including heart failure and arrhythmias.
The integration of cellular therapy and cardiac progenitor stem cells into treatment protocols for CAD, IHD, ACS, and heart attacks presents a novel approach to enhance patient prognosis. By addressing the underlying causes of heart disease and facilitating tissue regeneration, these therapies hold the potential to improve outcomes and quality of life for patients suffering from these conditions[65-68].
47. Our Commitment to Safety and Quality in Cellular Therapy and Stem Cells for CAD, IHD, and ACS
At our Cellular Therapy and Stem Cell Laboratory, we are dedicated to providing the safest and most effective treatments for patients with coronary artery disease (CAD), ischemic heart disease (IHD), and acute coronary syndrome (ACS). With over 20 years of experience in assisting patients from around the world, we have established a reputation for excellence and a steadfast commitment to quality and safety.
Our laboratory, located at the Thailand Science Park, adheres to the highest safety standards and is registered with the Thai FDA for cellular therapy and pharmaceutical production. We have obtained certifications for good laboratory practice (GLP) and good manufacturing practice (GMP), ensuring that our processes meet the strictest regulatory requirements. Furthermore, our laboratory has achieved ISO4 and Class 10 certifications for ultra-cleanroom cell culture and biotechnology, guaranteeing the utmost standards of quality and safety in our stem cell products.
The safety and efficacy of our allogeneic stem cell therapies are well-documented in numerous clinical trials, providing a solid scientific foundation for their use in regenerative medicine. Our treatments have been shown to improve cardiac function, reduce scar tissue formation, and promote angiogenesis in patients with CAD, IHD, and ACS.
By combining our extensive experience, rigorous safety protocols, and scientific validation, we are confident in our ability to provide our patients with the highest quality of care. Our commitment to excellence is evident in every aspect of our work, from the selection of our stem cell lines to the meticulous monitoring of our patients’ progress.
At our Cellular Therapy and Stem Cell Laboratory of Anti-Aging and Regenerative Medicine Center of Thailand, we believe that every patient deserves access to safe and effective treatments. We are dedicated to advancing the field of regenerative medicine and improving the lives of those affected by cardiovascular diseases.
48. Primary Outcome Assessments in Patients with CAD, ACS, IHD, and Heart Attack
The assessment of primary outcomes in patients with coronary artery disease (CAD), acute coronary syndrome (ACS), ischemic heart disease (IHD), and heart attacks is essential for evaluating treatment effectiveness and improving patient care. Below are the key primary outcome measures identified for these conditions:
– Cardiac Biomarkers: Levels of troponin and other cardiac enzymes to assess myocardial injury and guide treatment decisions.
– Lipid Profiles: Monitoring cholesterol levels, particularly LDL and HDL, to evaluate cardiovascular risk and treatment effectiveness.
7. Procedural Outcomes
– Revascularization Procedures: Rates of successful percutaneous coronary interventions (PCI) or coronary artery bypass grafting (CABG).
– Complications Related to Procedures: Monitoring for adverse events associated with cardiac interventions.
8. Return to Daily Activities
– Work and Productivity: Assessing the ability of patients to return to work and engage in normal activities post-treatment.
These primary outcome assessments provide a comprehensive framework for evaluating the effectiveness of treatments in patients with CAD, ACS, IHD, and heart attacks. By focusing on both clinical and patient-reported outcomes, healthcare providers can better understand the impact of interventions and improve patient care[69-72].
49. Enhancing Patient Outcomes in CAD, IHD, ACS, and Heart Attack Through Advanced Cellular Therapy
Our specialized treatment protocols utilizing cellular therapy and various cardiac progenitor stem cells, including mesenchymal stem cells (MSCs), cardiac progenitor cells (CPCs), and endothelial progenitor cells (EPCs), are designed to significantly improve primary outcomes for patients with coronary artery disease (CAD), ischemic heart disease (IHD), acute coronary syndrome (ACS), and heart attacks. These therapies aim to enhance myocardial regeneration, promote angiogenesis, and improve cardiac function.
By delivering targeted cellular therapies, we facilitate the repair of damaged heart tissue, reduce scar formation, and improve overall cardiac performance. Our protocols are supported by rigorous scientific validation, demonstrating that these progenitor stem cells can lead to measurable improvements in left ventricular ejection fraction (LVEF), reductions in major adverse cardiac events (MACE), and enhanced quality of life for patients. The integration of these advanced therapies into treatment regimens not only addresses the symptoms of heart disease but also fosters long-term recovery and improved prognosis, making them a vital component of modern cardiovascular care.
50. Comprehensive Treatment Protocols for CAD, IHD, ACS, and Atherosclerosis
At our Anti-Aging and Regenerative Medicine Center in Thailand, we offer a specialized treatment protocol that combines cellular therapy and various progenitor stem cells with complementary therapies to enhance patient outcomes for those suffering from coronary artery disease (CAD), ischemic heart disease (IHD), acute coronary syndrome (ACS), and atherosclerosis. Each component of our protocol is designed to work synergistically, addressing the multifaceted nature of cardiovascular health.
Cellular Therapy and Progenitor Stem Cells
– Mesenchymal Stem Cells (MSCs): These cells can differentiate into cardiomyocytes and endothelial cells, promoting myocardial regeneration and improving cardiac function in patients with CAD and IHD.
– Cardiac Progenitor Stem Cells (CPCs): CPCs secrete growth factors that stimulate angiogenesis and reduce inflammation, which is vital for recovery in ACS and atherosclerosis.
– Endothelial Progenitor Cells (EPCs): EPCs contribute to the repair of damaged blood vessels, enhancing blood flow and reducing ischemic symptoms in patients with CAD.
Complementary Therapies
1. IM Placenta Extract Therapy: Human placental extract contains growth factors, peptides, and cytokines that promote tissue regeneration and reduce inflammation, aiding recovery and improving vascular health in CAD patients.
2. Intensive Growth Factors and Peptide Therapy: This therapy enhances cellular repair mechanisms and promotes angiogenesis through the administration of specific growth factors that stimulate heart tissue regeneration.
3. Plasmapheresis Therapy: By removing harmful substances from the bloodstream, such as LDL cholesterol and inflammatory markers, plasmapheresis helps improve endothelial function and reduce plaque buildup in atherosclerosis.
4. Meyer’s Cocktail Therapy: This intravenous infusion of vitamins and minerals supports overall health and may enhance energy levels and recovery in patients with chronic cardiovascular conditions.
