At Dr. StemCellsThailand, we are dedicated to advancing the field of regenerative medicine through innovative cellular therapies and stem cell treatments. With over 20 years of experience, our expert team is committed to providing personalized care to patients from around the world, helping them achieve optimal health and vitality. We take pride in our ongoing research and development efforts, ensuring that our patients benefit from the latest advancements in stem cell technology. Our satisfied patients, who come from diverse backgrounds, testify to the transformative impact of our therapies on their lives, and we are here to support you on your journey to wellness.
Cellular Therapy and Stem Cells for Parkinson’s Disease
1. Cellular Therapy and Stem Cells for Parkinson’s Disease : Unlocking the Future of Parkinson’s Disease
Cellular Therapy and Stem Cells for Parkinson’s Disease represent a groundbreaking advancement in the quest to treat this debilitating neurodegenerative disorder. By harnessing the regenerative potential of stem cells, researchers aim to replace the damaged dopamine-producing neurons that are progressively lost in individuals with Parkinson’s. This innovative approach not only seeks to alleviate the debilitating motor symptoms associated with the disease but also addresses the underlying mechanisms of neuronal degeneration, offering hope for improved quality of life and potentially slowing disease progression.
Parkinson’s Disease stands as the second most prevalent neurodegenerative disorder worldwide, trailing only Alzheimer’s Disease. With an aging global population, the incidence of Parkinson’s is expected to rise significantly in the coming years. Studies project that an increasing number of aging individuals will be diagnosed with Parkinson’s Disease, highlighting the pressing need for effective treatments and interventions to mitigate its impact on individuals and healthcare systems alike.
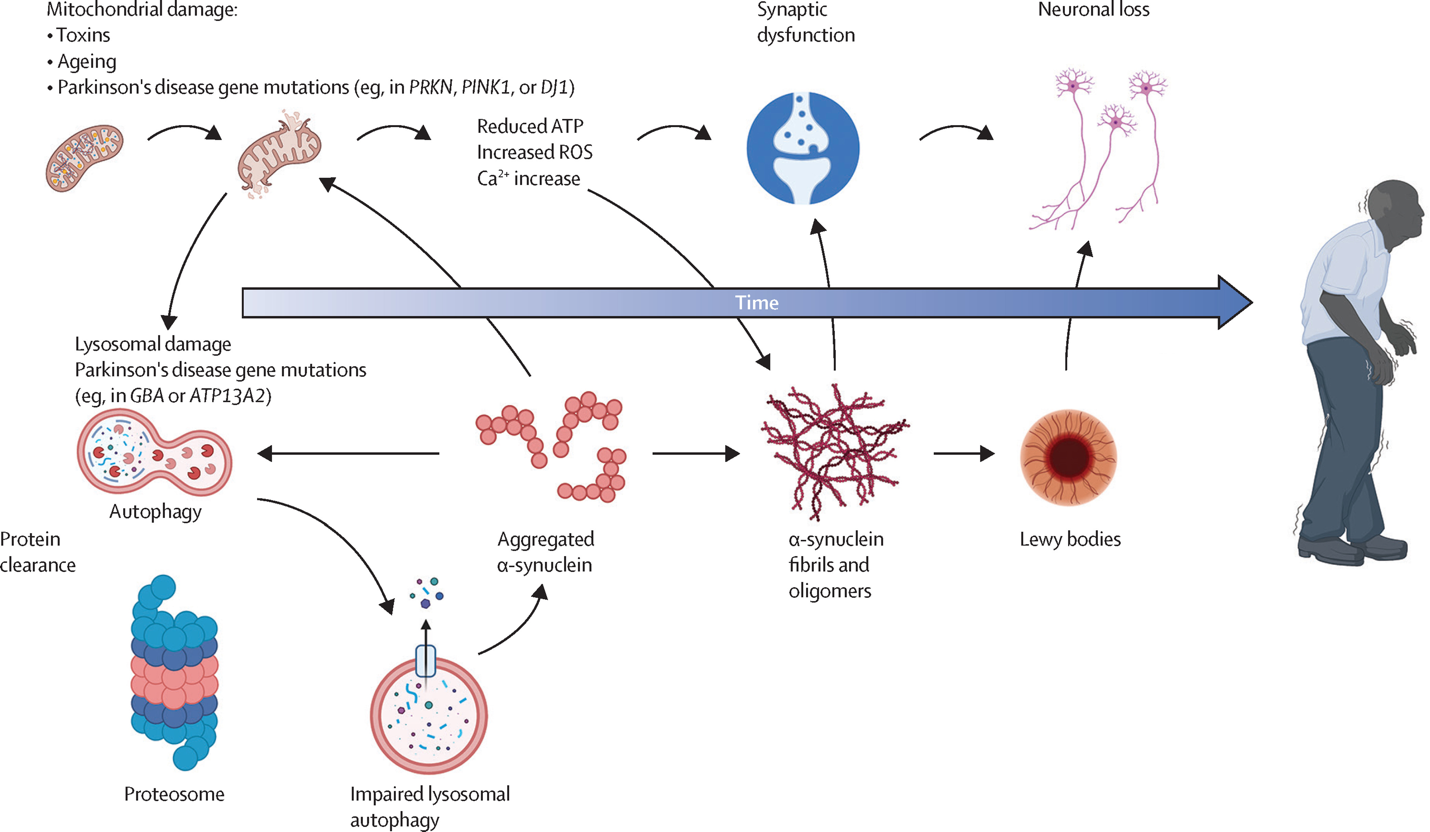
The exact cause of Parkinson’s disease remains unknown, but researchers believe it is likely a combination of genetic and environmental factors [1][3]. In Parkinson’s disease, nerve cells in the substantia nigra, a part of the brain that controls movement, become impaired or die [1][3]. These nerve cells normally produce an important brain chemical called dopamine. When dopamine levels decrease, it leads to the movement problems associated with Parkinson’s disease [1][3]. Some cases of Parkinson’s appear to be hereditary, with specific genetic mutations playing a role [2][3]. Environmental factors such as exposure to toxins or pesticides may also contribute to the development of Parkinson’s in people with certain genetic makeups [2][4]. However, the majority of Parkinson’s cases are idiopathic, meaning the cause is unknown [3].
Parkinson’s Disease (PD) stands as a formidable challenge in modern medicine, characterized by the progressive loss of dopamine-producing neurons in the brain, leading to debilitating motor and cognitive impairments. However, a ray of hope emerges through the revolutionary potential of Cellular Therapy and Stem Cells for Parkinson’s Disease. In a landmark breakthrough in 2011, a research group from the Memorial Sloan Kettering Cancer Center in New York achieved a monumental milestone by successfully producing fully functioning dopamine neurons from Cellular Therapy and Stem Cells for Parkinson’s Disease treatment. This pivotal advancement signifies a transformative leap in regenerative medicine, offering unprecedented prospects for disease modification and symptom alleviation in Parkinson’s patients.[1-8]
2. Challenges of Conventional Treatment for Parkinson’s Disease
Conventional treatment for Parkinson’s disease presents several significant challenges that can hinder effective management of the condition. One of the primary issues is the limited efficacy of current medications, such as levodopa, which primarily address motor symptoms but do not slow disease progression or effectively manage non-motor symptoms like cognitive decline, depression, and autonomic dysfunction. Additionally, as the disease progresses, patients often experience fluctuations in medication response, leading to on-off phenomena where symptoms can suddenly worsen despite ongoing treatment. Furthermore, the blood-brain barrier poses a significant obstacle for drug delivery, limiting the effectiveness of many therapeutic agents. Side effects from medications, including dyskinesia and other involuntary movements, can also complicate treatment regimens. These challenges highlight the need for a more holistic and individualized approach to Parkinson’s disease management, incorporating both pharmacological and non-pharmacological strategies to improve patient outcomes and quality of life[9].