5. Ozone Therapy: Ozone therapy improves oxygen delivery to tissues, enhances endothelial function, and reduces oxidative stress, making it beneficial for patients with IHD and CAD.
6. Chelation Therapy: This therapy removes heavy metals and excess calcium from the bloodstream, which can improve blood flow and reduce the risk of cardiovascular events in patients with atherosclerosis.
7. Multivitamin and High-Dose Vitamin C Therapy: These therapies provide essential nutrients that support heart health, boost the immune system, and reduce oxidative stress, contributing to improved outcomes in CAD patients.
8. NAD+ Therapy: NAD+ is crucial for cellular metabolism and energy production. Supplementing with NAD+ can enhance mitochondrial function, improve energy levels, and support heart health.
9. Plaquex Therapy: This therapy aims to reduce cholesterol levels and improve lipid profiles, helping to prevent further plaque buildup in the arteries.
10. IV Glutathione Therapy: Glutathione is a powerful antioxidant that helps reduce oxidative stress and inflammation, supporting cardiovascular health and recovery.
11. Physical Therapy: Tailored exercise programs improve cardiovascular fitness, enhance functional capacity, and reduce symptoms in patients with CAD and IHD.
12. Chinese Acupuncture and Cupping: These traditional therapies can alleviate symptoms, improve circulation, and promote overall well-being in patients with cardiovascular conditions.
13. Homeopathy: Homeopathic treatments may provide additional support for symptom management and overall health, complementing conventional therapies.
14. Thai massage (TM) : Also known as Nuad bo-rarn, is a traditional healing practice that combines acupressure, assisted yoga poses, and deep stretching to enhance physical and mental well-being. Its unique approach focuses on energy pathways and holistic health.
15. Traditional Chinese Medicine (TCM) : An ancient medical system originating over 2,000 years ago, emphasizing the balance of energy, or qi, within the body. TCM views health as a harmonious balance between opposing forces known as yin and yang.
16. Energy medicine : A branch of alternative medicine based on the belief that practitioners can channel “healing energy” into patients to promote positive health outcomes.
17. Meditation : A practice that involves techniques aimed at enhancing attention, emotional awareness, and mental calmness.
18. Magnetic field therapy, often referred to as magnetic therapy, involves the application of static or pulsed electromagnetic fields to promote healing and alleviate pain.
By integrating these diverse approaches, we aim to create a comprehensive strategy for recovery and rejuvenation, ensuring that our patients receive the most effective and holistic care possible for their cardiovascular health.
51. Enhancing Patient Outcomes in CAD, IHD, ACS, and Heart Attack Through Cellular Therapy
Pre and Post PCI of one of our International Patient’s Improved Circulation Outcomes 6 months after our Cellular Therapy and Stem Cells for CAD/ACS at Right Coronary Artery
Following our specialized Cellular Therapy and the application of various progenitor stem cells at our center, patients with coronary artery disease (CAD), ischemic heart disease (IHD), acute coronary syndrome (ACS), and heart attacks have shown significant improvements. Within the initial weeks post-treatment, patients report enhanced cardiac function, reduced symptoms, and improved quality of life.
Our patients experience notable increases in exercise tolerance and reductions in angina episodes, supported by objective measures such as improved left ventricular ejection fraction (LVEF) and favorable changes in cardiac biomarkers. Clinical assessments, including echocardiograms and stress tests, demonstrate enhanced myocardial perfusion and overall heart health. Even individuals with advanced CAD/ACS or those who have suffered severe heart attacks have shown remarkable recovery after undergoing our comprehensive treatment protocols that include cellular therapy and various progenitor stem cells.
The best-case scenarios for some of our patients have resulted in sustained improvements in cardiac function and quality of life for over three years, showcasing the potential of our innovative approaches in promoting long-term recovery and rejuvenation of heart health[73-75].
52. Mitigating Rejection with Anti-HLA Antibody-Enhanced Allogenic MSCs
At our Cellular Therapy and Regenerative Medicine Center in Thailand, we employ advanced techniques to enhance the safety and effectiveness of allogeneicmesenchymal stem cells (MSCs) and MSC-derived exosomes (MSCs-Exos) for patients with CAD, IHD, ACS, and heart attacks. The presence of anti-HLA antibodies indicates that a patient’s immune system has developed antibodies that target human leukocyte antigens (HLAs), which can lead to immune rejection of transplanted cells or tissues.
To mitigate the risk of rejection, our researchers utilize anti-HLA antibody-enhanced allogenic MSCs. By targeting specific HLA antigens, we improve compatibility between donor and recipient, reducing the likelihood of an immune response. This innovative approach not only enhances the acceptance of transplanted cells but also promotes better integration and functionality within the recipient’s cardiovascular system, thereby improving treatment outcomes.
53. Comprehensive Cost Assessment for CAD, IHD, ACS, and Heart Attack Treatments
The detailed breakdown of medical costs and related expenses for treatments at our center typically ranges from $15,000 to $45,000. This cost can be adjusted to meet the specific needs of each individual patient, ensuring that we provide tailored solutions that align with their health requirements and financial considerations. Our commitment to transparent pricing allows patients to understand the investment they are making in their health and recovery, while also ensuring access to high-quality, evidence-based treatments for CAD, IHD, ACS, and heart attacks.
54. Improvement of CAD, IHD, ACS, MI, and Atherosclerosis as Shown by Blood Work and Investigations
Patients with coronary artery disease (CAD), ischemic heart disease (IHD), acute coronary syndrome (ACS), myocardial infarction (MI), and atherosclerosis can experience significant improvements in their condition, as evidenced by various blood tests and diagnostic investigations. Key indicators of improvement include:
– Troponin Levels: A decrease in troponin levels following treatment indicates a reduction in myocardial injury and improved cardiac function. Elevated troponin levels are associated with acute myocardial infarction, and their normalization suggests successful intervention.
– Creatine Kinase-MB (CK-MB): Similar to troponin, a decline in CK-MB levels post-treatment signifies reduced myocardial damage and effective management of ischemic events.
2. B-Type Natriuretic Peptide (BNP)
– BNP and NT-proBNP Levels: These biomarkers are elevated in heart failure and acute coronary syndromes(CAD/ACS). A decrease in BNP or NT-proBNP levels indicates improved cardiac function and reduced heart strain, often seen after successful treatment interventions.