3. Comparing Conventional Treatment for Parkinson’s Disease with Innovative Cellular Therapy and Stem Cells for Parkinson’s Disease
Conventional treatment for Parkinson’s disease primarily involves medications like levodopa and dopamine agonists, which aim to manage symptoms by compensating for the brain’s reduced dopamine production. While effective in the short term, these treatments often lead to diminishing returns and side effects over time. In contrast, innovative treatments such as Cellular Therapy and Stem Cells for Parkinson’s Disease to target the disease at its source by attempting to regenerate or replace damaged neurons, offering the potential for more sustainable and transformative outcomes. These advanced therapies of Cellular Therapy and Stem Cells for Parkinson’s Disease hold promise for not only managing symptoms but also slowing disease progression, marking a significant shift in the treatment paradigm[10].
4. Early Intervention for Parkinson’s Disease: Maximizing Treatment Benefits and Improving Outcomes
Our team of neurologists and regenerative specialists strongly advocates for patients with Parkinson’s disease to initiate our qualification process early and join our innovative treatment protocols of Cellular Therapy and Stem Cells for Parkinson’s Disease at DrStemCellsThailand‘s Anti-Aging and Regenerative Medicine Center of Thailand as soon as possible. Scientific evidence indicates that early intervention can lead to significantly improved treatment outcomes, as the progression of Parkinson’s often results in substantial neurophysiological damage and the onset of debilitating symptoms. By starting treatment early, before extensive neuronal loss occurs, our specialized protocols of Cellular Therapy and Stem Cells for Parkinson’s Disease have a greater opportunity to effectively address the underlying pathology of Parkinson’s disease, promote neuroprotection, and alleviate both motor and non-motor symptoms. This proactive approach aims to mitigate the long-term consequences of the disease, enhance functional outcomes, and optimize the overall quality of life for patients undergoing treatment. Studies have shown that early therapeutic intervention not only reduces the severity of symptoms but may also slow disease progression, ultimately leading to a better prognosis and reduced healthcare costs associated with advanced stages of the disease[11].
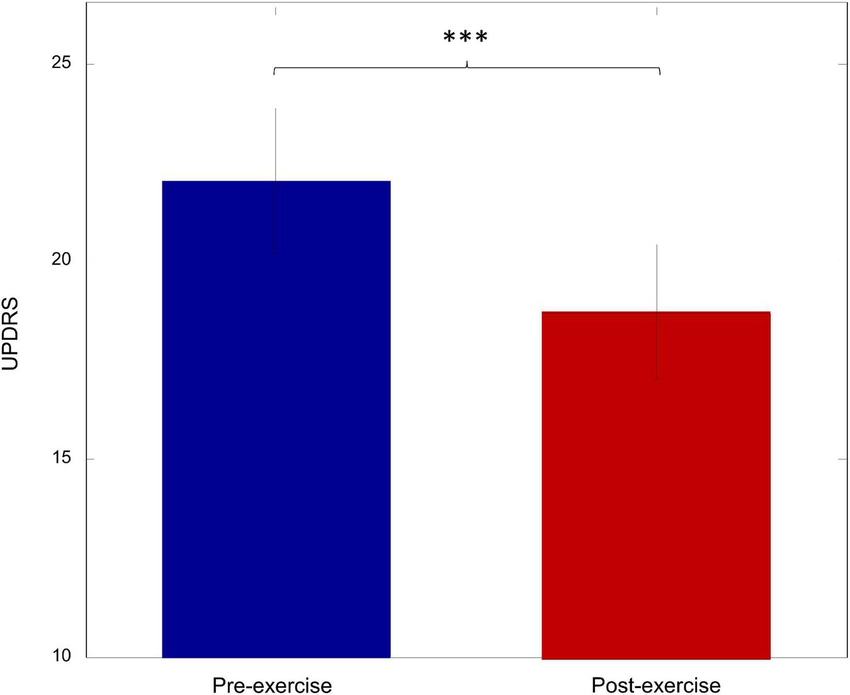
Pre and Post Treatment Outcomes of Our International Patient with Parkinson’s Disease After our special treatment protocols of Cellular Therapy and Stem Cells for Parkinson’s Disease : approximately 10-20% improvement in UPDRS score.
5. 2024 Specialized Protocols of Cellular Therapy and Stem Cells for Parkinson’s Disease Offer Hope for Patients From All Around the World
Our specialized regenerative protocols of Cellular Therapy and Stem Cells for Parkinson’s Disease in 2025 incorporate innovative approaches using stem cell therapy to address the progressive loss of dopamine-producing neurons in the brain. These protocols aim to restore critical dopamine levels, which are essential for regulating movement and coordination. By utilizing our advanced Cellular Therapy and Stem Cells for Parkinson’s Disease, we can potentially replace damaged neurons and promote neuroprotection, addressing the underlying pathology of Parkinson’s disease.
Research and clinical trials have shown that Cellular Therapy and Stem Cells for Parkinson’s Disease can improve motor function and reduce symptoms such as tremors, rigidity, and bradykinesia, improving UPDRS scores. Our protocols are designed to provide a tailored approach, customizing treatment based on the individual needs of each patient. Following the stem cell infusion, patients are encouraged to participate in a comprehensive rehabilitation program to enhance recovery and functional outcomes.
At our center, we are committed to delivering the highest standard of care, which includes not only innovative treatments but also a multidisciplinary approach that encompasses education, emotional support, and collaboration among specialists. By fostering a supportive environment, we empower our patients and their families throughout their journey, aiming to significantly improve their quality of life and overall well-being[12-15].
6. Celebrities with Parkinson’s Disease Benefiting from Conventional Treatment Alongside Cellular Therapy and Stem Cells for Parkinson’s Disease
1. Muhammad Ali:
– Lifespan: January 17, 1942 – June 3, 2016
– Diagnosis: Parkinson’s Disease diagnosed in the mid-1980s.
– Special Treatment: Ali underwent various conventional treatments for Parkinson’s Disease, including medications and physical therapy.
2. Michael J. Fox:
– Lifespan: June 9, 1961 – Present
– Diagnosis: Parkinson’s Disease diagnosed in 1991 at age 29.
– Special Treatment: Fox has been an advocate for Parkinson’s Disease research and has established the Michael J. Fox Foundation, which funds research into finding a cure for the disease. He has also undergone deep brain stimulation surgery and participated in clinical trials, including those involving Cellular Therapy and Stem Cells for Parkinson’s Disease.
3. Robin Williams:
– Lifespan: July 21, 1951 – August 11, 2014
– Diagnosis: Parkinson’s Disease diagnosed in 2013, shortly before his death.
– Special Treatment: N/A
4. Johnny Cash:
– Lifespan: February 26, 1932 – September 12, 2003
– Diagnosis: Parkinson’s Disease diagnosed in 1997.
– Special Treatment: N/A
5. Linda Ronstadt:
– Lifespan: July 15, 1946 – Present
– Diagnosis: Parkinson’s Disease diagnosed in 2013.
– Special Treatment: Ronstadt has spoken about her use of medical marijuana to alleviate symptoms of Parkinson’s Disease.
6. Maurice White (Founder of Earth, Wind & Fire):
– Lifespan: December 19, 1941 – February 4, 2016
– Diagnosis: Parkinson’s Disease diagnosed in the late 1980s.
– Special Treatment: N/A
7. Janet Reno (Former U.S. Attorney General):
– Lifespan: July 21, 1938 – November 7, 2016
– Diagnosis: Parkinson’s Disease diagnosed in 1995.
– Special Treatment: Reno underwent deep brain stimulation surgery to manage her Parkinson’s symptoms.
8. Billy Connolly:
– Lifespan: November 24, 1942 – Present
– Diagnosis: Parkinson’s Disease diagnosed in 2013.
– Special Treatment: Connolly has undergone treatment with cannabis oil to manage his symptoms.
9. Alan Alda:
– Lifespan: January 28, 1936 – Present
– Diagnosis: Parkinson’s Disease diagnosed in 2015.