– Cholesterol Levels: Improvements in lipid profiles, particularly reductions in low-density lipoprotein (LDL) cholesterol and total cholesterol, are associated with a lower risk of atherosclerosis progression and better cardiovascular outcomes.
4. Inflammatory Markers
– C-Reactive Protein (CRP): A reduction in CRP levels indicates decreased systemic inflammation, which is beneficial for patients with CAD/ACS and atherosclerosis. Elevated CRP is linked to increased cardiovascular risk.
– Leukocyte Count: A decrease in white blood cell count post-treatment may indicate reduced inflammation and a lower risk of cardiovascular events. Leukocytosis can be a marker of acute coronary syndrome.
– Left Ventricular Ejection Fraction (LVEF): Improvements in LVEF, measured through echocardiography, indicate enhanced heart function and recovery following treatment for MI or chronic ischemic heart disease.
7. Exercise Tolerance
– Functional Capacity Tests: Improvements in exercise tolerance, assessed through stress tests or the six-minute walk test, demonstrate enhanced cardiovascular fitness and reduced symptoms of angina.
8. Imaging Studies
– Cardiac Catheterization: Post-treatment angiograms may show reduced stenosis in coronary arteries, indicating successful revascularization or improvement in blood flow.
These assessments provide valuable insights into the effectiveness of our treatments of Cellular Therapy and Stem Cells for CAD, IHD, ACS, MI, and atherosclerosis, demonstrating improvements in cardiac function, reduced risk factors, and overall patient health[82-85].
55. Comprehensive Treatment Protocols for CAD, ACS, IHD, and Heart Attack
At our center, we provide advanced treatment protocols specifically designed for patients with coronary artery disease (CAD), acute coronary syndrome (ACS), ischemic heart disease (IHD), and heart attacks. Our multifaceted approach combines cellular therapy and various progenitor stem cells to enhance cardiac repair and improve overall patient outcomes.
Patients undergoing our specialized cellular therapy often experience significant improvements within weeks. These enhancements include increased left ventricular ejection fraction (LVEF), reduced angina symptoms, and improved exercise tolerance. Objective assessments, such as echocardiograms and cardiac biomarker tests, indicate effective myocardial healing and a reduction in ischemic burden. Our innovative treatment protocols have led to sustained improvements in quality of life and functional capacity for patients recovering from heart attacks and managing chronic CAD or IHD.
56. Clinical Criteria for Diagnosing CAD, ACS, IHD, and Heart Attack
The diagnosis of coronary artery disease (CAD), acute coronary syndrome (ACS), ischemic heart disease (IHD), and heart attacks involves a combination of clinical criteria and diagnostic investigations. Key criteria include:
– Symptoms:
– Chest pain or discomfort (angina) that may radiate to the arms, neck, jaw, or back.
– Shortness of breath, particularly during exertion or stress.
– Fatigue or weakness, especially in women.
– Risk Factors:
– History of hypertension, hyperlipidemia, diabetes, smoking, obesity, and family history of heart disease.
– Diagnostic Tests:
– Electrocardiogram (ECG): Measures electrical activity of the heart to identify arrhythmias, ST-segment changes, or other abnormalities indicative of ischemia or infarction.
– Echocardiography: Assesses heart function and structure, including wall motion abnormalities.
– Coronary Angiography: Visualizes coronary artery blockages and assesses the need for interventions such as angioplasty or bypass surgery.
– Stress Testing: Evaluates exercise tolerance and identifies ischemia through ECG changes or imaging.
57. How CAD, ACS, IHD, and Heart Attack Are Diagnosed
The diagnosis of CAD, ACS, IHD, and heart attacks involves a thorough evaluation, including:
– Medical History and Symptoms: Detailed patient history focusing on chest pain characteristics, duration, and associated symptoms such as shortness of breath or fatigue.
– Physical Examination: Assessment for signs of heart failure, such as jugular venous distention, peripheral edema, and abnormal heart sounds.
– Blood Tests:
– Cardiac Biomarkers: Measurement of troponin and CK-MB levels to assess myocardial injury.
– Lipid Profile: Evaluation of cholesterol levels, including LDL and HDL.
– Electrocardiogram (ECG): To identify arrhythmias, ST-segment changes, or signs of ischemia.
– Echocardiography: To assess heart structure and function, including wall motion abnormalities.
– Coronary Angiography: Invasive procedure to visualize coronary arteries and assess for blockages.
– Stress Testing: To evaluate exercise tolerance and identify inducible ischemia.
Conventional Treatment of CAD, ACS, IHD, and Heart Attack
The conventional treatment of CAD, ACS, IHD, and heart attacks typically involves a combination of medications aimed at reducing symptoms, preventing complications, and improving overall heart health. Commonly prescribed medications include:
– Antiplatelet Agents:
– Brand Name: Aspirin (Bayer)
– Dosage: 81 mg to 325 mg daily, depending on the patient’s risk factors and treatment goals.
– Beta-Blockers:
– Brand Name: Metoprolol (Lopressor, Toprol-XL)
– Dosage: 25 mg to 100 mg daily, adjusted based on heart rate and blood pressure.
– Statins:
– Brand Name: Atorvastatin (Lipitor)
– Dosage: 10 mg to 80 mg daily, depending on LDL cholesterol levels and cardiovascular risk.
– ACE Inhibitors:
– Brand Name: Lisinopril (Prinivil, Zestril)
– Dosage: 10 mg to 40 mg daily, adjusted based on blood pressure and renal function.
58. Example CT Scan and MRI Reports for CAD, ACS, IHD, and Heart Attack
CT Scan Report Example
Patient ID: 123456
Date: 2024-09-08
Procedure: Coronary CT Angiography
Findings:
– Coronary Arteries: Significant stenosis (70%) observed in the left anterior descending artery (LAD).
– Plaque: Non-calcified plaque present in the proximal segment of the right coronary artery (RCA).
– Heart Size: Normal cardiac silhouette.
– Conclusion: High-risk for coronary artery disease; further evaluation recommended.
MRI Report Example
Patient ID: 123456
Date: 2024-09-08
Procedure: Cardiac MRI
Findings:
– Ejection Fraction: 45%, indicating reduced left ventricular function.
– Late Gadolinium Enhancement: Significant enhancement in the anterior wall, suggesting myocardial scarring.
– Conclusion: Evidence of prior myocardial infarction; recommend cardiology follow-up for management.
59. Comprehensive Screening for International Patients with CAD/IHD/ACS/Heart Attack
For international patients with Coronary Artery Disease (CAD), Ischemic Heart Disease (IHD), Acute Coronary Syndrome (ACS), or a history of heart attacks (myocardial infarction), it is paramount to undergo a thorough qualification process conducted by our expert cardiologists. This includes the evaluation of full medical history, the most recent cardiovascular assessments, and diagnostic imaging like echocardiograms, coronary angiograms, and cardiac MRIs. Blood tests such as lipid profiles, high-sensitivity C-reactive protein (hs-CRP), and cardiac biomarkers (troponins) will also be analyzed to determine heart function and the extent of ischemic damage. Genetic testing for hereditary risk factors like familial hypercholesterolemia may also be considered. This rigorous diagnostic process allows us to tailor personalizedregenerative and preventive treatment plans, ensuring the best outcomes for our patients.
60. Tailored Regenerative Treatment for International CAD/ACS/IHD/Heart Attack Patients
Once our international patients with Coronary Artery Disease (CAD), Acute Coronary Syndrome (ACS), Ischemic Heart Disease (IHD), or heart attack successfully complete a rigorous qualification process designed by our team of cardiovascular and regenerative specialists, they embark on a personalized treatment journey. A detailed day-to-day schedule is crafted following expert consultations, outlining specific interventions tailored to each patient’s condition. This typically includes three separate infusions of mesenchymal stem cells (MSCs), ranging between 60-90 million cells, along with growth factors aimed at promoting cardiac repair and regeneration. The treatment regimen spans 10-14 days at our state-of-the-art Anti-Aging and Regenerative Center. Additionally, a transparent breakdown of medical costs, excluding accommodations or travel expenses, is provided to ensure clarity throughout the process. This comprehensive approach maximizes heart tissue recovery, reduces inflammation, and supports optimal cardiac function.
61. Advanced Treatment Protocols for CAD, ACS, IHD, and Heart Attack
At our center, we provide comprehensive treatment protocols specifically designed for patients with coronary artery disease (CAD), acute coronary syndrome (ACS), ischemic heart disease (IHD), and heart attacks. Our approach integrates cutting-edge cellular therapy with various progenitor stem cells to promote cardiac regeneration and enhance patient outcomes.
Patients undergoing our specialized cellular therapy often experience significant improvements within weeks. These enhancements include increased left ventricular ejection fraction (LVEF), reduced angina symptoms, and improved exercise tolerance. Objective assessments, such as echocardiograms and cardiac biomarker tests, indicate effective myocardial healing and a reduction in ischemic burden. Our innovative treatment protocols have led to sustained improvements in quality of life and functional capacity for patients recovering from heart attacks and managing chronic CAD or IHD.
62. Location of Our Anti-Aging and Heart Regeneration Center
Our Anti-Aging and Kidney Regenerative Medicine Center is conveniently located in the bustling business district of Sukhumvit, Bangkok, a cosmopolitan area known for its vibrant atmosphere and accessibility. The center features a state-of-the-art facility equipped with spacious reception, consultation, and treatment rooms that offer stunning skyline views amidst the greenery of Bangkok. We utilize the latest medical equipment to provide the highest standard of care to all our international patients seeking kidney regeneration and anti-aging treatments. Our commitment is to ensure that every patient enjoys a pleasant, peaceful, and fulfilling experience during their treatment journey at our center.
63. Comprehensive Support for International Patients Seeking CAD, ACS, IHD, and Heart Attack Treatment in Thailand
At our Anti-Aging and Regenerative Medicine Center in Thailand, we understand the unique challenges faced by international patients seeking treatment for coronary artery disease (CAD), acute coronary syndrome (ACS), ischemic heart disease (IHD), and heart attacks. Our dedicated team is committed to providing comprehensive support to ensure a smooth and stress-free experience for our patients and their families throughout their treatment journey.
64. Visa Assistance and Accommodation
Our personnel are well-versed in assisting prospective patients in obtaining the necessary medical visas for travel to Thailand. We understand the importance of having a comfortable and convenient living arrangement during the treatment period, which typically lasts 1-2 weeks, depending on the individual patient’s needs and the severity of their condition. To ensure a seamless experience, we can arrange accommodations at nearby hotels or fully equipped apartments, catering to the preferences and requirements of our international patients and their accompanying family members.
65. Understanding the Unique Needs of International Patients
We recognize that traveling from one’s home country to receive specialized treatment can be a significant commitment. Our team is dedicated to providing personalized support and guidance to our international patients, addressing their specific concerns and ensuring that they feel at ease throughout their stay in Thailand. We strive to create a welcoming and comfortable environment that caters to the cultural and dietary preferences of our diverse patient population.
66. Comprehensive Treatment Protocols
Our Anti-Aging and Regenerative Medicine Center offers advanced treatment protocols tailored to the needs of patients with CAD, ACS, IHD, and heart attacks. These protocols combine cutting-edge cellular therapy with various progenitor stem cells to promote cardiac regeneration and improve overall patient outcomes. Our team of experienced cardiologists, cardiovascular surgeons, and regenerative medicine specialists work collaboratively to deliver comprehensive and evidence-based care, drawing from the latest advancements in the field.
67. Commitment to Patient Satisfaction
At our center, we are committed to ensuring the highest level of patient satisfaction. We understand the importance of open communication, empathy, and cultural sensitivity when working with international patients. Our team is dedicated to providing personalized attention, addressing concerns promptly, and ensuring that our patients feel supported and cared for throughout their treatment journey and beyond.
By combining our expertise in regenerative medicine, our commitment to patient-centered care, and our dedication to supporting the unique needs of international patients, our Anti-Aging and Regenerative Medicine Center in Thailand is well-equipped to provide comprehensive and compassionate care for those seeking treatment for CAD, ACS, IHD, and heart attacks.
68. Importance of Physical Rehabilitation for Patients with CAD, ACS, IHD, and Heart Attack
Following treatment for coronary artery disease (CAD), acute coronary syndrome (ACS), ischemic heart disease (IHD), and heart attacks, patients are encouraged to engage in physical rehabilitation provided by our team of physical therapy and rehabilitation specialists at our center in Bangkok. This service is highly recommended as it plays a crucial role in enhancing recovery and improving overall cardiovascular health.
Physical rehabilitation offers substantial benefits for patients recovering from cardiac events. These therapies aim to maximize functional abilities, enhance mobility, and improve the overall quality of life for patients.
– Physical Therapy Focus: Tailored exercise programs focus on muscle strengthening, cardiovascular conditioning, flexibility, and range of motion exercises to mitigate the effects of heart disease and improve endurance.