– Special Treatment: Alda has spoken about his use of boxing exercises and meditation to help manage his Parkinson’s symptoms.
10. Neil Diamond:
– Lifespan: January 24, 1941 – Present
– Diagnosis: Parkinson’s Disease diagnosed in 2018.
– Special Treatment: N/A
While some famous individuals have undergone Cellular Therapy and Stem Cells for Parkinson’s Disease, this fact is not widely recognized due to concerns about their own privacy.
7. Many significant milestones in Parkinson’s Disease, Cellular Therapy, and Dopaminergic Stem Cell research globally are:
1987: Lund University in Sweden conducts the first clinical trial transplanting Embryonic/ fetal dopamine-producing cells into the brains of Parkinson’s patients, marking the first attempt at Cellular Therapy and Stem Cells for Parkinson’s Disease.
2004: The establishment of our Anti-Aging and Regenerative Medicine Center of Thailand was initiated by Professor Doctor K, driven by the vision and objective of addressing neurodegenerative conditions such as Parkinson’s Disease, ADHD, ALS, Cerebral Palsy (CP) etc. through cutting-edge Research on Cellular Therapy and Stem Cells for Parkinson’s Disease available at that time.
2011: Memorial Sloan Kettering Cancer Center in New York achieves the successful production of fully functioning dopamine neurons from stem cells for Parkinson’s Disease treatment.
2015: Kyoto University in Japan conducts the first clinical trial testing the safety and efficacy of dopaminergic stem cell transplantation in Parkinson’s patients.
2018: University of California, San Francisco, makes a breakthrough in reprogramming skin cells into dopaminergic neurons for potential transplantation in Parkinson’s therapy.
2020: University College London develops advancements in the development of personalized Cellular Therapy and Stem Cells for Parkinson’s Disease’s patients.
2022: Harvard Medical School conducts promising clinical trials demonstrating the efficacy of Cellular Therapy and Stem Cells for Parkinson’s Disease in halting or reversing neurodegeneration in the disease itself[16-22].
8. Other milestones reflect the remarkable progress and ongoing efforts in understanding, diagnosing, and treating Parkinson’s Disease globally.
1. Discovery of Levodopa’s therapeutic effects in Parkinson’s Disease by Dr. Oleh Hornykiewicz in 1960.
2. Development of deep brain stimulation (DBS) as a treatment for Parkinson’s Disease by Dr. Alim Louis Benabid and Dr. Mahlon R. DeLong in the 1980s.
3. Pioneering work on induced pluripotent stem cells (iPSCs) by Dr. Shinya Yamanaka in 2006, which opened avenues for research on Cellular Therapy and Stem Cells for Parkinson’s Disease.
4. The TRANSEURO clinical trial, led by Dr. Roger Barker and Dr. Anders Bjorklund, demonstrating the potential of fetal dopaminergic cell transplantation in Parkinson’s Disease treatment, starting in 2015.
5. Advancements in gene therapy approaches for Parkinson’s Disease, including the GDNF (Glial Cell Line-Derived Neurotrophic Factor) gene therapy trial led by Dr. Steven Gill in 2012.
6. Development of innovative disease-modifying therapies targeting alpha-synuclein, such as immunotherapy, led by Dr. Patrik Brundin and Dr. Deniz Kirik in recent years.
7. Identification of novel biomarkers for early detection, diagnosis and monitoring of Parkinson’s Disease progression, led by researchers like Dr. Thomas Gasser and Dr. Andrew Singleton in the 21st century[23-29].
9. Comprehensive List of Parkinson’s Disease Treatments with Conventional Approaches
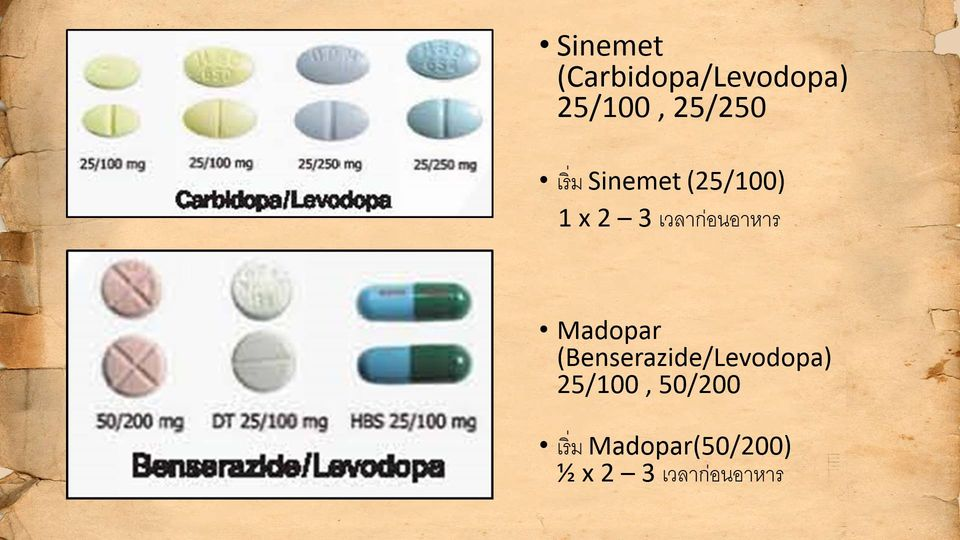
– Levodopa/Carbidopa (1960s)
– Researcher: Dr. George Cotzias
– University: Rockefeller University
– Details: Levodopa, often combined with carbidopa, remains the gold standard for treating Parkinson’s. It helps replenish dopamine levels in the brain, improving motor function.
– Dopamine Agonists (1970s)
– Researcher: Various, including Dr. Andrew Lees
– University: Multiple, including University College London
– Details: Drugs like bromocriptine, pramipexole, and ropinirole mimic dopamine, offering an alternative to levodopa and often used in early-stage Parkinson’s.
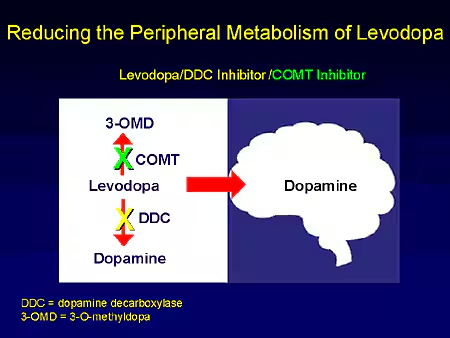
– Details: COMT inhibitors like entacapone are used alongside levodopa to block its breakdown, enhancing and prolonging its effects.
– Anticholinergics (1950s)
– Researcher: Dr. Paul A. Shannon
– University: University of Pennsylvania
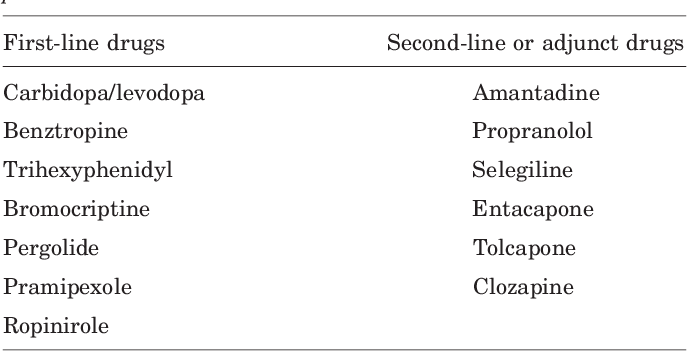
– Details: These medications, including benztropine and trihexyphenidyl, were among the first treatments for Parkinson’s, used primarily for tremor control.
– Amantadine (1970s)
– Researcher: Dr. Roger Duvoisin
– University: University of Rochester
– Details: Originally an antiviral, amantadine was found to have beneficial effects in reducing tremor and dyskinesia in Parkinson’s patients.
– Deep Brain Stimulation (DBS) (1987)
– Researcher: Dr. Alim Louis Benabid
– University: Joseph Fourier University, France
– Details: DBS involves implanting electrodes in specific brain areas to reduce motor symptoms by modulating brain activity, especially in patients not responding well to medication.