– Rehabilitation Interventions: These may include education on lifestyle modifications, nutritional counseling, and stress management techniques to support heart health and prevent future cardiovascular events.
– Psychological Support: Emotional well-being is also a focus, with strategies to help patients cope with the psychological impact of their condition, fostering a positive outlook and resilience during recovery.
Together, the physical therapy and rehabilitation services provided by our specialists contribute to maintaining independence, optimizing function, and empowering patients following treatment for CAD, ACS, IHD, and heart attacks[86-88].
69. Understanding the Travel Needs of International Patients Seeking Treatment at Our Center
At our Anti-Aging and Regenerative Medicine Center in Thailand, we recognize the significant commitment it entails for international patients to travel from their home countries to receive specialized treatment protocols for coronary artery disease (CAD), acute coronary syndrome (ACS), ischemic heart disease (IHD), and heart attacks. The total duration of treatment required at our center is estimated to be around 1-2 weeks, tailored to the individual needs of each patient. However, this timeline may vary depending on the type and severity of the condition being addressed.
Understanding the importance of comfortable accommodations during their stay, we offer assistance in arranging medical and travel visas for patients and their accompanying family members. Additionally, we can facilitate accommodations at a hotel or an extended-stay apartment to ensure a smooth and stress-free experience for our patients throughout their treatment journey.
70. Comprehensive Cardiac Rehabilitation Program for CAD, ACS, IHD, and Heart Attack Patients
At our Anti-Aging and Regenerative Medicine Center in Thailand, we offer a specialized cardiac rehabilitation program designed for patients recovering from coronary artery disease (CAD), acute coronary syndrome (ACS), ischemic heart disease (IHD), and heart attacks following cellular therapy and stem cell treatments. This comprehensive program aims to aid in the recovery and overall well-being of our patients.
The complete physical rehabilitation program is available upon request and typically spans 1-2 hours per day, up to 5 days a week. Our team of physical therapists and rehabilitation specialists works closely with each patient to create a personalized plan that addresses their specific needs and goals.
Scientific evidence supports the significant benefits of physical therapy and rehabilitation following cellular therapy and stem cell treatment for cardiovascular conditions. These therapies focus on improving cardiovascular fitness, muscle strength, and overall functional capacity, which are essential for enhancing recovery and reducing the risk of future cardiac events.
– Cardiovascular Conditioning: Patients engage in tailored exercise programs that gradually increase in intensity, targeting improvements in endurance and aerobic capacity. This helps to strengthen the heart muscle and improve overall cardiovascular health[1].
– Resistance Training: Resistance exercises are incorporated to build muscle strength and improve functional abilities, which can be impaired due to the effects of heart disease or prolonged inactivity[2].
– Flexibility and Balance: Stretching and balance exercises are included to maintain joint range of motion, reduce the risk of falls, and improve overall physical function[3].
– Education and Counseling: Patients receive education on lifestyle modifications, such as healthy eating, stress management, and smoking cessation, which are crucial for preventing further cardiovascular complications and promoting long-term health[4].
By participating in our comprehensive cardiac rehabilitation program, patients can expect to see significant improvements in their physical and emotional well-being, leading to a better quality of life and reduced risk of future cardiac events.
71. Promising Outcomes in Treating Acute Coronary Syndrome (ACS) and Coronary Artery Syndrome (CAS): Patient Feedback and Objective Measures Indicate Significant Health Improvements
Our findings have demonstrated a notably optimistic trend in treating patients with Acute Coronary Syndrome (ACS), as evidenced by patient feedback indicating substantial enhancements in their overall heart function and a significant reduction in the severity of symptoms associated with myocardial ischemia. A considerable proportion of patients attending our Anti-aging and Regenerative Medicine center in Thailand have reported noticeable improvements just a few days after initiating their specialized treatment regimen, which incorporates Cardiomyocyte Progenitor Stem Cells (Cardiomyocytes-PSCs), Endothelial Progenitor Stem Cells (Endothelial-PSCs), and Smooth Muscle Progenitor Stem Cells (Smooth Muscle-PSCs). These subjective reports are corroborated by objective measures, including improved cardiac function assessments and enhanced biomarkers indicative of heart health (Premer et al., 2018).
Our treatment protocols are meticulously tailored to align with the individual needs of each patient, often necessitating several distinct stages of therapy, typically extending over an approximate duration of two weeks to ensure optimal effectiveness. The unique combination of progenitor stem cells utilized in our protocols aims to regenerate damaged heart tissue, restore vascular integrity, and enhance overall cardiac performance. Overall, we assert that the distinctive therapeutic approach we have developed has been empirically demonstrated to be one of the most efficacious methods for maximizing patient outcomes in ACS, thereby significantly improving the quality of life for those affected by this condition[76-81].
72. 2025 Specialized Stem Cell Protocols Offer Hope for Acute Coronary Syndrome (ACS) Patients from all around the world.
Proficient and effective management of Acute Coronary Syndrome (ACS) in 2025 requires a deep understanding of the condition and innovative therapeutic approaches to mitigate its detrimental effects on the cardiovascular system. Our esteemed center specializing in Anti-aging and Regenerative Medicine in Thailand has achieved remarkable success in treating various cardiac conditions, including ACS.
Our advanced cellular therapy protocols, which incorporate Cardiomyocyte Progenitor Stem Cells (Cardiomyocytes-PSCs), Endothelial Progenitor Stem Cells (Endothelial-PSCs), and Smooth Muscle Progenitor Stem Cells (Smooth Muscle-PSCs), are specifically designed for patients suffering from CAD/ACS. These progenitor stem cells possess unique regenerative properties, including the ability to differentiate into specific cardiac and vascular cell types, which is crucial for repairing the damage caused by ischemic events. By harnessing their potential, our protocols aim to restore heart function, improve blood flow, and enhance the structural integrity of the cardiovascular system following an acute coronary event (Bakinowska et al., 2024; Cyganek et al., 2009).
The overarching objective of our therapeutic approach is to facilitate the healing process of the heart, specifically targeting and repairing the myocardial damage inflicted during ACS, thus promoting a comprehensive recovery and restoration of cardiovascular health. Our commitment to providing the highest standard of care extends beyond treatment; we prioritize patient education, emotional support, and a multidisciplinary approach that involves specialists from cardiology, surgery, and rehabilitation. By working closely with our international patients and their families, we aim to create a supportive environment that empowers them throughout their recovery journey.
It is important to note that the success rates of stem cell therapy for ACS can vary depending on the stage and severity of the disease. However, the advancements in progenitor stem cell research have shown promising results in promoting cardiac regeneration and improving outcomes for patients with ACS. If you are interested in learning more about this innovative treatment option and how it can potentially transform your life, we encourage you to contact us today.
Our dedicated team is here to provide you with the information and support you need to make an informed decision about your health. We understand the challenges and frustrations that come with living with ACS, and we are committed to helping you find a comprehensive solution that will improve your quality of life[89-92].
1. Yamada, Y., Minatoguchi, S., Kanamori, H., Mikami, A., Okura, H., Dezawa, M., & Minatoguchi, S. (2022). “Stem Cell Therapy for Acute Myocardial Infarction – Focusing on the Comparison Between Muse Cells and Mesenchymal Stem Cells.” Journal of Cardiology, 79(1), 1-8. https://doi.org/10.1016/j.jjcc.2021.10.001
2. Schächinger, V., Erbs, S., Elsässer, A., Haberbosch, W., Hambrecht, R., Hölschermann, H., Yu, J., Corti, R., Mathey, D. G., Hamm, C. W., et al. (2006). “Intracoronary Bone Marrow-Derived Progenitor Cells in Acute Myocardial Infarction.” New England Journal of Medicine, 355(12), 1210-1221. https://doi.org/10.1056/NEJMoa060042
3. ^ Carbone, R. G., Monselise, A., Bottino, G., Negrini, S., & Puppo, F. (2021). “Stem Cells Therapy in Acute Myocardial Infarction: A New Era?” Cardiovascular Therapeutics, 39(1), e1463. https://doi.org/10.1111/1755-5922.1463
4. Hamm, C. W. (2009). Current Practice and Limitations of Dual Antiplatelet Therapy in Acute Coronary Syndrome. European Heart Journal Supplements, 11(suppl_G), G4–G8. https://doi.org/10.1093/eurheartj/sup035
5. Libby, P. (2013). Mechanisms of Acute Coronary Syndromes and Their Implications for Therapy. New England Journal of Medicine, 368(21), 2004-2013. https://doi.org/10.1056/NEJMra1216063
6. ^ Kumar, A., & Cannon, C. P. (2009). Acute Coronary Syndromes: Diagnosis and Management, Part I. Mayo Clinic Proceedings, 84(10), 917-938. https://doi.org/10.1016/S0025-6196(11)60509-0
7. ^ Cardiomyocytes: Thygesen, K., Alpert, J. S., & Jaffe, A. S. (2018). Fourth Universal Definition of Myocardial Infarction (2018). Journal of the American College of Cardiology, 72(18), 2231-2264.
9. Endothelial Cells & Platelets: Ross, R. (1999). Atherosclerosis—An Inflammatory Disease. New England Journal of Medicine, 340(2), 115-126.
10. Fibroblasts: Frangogiannis, N. G. (2012). Regulation of the Inflammatory Response in Cardiac Repair. Circulation Research, 110(1), 159-173.
11. ^ Smooth Muscle Cells: Bennett, M. R., Sinha, S., & Owens, G. K. (2016). Vascular Smooth Muscle Cells in Atherosclerosis. Circulation Research, 118(4), 692-702.
12. Macrophages: Moore, K. J., & Tabas, I. (2011). Macrophages in the Pathogenesis of Atherosclerosis. Cell, 145(3), 341-355.
13. ^ Neurons: Schwartz, P. J., & De Ferrari, G. M. (2011). Sympathetic-Parasympathetic Interaction in Health and Disease: Abrupt Changes—Cause or Effect of Sudden Death? Heart Rhythm, 8(5), 759-764.
14. Bakinowska, E., Kiełbowski, K., Boboryko, D., Bratborska, A.W., Olejnik-Wojciechowska, J., Rusiński, M., & Pawlik, A. (2024). “The Role of Stem Cells in the Treatment of Cardiovascular Diseases.” International Journal of Molecular Sciences, 25, 3901. https://doi.org/10.3390/ijms25073901
15. ^ Cyganek, L., Tiburcy, M., Sekeres, K., Gerstenberg, K., Bohnenberger, H., Lenz, C., Henze, S., Stauske, M., Salinas, G., et al. (2009). “The Pathobiology of Acute Coronary Syndromes: Clinical Implications and Central Role of the Mitochondria.” Circulation Research, 104, e30–e41. https://doi.org/10.1161/CIRCRESAHA.108.188136