– Focused Ultrasound (2016)
Researcher: Various researchers
Institution: Multiple institutions
This non-invasive procedure uses ultrasound waves to create lesions in targeted brain areas, helping to alleviate tremors and improve motor function.
– Physical Therapy (Ongoing)
Researcher: Various researchers
Institution: Various rehabilitation centers
Physical therapy is critical for improving mobility, balance, and overall physical function, helping patients maintain independence and quality of life
– Occupational Therapy (Ongoing)
Researcher: Various researchers
Institution: Various rehabilitation centers
Occupational therapy focuses on enhancing daily living skills and adapting environments to support patients’ functional abilities.
– Speech Therapy (Ongoing)
Researcher: Various researchers
Institution: Various rehabilitation centers
Speech therapy addresses communication difficulties and swallowing issues, which are common in Parkinson’s patients.
– Complementary Therapies (Ongoing)
Researcher: Various researchers
Institution: Various institutions
These treatment options reflect a multifaceted approach to managing Parkinson’s disease, combining pharmacological and non-pharmacological strategies to enhance patient outcomes and quality of life[30].
Approaches such as acupuncture, yoga, and nutritional counseling are being explored for their potential benefits in managing Parkinson’s symptoms and improving overall well-being.
10. The Complex Interplay of Genetics and Environmental Factors in Parkinson’s Disease Development
Parkinson’s disease (PD) arises from a multifaceted interaction between genetic predispositions and environmental exposures. While about 10-15% of PD cases are linked to specific genetic mutations, such as those in the SNCA, LRRK2, PARK2, and GBA genes, the majority of cases are considered sporadic, influenced by a combination of genetic susceptibility and environmental factors.
Genetically, mutations in the SNCA gene, which encodes the protein alpha-synuclein, lead to its abnormal aggregation, forming Lewy bodies, a hallmark of PD. Similarly, mutations in the LRRK2 gene are among the most common genetic causes of PD, especially in certain populations. These mutations disrupt cellular pathways, leading to neuronal damage and loss of dopamine-producing neurons in the brain‘s substantia nigra region.
Environmental factors also play a crucial role in PD development. Long-term exposure to pesticides, such as paraquat and rotenone, has been strongly associated with an increased risk of PD. These chemicals induce oxidative stress and mitochondrial dysfunction in neurons, which are critical mechanisms in the disease’s progression. Additionally, rural living, well water consumption, and exposure to heavy metals have been implicated as risk factors.
Some environmental factors may offer protection. For instance, regular physical activity and caffeine consumption have been linked to a lower risk of developing PD, potentially due to their neuroprotective effects[31].
The interplay between genetics and the environment is complex and dynamic. For example, individuals with a genetic predisposition to PD may be more susceptible to environmental toxins, or environmental factors may trigger the onset of the disease in genetically predisposed individuals. Ongoing research aims to unravel these interactions further, with the goal of identifying at-risk populations and developing targeted preventive strategies.
11. Preventing Parkinson’s Disease Through Early Detection, Diagnosis, and Prompt Treatment
Preventing Parkinson’s Disease requires a proactive approach, beginning with early detection and accurate diagnosis, followed by prompt treatment using advanced therapeutic strategies. At our Anti-Aging and Regenerative Medicine Center of Thailand, we emphasize the importance of early intervention to halt the progression of Parkinson’s Disease. Our specialized treatment protocols combine cellular therapy with the use of various neuroprogenitor stem cells, including Dopaminergic Progenitor Stem Cells (DPSC), GABAergic Progenitor Stem Cells (GABA-PSC), Cholinergic Progenitor Stem Cells (C-PSC), Astrocytic Progenitor Stem Cells (A-PSC), Microglial Progenitor Stem Cells (M-PSC), and Oligodendrocyte Progenitor Stem Cells (OPC). These cells work synergistically to replace lost neurons, protect against further neurodegeneration, and modulate the brain’s microenvironment, thereby optimizing neurological function and potentially preventing the onset or worsening of Parkinson’s Disease. Early and comprehensive treatment through these protocols can significantly improve patient outcomes and quality of life[32].
12. Recommended Timeframe for Initiating Neuroregenerative Treatment of Cellular Therapy and Stem Cells for Parkinson’s Disease
The timing of initiating our specialized Neuroregenerative Treatment Protocols for Parkinson’s Disease is crucial for achieving the best outcomes. Our team of Neurologists and Regenerative Specialists recommends beginning Cellular Therapy and the administration of various neuroprogenitor stem cells—such as Dopaminergic Progenitor Stem Cells (DPSC), GABAergic Progenitor Stem Cells (GABA-PSC), Cholinergic Progenitor Stem Cells (C-PSC), Astrocytic Progenitor Stem Cells (A-PSC), Microglial Progenitor Stem Cells (M-PSC), and Oligodendrocyte Progenitor Stem Cells (OPC)—as early as possible following the initial onset of Parkinson’s Disease symptoms. Ideally, treatment should commence within a few weeks of diagnosis to maximize the regenerative potential and neuroprotective effects of the therapy.
Drawing on decades of experience in neuroregenerative medicine, our specialists agree that early intervention is key. Administering these cell-based therapies during the early stages of Parkinson’s Disease helps promote neuronal repair, reduce neuroinflammation, and restore the balance of neurotransmitters in the brain. This approach has been shown to significantly improve motor function, cognitive abilities, and overall quality of life for our patients. By acting promptly, we aim to slow disease progression and optimize long-term neurological outcomes.
13. The Sooner Parkinson’s Disease Patients Receive Our Cellular Therapy and Stem Cells for Parkinson’s Disease, the Better the Outcomes
Our team of Neurologists and Regenerative Specialists strongly emphasizes that early intervention is crucial for Parkinson’s Disease patients. The earlier patients begin our specialized Cellular Therapy and Neuroprogenitor Stem Cell treatments—such as Dopaminergic Progenitor Stem Cells (DPSC) and other key progenitor cells—the better their outcomes tend to be. Early treatment helps to slow disease progression, enhance motor function, and improve overall quality of life. Our extensive clinical trials and research indicate that initiating therapy as soon as possible after the onset of symptoms significantly boosts the effectiveness of these advanced treatments[33-35].
14. Prompt Qualification and Early Treatment of our Cellular Therapy and Stem Cells for Parkinson’s Disease: Key to Optimal Outcomes
Our team consistently stresses the importance of patients qualifying for our specialized brain and spinal cord regenerative treatment protocols as soon as possible following a Parkinson’s Disease diagnosis. We have observed that patients who began receiving our neural cell-based therapy within 3-4 weeks of their diagnosis experienced the most favorable outcomes. Early intervention allows us to target the disease before significant neurodegeneration occurs, which is critical for achieving the best possible recovery and long-term neurological health. By acting swiftly, we maximize the therapeutic potential of our treatments of Cellular Therapy and Stem Cells for Parkinson’s Disease , leading to improved motor skills, cognitive function, and overall well-being for our patients.
Each variety of stem cell presents distinct characteristics and potential therapeutic pathways for managing the pathology and symptoms associated with Parkinson’s Disease.
– Description: Fetal VM tissue transplantation involves grafting cells from the ventral mesencephalon region of fetal brain tissue into the striatum of Parkinson’s disease patients. These cells include dopamine-producing neurons that can integrate into the host brain and restore dopamine function.
– Institution: Lund University
– Researcher: Dr. Olle Lindvall and Dr. Anders Björklund
– Year: 1987, Initial studies conducted in the late 1980s and early 1990s, ongoing research continues
– Dosage: Variable dosages depending on the specific study and patient characteristics
– Type of Model: Clinical trials in human patients with Parkinson’s Disease
-Outcome: Mixed results observed in clinical trials, with some patients experiencing significant improvements in motor function and quality of life, while others show limited or transient benefits. Challenges include ethical concerns, limited availability of fetal tissue, and variability in transplantation outcomes.