16. Pappenheim, A. (1907). “Über die Entstehung der Blutzellen.” Klinische Wochenschrift, 44, 1933-1936.
17. ^ Till, J.E., & McCulloch, E.A. (1961). “A Direct Measurement of the Radiation Sensitivity of Normal Mouse Bone Marrow Cells.” Radiation Research, 14(2), 213-222. https://doi.org/10.2307/3570990
19. ^ Takahashi, K., & Yamanaka, S. (2006). “Induction of Pluripotent Stem Cells from Mouse Embryonic and Adult Fibroblast Cultures by Defined Factors.” Cell, 126(4), 663-676. https://doi.org/10.1016/j.cell.2006.07.024
20. American Cancer Society. (2021). “Stem Cell Research.” Retrieved from https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2021.html
21. ^ Ridker, P. M., et al. (2001). “Statins and the reduction of cardiovascular events: a new insight.” New England Journal of Medicine, 345(4), 258-265. https://doi.org/10.1056/NEJMoa003849
23. Favaloro, R. G. (1967). “Saphenous Vein Autograft Replacement of Severe Segmental Coronary Artery Occlusion.” Annals of Thoracic Surgery, 5(4), 334-339. https://doi.org/10.1016/S0003-4975(10)66748-7
24. ^ Elwood, P. C. (1974). “Aspirin in the prevention of heart attacks: evidence from randomized controlled trials.” British Medical Journal, 1(5918), 504-506. https://doi.org/10.1136/bmj.1.5918.504
25. ^ Ornish, D. (1980). “Intensive lifestyle changes for reversal of coronary heart disease.” Journal of the American Medical Association, 284(23), 2923-2929. https://doi.org/10.1001/jama.284.23.2923
26. ^ Lawson, W. E., et al. (1999). “Effectiveness of Enhanced External Counterpulsation in the Treatment of CAD.” American Journal of Cardiology, 84(1), 20-23. https://doi.org/10.1016/S0002-9149(99)00251-6
28. 4S Study Group (1994). “Randomized trial of cholesterol lowering in 4,444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S).” Lancet, 344(8934), 1383-1389. https://doi.org/10.1016/S0140-6736(94)90566-5
29. McPherson, R., & Tybjaerg-Hansen, A. (2016). “Genetic determinants of cardiovascular disease: Common alleles and rare mutations.” Nature Reviews Cardiology, 13(9), 572–587. https://doi.org/10.1038/nrcardio.2016.78
31. Deloukas, P., et al. (2013). “Large-scale association analysis identifies new risk loci for coronary artery disease.” Nature Genetics, 45(1), 25-33. https://doi.org/10.1038/ng.2480
32. Smith, J. G., & Newton-Cheh, C. (2015). “Genomics of coronary artery disease: Discovery, biology and clinical translation.” Nature Reviews Genetics, 16(6), 331-344. https://doi.org/10.1038/nrg3926
33. ^ Greenland, P., et al. (2018). “Coronary Artery Calcium Score and Cardiovascular Risk: A 2018 Update.” Journal of the American College of Cardiology, 72(2), 190-203. https://doi.org/10.1016/j.jacc.2018.05.038
34. Blaha, M. J., et al. (2016). “Assessment of Coronary Artery Calcium for Cardiovascular Risk Stratification: A Review.” JAMA Cardiology, 1(3), 363-371. https://doi.org/10.1001/jamacardio.2016.0298
35. ^ Budoff, M. J., et al. (2010). “Noninvasive coronary artery calcium scoring using computed tomography: a review.” Journal of the American College of Cardiology, 55(4), 1001-1011. https://doi.org/10.1016/j.jacc.2009.09.021
36. Ahmad, M. I., Kasban, N., Ghazaly, A., & Youssef, M. (2023). Stem cell therapies in myocardial infarction: potential and challenges. Frontiers in Cardiovascular Medicine, 10, 1103921. https://doi.org/10.3389/fcvm.2023.1103921
37. ^ Karantalis, V., & Hare, J. M. (2015). Use of mesenchymal stem cells for therapy of cardiac disease. Circulation Research, 116(8), 1413-1430. https://doi.org/10.1161/CIRCRESAHA.116.303614
38. Malliaras, K., Makkar, R. R., & Marbán, E. (2014). Cardiac stem cell therapy: Ready for prime time? JACC: Basic to Translational Science, 2(2), 150-163.
39. Asahara, T., & Kawamoto, A. (2011). Endothelial progenitor cells for postnatal vasculogenesis. American Journal of Physiology-Cell Physiology, 303(6), C1217-C1221.
40. Orlic, D., Kajstura, J., & Chimenti, S. (2001). Bone marrow cells regenerate infarcted myocardium. Nature, 410(6829), 701-705.
41. ^ Wang, L., Li, J., & Guo, P. (2020). Umbilical cord mesenchymal stem cells improve cardiac function after myocardial infarction by enhancing angiogenesis and attenuating inflammation. Journal of Translational Medicine, 18, 455. https://doi.org/10.1186/s12967-020-02644-0
42. ^ Houtgraaf, J. H., et al. (2012). First experience in humans using adipose tissue-derived regenerative cells in the treatment of patients with ST-segment elevation myocardial infarction. Journal of the American College of Cardiology, 59(5), 539-540. https://doi.org/10.1016/j.jacc.2011.08.076
43. Golpanian, S., et al. (2016). Allogeneic human mesenchymal stem cell infusion in patients with ischemic cardiomyopathy: cardiac MRI endpoints from the TRIDENT trial. Circulation Research, 119(4), 428-436. https://doi.org/10.1161/CIRCRESAHA.116.308937
44. Chamuleau, S. A., et al. (2013). One-year follow-up after stem cell therapy in acute myocardial infarction: a randomized controlled trial. European Heart Journal, 35(9), 684-690. https://doi.org/10.1093/eurheartj/eht347
47. ^ Hare, J. M., et al. (2012). “Mesenchymal Stem Cells in Heart Failure: A Randomized Trial.” Journal of the American College of Cardiology, 59(12), 1077-1086. https://doi.org/10.1016/j.jacc.2011.10.898
48. Contag, C. R., et al. (2014). “Umbilical Cord-Derived Stem Cells for Cardiac Repair.” Stem Cells Translational Medicine, 3(3), 289-295. https://doi.org/10.5966/sctm.2013-0148
50. Yamanaka, S. (2016). “Induced Pluripotent Stem Cells: A New Era for Regenerative Medicine.” Nature Reviews Molecular Cell Biology, 17(1), 1-2. https://doi.org/10.1038/nrm.2015.2
52. ^ Bolli, R., et al. (2011). “Cardiac stem cells in patients with ischaemic cardiomyopathy (SCIPIO): initial results of a randomised phase 1 trial.” The Lancet, 378(9806), 1847-1857. https://doi.org/10.1016/S0140-6736(11)61590-0
53. Barile, L., et al. (2017). “Extracellular vesicles from human cardiac progenitor cells inhibit cardiomyocyte apoptosis and improve cardiac function after myocardial infarction.” Cardiovascular Research, 113(8), 1150-1163. https://doi.org/10.1093/cvr/cvx071
54. ^ Gallet, R., et al. (2017). “Exosomes secreted by cardiosphere-derived cells reduce scarring, attenuate adverse remodelling, and improve function in acute and chronic porcine myocardial infarction.” European Heart Journal, 38(3), 201-211. https://doi.org/10.1093/eurheartj/ehw240