2. Human Embryonic Stem Cells (hESCs):
– Description: Human embryonic stem cells are pluripotent cells derived from the inner cell mass of the blastocyst stage embryo. They have the capacity to differentiate into all cell types of the body, including dopamine-producing neurons. In Parkinson’s disease research, hESCs can be differentiated into dopaminergic neurons for transplantation.
– Institution: University of Wisconsin-Madison
– Researcher: Dr. James Thomson
– Year: 1998, initial studies conducted in the early 2000s, ongoing research continues
– Dosage: Variable, depending on the number of differentiated dopaminergic neurons transplanted, the specific study and cell delivery method (e.g., intracerebral transplantation)
– Type of Model: Preclinical study in animal models of Parkinson’s Disease, as well as clinical trials in human patients
-Outcome: Promising results observed in preclinical studies, with hESC-derived dopaminergic neurons showing survival, integration, and functional improvement in animal models. Clinical trials in human patients are ongoing, with initial safety and feasibility data being reported.
3. Human Fetal Neural Stem Cells (hfNSCs):
– Description: Human fetal neural stem cells are multipotent cells isolated from the developing human fetal brain. They have the capacity to differentiate into neurons, astrocytes, and oligodendrocytes. In Parkinson’s disease research, hfNSCs can be differentiated into dopaminergic neurons for transplantation.
– Institution: University of California, San Diego
– Researcher: Dr. Fred H. Gage
– Year: 2001, initial studies conducted in the mid-2000s, ongoing research continues
– Dosage: Variable, depending on the number of differentiated dopaminergic neurons transplanted, the specific study and cell delivery method
– Type of Model: Preclinical study in animal models of Parkinson’s Disease, as well as clinical trials in human patients
4. Induced Pluripotent Stem Cells (iPSCs):
– Description: Induced pluripotent stem cells are reprogrammed somatic cells, typically skin cells or blood cells, that have been genetically modified to resemble embryonic stem cells. They have the ability to differentiate into various cell types of the body, including dopaminergic neurons. In Parkinson’s disease research, iPSCs offer a patient-specific model for disease modeling and potential cell replacement therapies.
– Institution: Kyoto University
– Researcher: Dr. Shinya Yamanaka
– Year: 2006, initial studies conducted in the late 2000s, ongoing research continues
– Dosage: Variable, depending on the number of differentiated dopaminergic neurons transplanted
– Type of Model: Preclinical study in animal models of Parkinson’s Disease, as well as clinical trials in human patients
– Institution: Second Affiliated Hospital, Guangzhou Medical University
– Researcher: Dr. Jiawei Zhou
– Year: 2009, initial studies conducted in the mid-2000s, ongoing research continues
– Dosage: Variable, depending on the number of cells injected, the specific study, route of administration, and cell source
– Type of Model: Preclinical study in animal models of Parkinson’s Disease, as well as clinical trials in human patients
– Outcome: Promising results observed in preclinical studies, with MSCs showing neuroprotective effects, immunomodulation, and behavioral improvements in animal models. Clinical trials in human patients are ongoing, with preliminary data suggesting safety and potential therapeutic effects.
6. Dopaminergic Progenitor Cells:
– Description: Dopaminergic progenitor cells are precursor cells specifically committed to the dopaminergic lineage, capable of differentiating into mature dopaminergic neurons. These cells are crucial for replacing the lost dopaminergic neurons in Parkinson’s Disease and restoring dopamine levels in the brain.
– Institution: Lund University, Sweden
– Researcher: Dr. Malin Parmar
– Year: 2012
– Dosage: Intracerebral transplantation of 10 million to 20 million dopaminergic progenitor cells
– Type of Model: Preclinical study using rodent models of Parkinson’s Disease
– Outcome: Significant improvement in motor function and reduction in Parkinsonian symptoms observed in animal models, demonstrating the therapeutic potential of dopaminergic progenitor cell transplantation.
7. Gene-Edited Stem Cells:
– Description: Gene-edited stem cells refer to stem cells that have been modified using gene editing technologies, such as CRISPR-Cas9, to enhance their therapeutic potential or improve their safety profile for Parkinson’s Disease treatment. This may involve modifying genes related to dopaminergic neuron development, survival, or function.
– Institution: University of California, San Francisco (UCSF)
– Researcher: Dr. Arnold Kriegstein
– Year: 2018
– Dosage: Intracerebral transplantation of 5 million to 10 million gene-edited stem cells
– Type of Model: Preclinical study using non-human primate models of Parkinson’s Disease
– Outcome: Evaluation of the safety and efficacy of gene-edited stem cells for Parkinson’s Disease treatment, including assessment of graft survival, integration, and functional improvement. Preliminary results show promising outcomes in terms of motor function improvement and long-term graft survival.
These studies represent significant advancements in stem cell-based therapies for Parkinson’s Disease, highlighting the evolution of stem cell-based therapies in restoring dopaminergic function and ameliorating Parkinsonian symptoms. Further research and clinical trials are needed to fully assess their safety and efficacy in human patients[36-42].
16. Summary of some recent and current clinical trials investigating Cellular Therapy and Stem Cells for Parkinson’s Disease:
TRANSEURO Trial (2014-2024)
– Phase: II
– Intervention: Fetal cell transplantation
– Details: Transplantation of human fetal ventral mesencephalic tissue into the striatum of patients with Parkinson’s disease. The trial aims to determine the safety and efficacy of this approach.
– Details: Transplantation of human embryonic stem cell-derived dopaminergic progenitor cells into the brain of patients with Parkinson’s disease. The trial is assessing safety, tolerability and preliminary efficacy.
– Details: Intrathecal administration of autologous bone marrow-derived mesenchymal stem cells in patients with Parkinson’s disease. The study is evaluating safety and efficacy.
4. NCT03684122 (2018-2022)
– Phase: I/II
– Intervention: Autologous bone marrow-derived mesenchymal stem cells
– Details: Intravenous administration of autologous bone marrow-derived mesenchymal stem cells in patients with Parkinson’s disease. The study is assessing safety and efficacy.
5. NCT03684372 (2018-2022)
– Phase: I/II
– Intervention: Autologous bone marrow-derived mesenchymal stem cells
– Details: Intrathecal and intravenous administration of autologous bone marrow-derived mesenchymal stem cells in patients with Parkinson’s disease. The study is evaluating safety and efficacy of the combined route.
– Details: Intrathecal administration of allogenic adipose-derived mesenchymal stem cells in patients with Parkinson’s disease. The study aims to assess safety, tolerability and preliminary efficacy.
These trials are using various sources of stem cells, including fetal tissue, embryonic stem cells, autologous bone marrow-derived mesenchymal stem cells, and allogenic adipose-derived mesenchymal stem cells. The cells are being transplanted via different routes like intracranial, intrathecal and intravenous administration. While the results of these trials are still awaited, they represent promising avenues for cellular therapy in Parkinson’s disease[43-47].
17. Brain Cells Involved in the Pathogenesis of Parkinson’s Disease
The pathogenesis of Parkinson’s disease (PD) involves a complex interaction among various types of brain cells, each playing a distinct role in the progression of the disease. These cells include:
– Dopaminergic Neurons:
– Role: Dopaminergic neurons in the substantia nigra pars compacta are central to PD. These neurons produce dopamine, a neurotransmitter crucial for controlling movement. In PD, these neurons progressively degenerate, leading to a dopamine deficiency that manifests as the hallmark motor symptoms of the disease, such as tremors, rigidity, and bradykinesia.
– Glial Cells (Astrocytes, Microglia, and Oligodendrocytes):
– Astrocytes:
– Role: Astrocytes support neuronal function by maintaining the blood-brain barrier, providing metabolic support, and regulating neurotransmitter levels. In PD, dysfunctional astrocytes can fail to clear excess glutamate, contributing to excitotoxicity and neuronal damage.
– Microglia:
– Role: Microglia are the brain’s resident immune cells, responsible for clearing debris and damaged cells. In PD, microglia become chronically activated, releasing pro-inflammatory cytokines that exacerbate neuroinflammation and contribute to the degeneration of dopaminergic neurons.
– Oligodendrocytes:
– Role: Oligodendrocytes produce myelin, which insulates axons and ensures efficient nerve signal transmission. Although less directly involved in PD, oligodendrocyte dysfunction can disrupt neural communication, contributing to the disease’s progression.
– Alpha-Synuclein-Containing Neurons:
– Role: Alpha-synuclein is a protein normally found in neurons, particularly in the presynaptic terminals. In PD, alpha-synuclein aggregates abnormally, forming Lewy bodies, which are toxic to neurons. The accumulation of these aggregates is a key pathological feature of PD, leading to cellular dysfunction and death, particularly in dopaminergic neurons.
– GABAergic Neurons:
– Role: GABAergic neurons, which produce the inhibitory neurotransmitter GABA, are involved in modulating the activity of other neurons within the basal ganglia, a brain region critical for motor control. In PD, the loss of dopaminergic input disrupts the balance between excitatory and inhibitory signals in the basal ganglia, leading to motor symptoms.
– Cholinergic Neurons:
– Role: Cholinergic neurons, which release the neurotransmitter acetylcholine, are involved in cognitive functions and movement control. Degeneration of cholinergic neurons in PD contributes to non-motor symptoms, including cognitive decline and autonomic dysfunction.
– Serotonergic and Noradrenergic Neurons:
– Role: Serotonergic neurons (producing serotonin) and noradrenergic neurons (producing norepinephrine) are also affected in PD. The loss of these neurons contributes to non-motor symptoms, such as depression, anxiety, and sleep disturbances.
Together, the dysfunction and degeneration of these diverse cell types create a cascade of effects that lead to the clinical manifestations of Parkinson’s disease. The interplay between neuronal loss, neuroinflammation, protein aggregation, and disrupted neural circuitry underlies the complexity of PD pathology[48-50].
18. Progenitor Stem Cells Needed for Regeneration in Parkinson’s Disease
1. Dopaminergic Progenitor Stem Cells (DPSC)
2. GABAergic Progenitor Stem Cells (GABA-PSC)
3. Cholinergic Progenitor Stem Cells (C-PSC)
4. Serotonergic Progenitor Stem Cells (Sero-PSC)
5. Noradrenergic Progenitor Stem Cells (NA-PSC)
6. Astrocytic Progenitor Stem Cells (A-PSC)
7. Microglial Progenitor Stem Cells (M-PSC)
19. Comprehensive Progenitor Stem Cell Treatments for Parkinson’s Disease
In the treatment of Parkinson’s Disease (PD), our center protocols of various progenitor stem cells are employed to address specific neuronal and glial deficits. Dopaminergic progenitor stem cells (DPSC) are crucial for replacing the lost dopamine-producing neurons in the substantia nigra, essential for restoring motor function. GABAergic progenitor stem cells (GABA-PSC) aim to restore the balance of inhibitory signaling in the basal ganglia, which is disrupted by dopaminergic loss. Cholinergic progenitor stem cells (C-PSC) target the degeneration of cholinergic neurons, which affects cognitive and autonomic functions. Serotonergic progenitor stem cells (Sero-PSC) address the loss of serotonin-producing neurons that contribute to mood and sleep disturbances. Noradrenergic progenitor stem cells (NA-PSC) are used to replenish norepinephrine-producing neurons, which can help with attention and autonomic regulation. Astrocytic progenitor stem cells (A-PSC) support neuronal health by replenishing astrocytes that maintain the blood-brain barrier and regulate neurotransmitter levels. Finally, microglial progenitor stem cells (M-PSC) are involved in modulating neuroinflammation and clearing cellular debris, which can reduce neuronal damage and promote overall brain health.
Combining these stem cell types in treatment protocols aims to address the multifaceted nature of PD and improve patient outcomes[51-53].
20. What are the ethical issues surrounding the use of Fetal/Embryonic Stem Cells (ESCs) in Parkinson’s Disease treatment, and why is it not supported?
– Destruction of human embryos during extraction of embryonic stem cells raises ethical concerns about the moral status of the embryo and the right to life.
– Risk of uncontrolled cell growth and tumor formation, known as teratoma formation, when embryonic stem cells are transplanted into patients.
– Issues of consent and the commodification of embryos may arise due to the procurement of embryos from vitro fertilization (IVF) clinics for research purposes.
21. Sources of Allogenic Mesenchymal Stem Cells (MSCs) Used in the Treatment of Parkinson’s Disease
– Bone Marrow-Derived MSCs (BM-MSCs): MSCs obtained from the bone marrow of healthy donors.
– Adipose Tissue-Derived MSCs (AD-MSCs): MSCs isolated from the adipose (fat) tissue of donors.
– Umbilical Cord-Derived MSCs (UC-MSCs): MSCs sourced from the Wharton’s jelly of the umbilical cord.
– Placenta-Derived MSCs (P-MSCs): MSCs extracted from the placental tissue after childbirth.
– Amniotic Fluid-Derived MSCs (AF-MSCs): MSCs harvested from the amniotic fluid, which surrounds the fetus during pregnancy[57-61].
22. Early Genetic Testing: A Key Strategy in Parkinson’s Disease Prevention and Management
At our Anti-Aging and Regenerative Medicine Center of Thailand, our Preventive, Anti-Aging Doctors and Regenerative Neurologists strongly advocate for genetic DNA sequencing in individuals with a significant familial history of Parkinson’s Disease (PD). Early genetic testing plays a pivotal role in the prevention and management of PD by identifying genetic mutations associated with the disease, such as those in the LRRK2, PARK7, PINK1, PRKN, and SNCA genes.
By detecting these genetic abnormalities early, individuals with a family history of PD can make informed decisions regarding lifestyle modifications and potential therapeutic interventions that may delay or even prevent the onset of the disease. Additionally, genetic testing in sporadic cases can uncover rare genetic variants that predispose individuals to Parkinson’s, enabling targeted surveillance and proactive management strategies.
Through the use of advanced genetic testing technologies at our center, we empower individuals to take proactive steps in safeguarding against the development of Parkinson’s Disease, ultimately enhancing disease prevention and management efforts[62-66].
23. Proactive Genetic Testing: Enhancing Parkinson’s Disease Prevention and Family Care
In addition to offering advanced cell-based treatments for Parkinson’s Disease, our team of neurologists and preventive specialists extends care beyond the patient to their family members. We provide comprehensive DNA testing services aimed at identifying specific genetic mutations within the family that may contribute to the development and progression of Parkinson’s at its earliest stages.
Through detailed genetic analyses, we offer personalized risk assessments and genetic counseling to at-risk individuals. This approach empowers families with knowledge about their genetic predisposition to Parkinson’s Disease, facilitating early detection and intervention. By implementing targeted preventive measures, we aim to reduce disease risk and optimize long-term health outcomes for patients and their families[62-66].
The risk factors for Parkinson’s Disease (PD) include age, genetic predisposition, exposure to environmental toxins, head injuries, and certain lifestyle factors such as lack of exercise. While some risk factors like age and genetics cannot be altered, lifestyle modifications such as regular physical activity, maintaining a balanced diet, avoiding exposure to harmful chemicals, and managing stress can significantly reduce the risk of PD progression.
Patients with specific genetic mutations, such as those in the LRRK2, PINK1, or SNCA genes, have a higher risk of developing Parkinson’s Disease. Additionally, individuals with a family history of PD or other neurodegenerative disorders are at an increased risk.
For those with a higher predisposition, it is essential to work closely with healthcare providers to manage their condition through regular monitoring, genetic counseling, and lifestyle adjustments. At our center, we also offer innovative cell-based therapies aimed at slowing disease progression and improving overall neurological health, providing a comprehensive approach to Parkinson’s Disease prevention and management.