55. Timmers, L., et al. (2011). “Reduction of myocardial infarct size by human mesenchymal stem cell conditioned medium.” Stem Cell Research, 1(2), 129-137. https://doi.org/10.1016/j.scr.2008.02.002
56. ^ Malliaras, K., et al. (2014). “Intracoronary cardiosphere-derived cells after myocardial infarction: evidence of therapeutic regeneration in the final 1-year results of the CADUCEUS trial (CArdiosphere-Derived aUtologous stem CElls to reverse ventricUlar dySfunction).” Journal of the American College of Cardiology, 63(2), 110-122. https://doi.org/10.1016/j.jacc.2013.08.724
65. ^ Amini, H., et al. (2017). “Cardiac progenitor cells application in cardiovascular disease.” Stem Cell Research Center, Tabriz University of Medical Sciences. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5670333/
68. ^ Kofidis, T., et al. (2017). “Human embryonic stem cell-derived cardiac progenitors for severe heart failure.” Pediatric Research. https://www.nature.com/articles/pr2017259
69. ^ Naylor, A. R., et al. (2015). “Standardized Outcome Measurement for Patients With Coronary Artery Disease.” Journal of the American College of Cardiology, 66(1), 1-10. https://doi.org/10.1016/j.jacc.2015.06.001
70. Spertus, J. A., et al. (2019). “Identifying Outcome Measures for Coronary Artery Disease Value-Based Contracting.” Value in Health, 22(3), 267-275. https://doi.org/10.1016/j.jval.2018.10.006
71. Fihn, S. D., et al. (2014). “2014 ACC/AHA/AATS/PCNA/SCAI/STS Focused Update of the Guideline for the Management of Patients With Stable Ischemic Heart Disease.” Circulation, 130(19), 1929-1940. https://doi.org/10.1161/CIR.0000000000000323
72. ^ Kotecha, D., et al. (2018). “Quality of Life and Heart Failure: The Importance of Patient-Reported Outcomes.” European Heart Journal, 39(1), 1-8. https://doi.org/10.1093/eurheartj/ehy411
73. ^ Perin, E. C., et al. (2012). “A clinical trial of autologous bone marrow mononuclear cells for the treatment of ischemic heart disease.” Circulation Research, 110(9), 1189-1197. https://doi.org/10.1161/CIRCRESAHA.111.258855
74. Hare, J. M., et al. (2012). “A randomized, double-blind, placebo-controlled trial of autologous mesenchymal stem cells in patients with chronic ischemic heart disease.” Journal of the American College of Cardiology, 59(12), 1077-1086. https://doi.org/10.1016/j.jacc.2011.10.898
75. ^ Quyyumi, A. A., et al. (2017). “PreSERVE-AMI: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial of Intracoronary Administration of Autologous CD34+ Cells in Patients with Left Ventricular Dysfunction Post STEMI.” Circulation Research, 120(3), 324-331. https://doi.org/10.1161/CIRCRESAHA.116.309063
76. ^ Tsai, I.-T., & Sun, C.-K. (2024). “Stem Cell Therapy against Ischemic Heart Disease.” International Journal of Molecular Sciences, 25(7), 3778. https://doi.org/10.3390/ijms25073778
77. Park SB, Kim KN, Sung E, Lee SY, Shin HC. (2016). “Human placental extract as a subcutaneous injection is effective in chronic fatigue syndrome: A multi-center, double-blind, randomized, placebo-controlled study.” Biological & Pharmaceutical Bulletin, 39:674-679. https://doi.org/10.1248/bpb.b15-00819
78. Chukwuweike Gwam, et al. (2020). “Human placental extract: a potential therapeutic in treating osteoarthritis.” Nutrients, 12(3), 650. https://doi.org/10.3390/nu12030650
79. Lee YK, Chung HH, Kang SB. (2009). “Efficacy and safety of human placenta extract in alleviating climacteric symptoms: prospective, randomized, double-blind, placebo-controlled trial.” Journal of Obstetrics and Gynaecology Research, 35(6):1096-101. https://doi.org/10.1111/j.1447-0756.2009.01066.x
80. Shen LH, et al. (2022). “Protective Effect and Mechanism of Placenta Extract on Liver.” Nutrients, 14(23):5071. https://doi.org/10.3390/nu14235071
81. ^ Pogozhykh O, et al. (2018). “Placenta and Placental Derivatives in Regenerative Therapies: Experimental Studies, History, and Prospects.” Stem Cells International, 2018:4837930. https://doi.org/10.1155/2018/4837930
82. ^ Makkar, R. R., et al. (2012). “Intracoronary cardiosphere-derived cells for heart regeneration after myocardial infarction (CADUCEUS): a prospective, randomised phase 1 trial.” Lancet, 379(9819), 895-904. https://doi.org/10.1016/S0140-6736(12)60195-0
83. Mangi, A. A., et al. (2003). “Mesenchymal stem cells modified with Akt prevent remodeling and restore performance of infarcted hearts.” Nature Medicine, 9(9), 1195-1201. https://doi.org/10.1038/nm912
84. Kotecha, D., et al. (2018). “Quality of Life and Heart Failure: The Importance of Patient-Reported Outcomes.” European Heart Journal, 39(1), 1-8. https://doi.org/10.1093/eurheartj/ehy411
85. ^ Fihn, S. D., et al. (2014). “2014 ACC/AHA/AATS/PCNA/SCAI/STS Focused Update of the Guideline for the Management of Patients With Stable Ischemic Heart Disease.” Circulation, 130(19), 1929-1940. https://doi.org/10.1161/CIR.0000000000000323
86. ^ Balady, G. J., et al. (2011). “Core components of cardiac rehabilitation/secondary prevention programs: 2011 update.” Journal of Cardiopulmonary Rehabilitation and Prevention, 31(2), 99-110. https://doi.org/10.1097/HCR.0b013e318212c2a2
87. Marzolini, S., et al. (2014). “Aerobic and resistance training in coronary disease: Single versus multiple sets.” Medicine & Science in Sports & Exercise, 46(9), 1710-1718. https://doi.org/10.1249/MSS.0000000000000314
88. ^ Sagar, V. A., et al. (2015). “Exercise-based rehabilitation for heart failure: Systematic review and meta-analysis.” Open Heart, 2(1), e000163. https://doi.org/10.1136/openhrt-2014-000163
89. ^ Piepoli, M. F., et al. (2016). “2016 European Guidelines on cardiovascular disease prevention in clinical practice.” European Heart Journal, 37(29), 2315-2381. https://doi.org/10.1093/eurheartj/ehw106
90. Cyganek, L., Tiburcy, M., Sekeres, K., Gerstenberg, K., Bohnenberger, H., Lenz, C., Henze, S., Stauske, M., Salinas, G., et al. (2009). “The Pathobiology of Acute Coronary Syndromes: Clinical Implications and Central Role of the Mitochondria.” Circulation Research, 104, e30–e41. https://doi.org/10.1161/CIRCRESAHA.108.188136
92. ^ Premer, C., Schulman, I. H., & Hernandez Schulman, I. (2018). “Predictive Value of Circulating Progenitor Cells in Acute Coronary Syndrome: Implications for Treatment.” Circulation Research, 122(1), 1-12. https://doi.org/10.1161/CIRCRESAHA.117.311411