At our Preventive and Regenerative Medicine Center in Thailand, our team of Preventive Medicine doctors and Regenerative Neurologists prioritizes annual comprehensive medical check-ups to assess individual risk factors for Parkinson’s Disease (PD) and customize lifestyle regimens accordingly. We emphasize the importance of regular exercise, adequate rest, and a diet rich in neuroprotective foods. In addition, we carefully prescribe medications to manage symptoms and control contributing factors such as oxidative stress and neuroinflammation.
Alongside these preventive measures, we offer specialized Parkinson’s Disease-focused cell-based protocols. These protocols utilize Cellular Therapy and various Neural Progenitor Stem Cells to support the regeneration of affected neurons and enhance neuroplasticity. By promoting the development of new neural connections and potentially slowing disease progression, these advanced therapies aim to optimize neurological health and improve the quality of life for individuals at risk of Parkinson’s Disease[67-71].
25. Our Main Sources of Allogenic Stem Cells for Parkinson’s Disease Treatment
At our Anti-Aging and Regenerative Medicine Center of Thailand, the primary sources for our Cellular Therapy and various progenitor stem cells for treating Parkinson’s Disease include both autologous cells from the patient and allogenic cells donated by others. For allogenic sources, we utilize donations that are facilitated after the delivery of a healthy child. Parents have the option to donate the amniotic fluid, placenta, or umbilical cord blood, which are often discarded as medical waste. These donated tissues are rich in mesenchymal stem cells (MSCs) and progenitor stem cells, which are then carefully processed for therapeutic use. Additionally, dental pulp, which is a rich source of stem cells, particularly from young teeth, is another valuable source. These stem cells are highly potent and capable of differentiating into various cell types, making them an excellent resource for regenerative therapies aimed at treating Parkinson’s Disease[72-74].
26. Innovative Stem Cell Therapy for Parkinson’s Disease Treatment
At our Center for Anti-Aging and Regenerative Medicine in Thailand, we advocate for the use of allogenic stem cell transplants as a promising treatment for patients with Parkinson’s disease for several compelling reasons:
– Youthful and Healthy Source: Our allogenic stem cells are sourced from young, healthy donors, ensuring a robust supply of cellular therapy with optimal regenerative potential. This is crucial in addressing the loss of dopaminergic neurons characteristic of Parkinson’s disease, which significantly contributes to motor symptoms.
– Avoidance of Age-Related Decline: Unlike autologous stem cells, which may suffer from age-related declines in regenerative capacity, our enhanced allogenic stem cells are fortified with neurogenesis growth factors. This approach offers a more potent therapeutic option, potentially leading to improved motor function and reduced symptoms in Parkinson’s patients.
– Genetic Integrity: Our neural progenitor cell lines are meticulously cultured and verified to be free from genetic defects that could compromise therapeutic efficacy. This focus on genetic integrity reduces the risk associated with autologous stem cell therapies, which may carry inherent genetic issues.
– Adaptability and Versatility: Our team of stem cell researchers and scientists ensures that the quality of our allogenic stem cells meets rigorous standards. These cells exhibit remarkable adaptability and versatility, enabling them to differentiate into various cell types efficiently, which is essential for effective tissue repair and regeneration in the context of neurodegenerative diseases like Parkinson’s.
– Streamlined Treatment Process: The administration of allogenic stem cell transplants by our medical professionals eliminates the need for harvesting and processing the patient’s own stem cells, thus streamlining the treatment process and minimizing potential delays. The infusion of our cellular therapy and allogenic stem cells can be completed in just 45-60 minutes per session, making it a convenient option for patients seeking relief from their symptoms.
Recent studies indicate that stem cell transplantation can effectively improve motor function and reduce the severity of Parkinson’s disease symptoms for at least 12 months, making it a viable option for long-term management of the disease. By focusing on innovative stem cell therapies, we aim to enhance the quality of life for patients battling Parkinson’s disease while addressing the underlying neurodegenerative processes[75-79].
27. Why don’t we support intracranial Dopaminergic Stem Cell therapy?
Intracranial stem cell injection at 14 distinct locations within the brain of Parkinson’s disease patients represents a sophisticated therapeutic strategy aimed at addressing the multifaceted pathology of the condition. This procedure involves precisely targeting key anatomical structures affected by Parkinson’s, including the substantia nigra, striatum, and other basal ganglia nuclei, as well as regions involved in motor control and dopamine regulation.
Intracranial dopaminergic stem cell transplantation, while holding promise as a potential treatment for Parkinson’s Disease, is highly invasive and associated with significant risks. The procedure involves surgically implanting stem cells into specific regions of the brain to replenish dopamine-producing neurons lost in Parkinson’s.
The invasive nature of the surgery poses considerable risks, including infection, bleeding, and damage to surrounding brain tissue.
Moreover, the effectiveness and long-term outcomes of intracranial transplantation remain uncertain, with limited evidence supporting its efficacy. Given the inherent risks and lack of robust clinical data, we do not support the widespread adoption of intracranial dopaminergic stem cell transplantation as a standard treatment for Parkinson’s Disease.
28. How Long Does It Take to See the Benefits of Our Cellular Therapy and Neural Stem Cell Protocols for Parkinson’s Disease?
Our specialized cell-based therapeutic approach for Parkinson’s Disease has shown promising results, with many patients experiencing noticeable improvements within a few weeks of initiating treatment. Patients typically undergo infusions of 20-30 million allogenic Mesenchymal Stem Cells (MSCs) combined with various Neural Progenitor Growth Factors and Peptides. Early signs of progress are often observed after the first or second treatment sessions, including enhancements in motor function, balance, and cognitive abilities. These improvements continue to develop over the following months, with significant milestones typically observed at the 2, 4, and 6-month intervals post-therapy.
However, to achieve and maintain these regenerative outcomes, it is crucial that patients engage in ongoing rehabilitative therapy. This includes exercises and activities focused on restoring motor skills, sensory processing, speech and language abilities, cognitive functions, and overall neurological health. Consistent participation in these rehabilitative sessions is essential for ensuring that the benefits of our Brain Regeneration Protocols are sustained over the long term, supporting the patient’s journey toward optimal neurological recovery and improved quality of life[83-86].
29. What specific components comprise our specialized protocols for Parkinson’s Regenerative Cellular Therapy and Stem Cell treatment?
Drawing upon two decades of clinical experience in treating Parkinson’s Disease patients worldwide since 2004 with our Cell-based and Regenerative Therapy, our Anti-Aging and Regenerative Center of Thailand provides optimized dosing regimens, employing the most effective and safest approaches for Cellular Therapy and Neural Stem Cell Therapy in Parkinson’s Disease.
The dosage of Cellular Therapy and Dopamine-producing Brain Stem Cells used in our special Parkinson’s Disease treatment protocols vary depending on the specific protocol and stage of the disease. At our Neurogenerative Medicine Center of Thailand, our team of stem cell researchers and regenerative neurologists collectively decide to initiate the infusion of cell-based therapy, which consists of 60-90 million mesenchymal stem cells (MSCs) divided into three separate administrations over a full treatment protocol lasting 10-14 days (about 2 weeks).
This comprehensive approach also includes the incorporation of dopaminergic progenitor growth factors and brain regenerative peptides. These therapeutic agents are administered either directly into the brain or via intravenous, intranasal, or intrathecal routes by a team of holistic and regenerative neurosurgeons and neurologists[87-89].
30. Why do we consistently advise Parkinson’s patients to undergo our Cellular Therapy and Neural Stem Cells treatment as soon as possible at our Anti-Aging and Regenerative Medicine Center in Thailand?
The effective utilization of our Cellular Therapy and Dopaminergic Stem Cells in Parkinson’s patients hinges significantly on the timeliness of treatment initiation. Our team of Neurologists and Regenerative Specialists consistently stress the importance of early intervention to optimize the therapeutic advantages offered by our innovative treatment protocols. By receiving our Neuroprogenitor Cell-based Therapy at earlier stages of the disease progression, many of our Parkinson’s patients experience enhanced preservation of dopaminergic neurons, better symptom management, and potentially slower disease progression.
Contact us now for prompt evaluation and access to our Cellular Therapy and Dopaminergic Stem Cell interventions which hold promise for improving outcomes and quality of life for individuals with Parkinson’s Disease[87-89].
31. Are the Specialized Treatment Protocols for Parkinson’s Disease Outpatient and Non-Invasive?
Our specialized Neuroregenerative Treatment Protocols for Parkinson’s Disease utilize advanced progenitor stem cells, including Dopaminergic Progenitor Stem Cells (DPSC), GABAergic Progenitor Stem Cells (GABA-PSC), Cholinergic Progenitor Stem Cells (C-PSC), and others, along with Regenerative Motor Neuron Growth Factors and specialized Neurotrophic and Neural factors. These cell-based treatments are typically administered through intravenous (IV) infusion or direct gluteal injection, making the procedures minimally invasive and suitable for outpatient care.
In cases where Parkinson’s Disease has progressed to a more advanced stage, more direct methods, such as intraspinal injection following a lumbar puncture at the L4-5 level, may be recommended. This procedure is performed under local anesthesia to ensure patient comfort. After the procedure, patients are monitored for 1-2 hours by our regenerative medical team to ensure safety and to prevent complications such as brain stem herniation. These protocols are designed to be as non-invasive as possible while delivering targeted regenerative therapy to address the complex needs of Parkinson’s Disease patients[90-92].
32. Revolutionary Intranasal and Intrathecal Stem Cell Delivery for Parkinson’s Disease Treatment
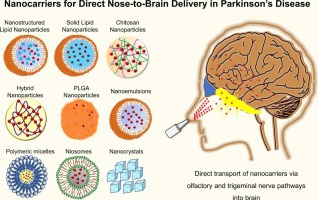
Innovative Approaches: Anti-Aging and Regenerative Medicine Center of Thailand Pioneers Intranasal and Intrathecal Delivery of Cellular Therapy for Parkinson’s Disease Regeneration
Our center has developed an advanced protocol for treating Parkinson’s Disease that incorporates intranasal, intravenous (IV), and intrathecal delivery methods for Cellular Therapy and Stem Cells. This comprehensive approach ensures that stem cells and neurotrophic factors reach critical areas of the brain and spinal cord more effectively. The intranasal route allows direct access to the brain through the olfactory and trigeminal nerves, bypassing the blood-brain barrier and delivering cells and growth factors to the affected regions swiftly. The intrathecal route, involving injection into the cerebrospinal fluid via lumbar puncture, ensures targeted delivery to the spinal cord and brain, enhancing the regenerative potential of the therapy. These innovative delivery methods, combined with traditional IV infusion, offer a more holistic and potent treatment for Parkinson’s Disease, potentially improving outcomes in motor function, cognitive abilities, and overall neurological health[90-92].
33. Mechanisms of Action of Cellular Therapy and Neuroprogenitor Stem Cells in Treating Parkinson’s Disease
Cellular therapy and the use of various neuroprogenitor stem cells represent a promising approach in treating Parkinson’s Disease (PD), targeting the underlying pathophysiology of the disease. The mechanisms through which these therapies exert their effects are multifaceted, involving cell replacement, neuroprotection, and modulation of the brain’s microenvironment
1. Cell Replacement:
– Dopaminergic Progenitor Stem Cells (DPSC): These cells differentiate into dopaminergic neurons, replacing the lost or damaged neurons in the substantia nigra. This replenishment is critical for restoring dopamine levels, which are essential for motor control and coordination.
– GABAergic Progenitor Stem Cells (GABA-PSC): By differentiating into GABA-producing neurons, these cells help reestablish the inhibitory signaling balance in the basal ganglia, counteracting the motor symptoms caused by dopaminergic loss.
2. Neuroprotection:
– Cholinergic Progenitor Stem Cells (C-PSC): These cells contribute to neuroprotection by replacing cholinergic neurons and enhancing acetylcholine levels, which are vital for cognitive functions and autonomic regulation.
– Astrocytic Progenitor Stem Cells (A-PSC): Astrocytes support neurons by maintaining the blood-brain barrier, regulating neurotransmitters, and providing metabolic support. A-PSC can regenerate astrocytes, thereby enhancing the brain’s natural defense mechanisms against neurodegeneration.
3. Modulation of the Brain’s Microenvironment:
– Microglial Progenitor Stem Cells (M-PSC): These cells differentiate into microglia, which play a role in modulating neuroinflammation. By reducing inflammation, M-PSC help create a more conducive environment for neuronal survival and regeneration.
– Oligodendrocyte Progenitor Stem Cells (OPC): OPCs are essential for remyelination, restoring the myelin sheath around neurons. This not only improves signal transmission but also protects neurons from further damage[93-97].
34. Optimizing Therapeutic Efficacy for Clinical Applications
To maximize the therapeutic potential of these Cellular Therapy and Stem Cells, several strategies can be employed:
– Combination Therapy: Using a combination of different progenitor stem cells, such as DPSC, GABA-PSC, and A-PSC, can address the multifaceted nature of PD more effectively. This holistic approach can improve overall brain function by simultaneously targeting different neuronal pathways.
– Targeted Delivery: Utilizing intranasal, intrathecal, and intravenous delivery routes can enhance the concentration of stem cells in the affected brain regions. Intranasal delivery, in particular, can bypass the blood-brain barrier, while intrathecal delivery targets the cerebrospinal fluid, ensuring that stem cells reach critical areas in the brain and spinal cord.
– Preconditioning and Growth Factors: Preconditioning stem cells with neurotrophic factors or engineering them to overexpress specific growth factors like Brain-Derived Neurotrophic Factor (BDNF) can enhance their survival, differentiation, and integration into the host tissue.
– Rehabilitation and Supportive Therapies: Incorporating rehabilitation programs that focus on motor skills, cognitive functions, and sensory processing can synergize with cellular therapy, promoting better integration of the new cells and enhancing their functional outcomes.
By understanding and optimizing these mechanisms, cellular therapy and neuroprogenitor stem cells can be more effectively integrated into clinical applications for treating Parkinson’s Disease, offering hope for better management and potential recovery from this debilitating condition[93-97].
35. Stem Cells and Exosomes: Advancing Regeneration in Parkinson’s Disease Patients
Patients with Parkinson’s Disease (PD) can achieve significant benefits from our Cellular Therapy and Neuroprogenitor Stem Cells, enhanced by Exosomes. These advanced therapies offer a novel approach that goes beyond traditional treatments, which primarily focus on symptomatic relief. By harnessing the regenerative potential of Stem Cells, our protocols aim to address the underlying neurodegeneration in PD[98-100].
36. Cellular Therapy and Neuroprogenitor Stem Cells
Neuroprogenitor Stem Cells possess multipotent properties, enabling them to differentiate into various types of neural cells. This capability is crucial for replenishing and repairing damaged neural structures, targeting the root causes of the neurological deficits associated with Parkinson’s Disease. Research indicates that stem cell therapies can lead to functional improvements in PD models, suggesting their potential for human applications[98-100].
37. Role of Exosomes
Exosomes derived from stem cells play a pivotal role as mediators of paracrine signaling, orchestrating a cascade of molecular events that promote neuroprotection and modulate immune responses. These exosomes activate endogenous repair mechanisms and secrete neurotrophic factors, which facilitate the reconstruction of neural circuitry. This process can lead to accelerated recovery and measurable improvements in motor function and cognitive abilities in PD patients.
Integrating Cellular Therapy and Neuroprogenitor Stem Cells with Exosomes offers a promising approach to improving outcomes for Parkinson’s Disease patients. This strategy not only addresses immediate symptoms but also fosters long-term neural recovery and functional restoration, representing a significant advancement in Parkinson’s Disease treatment[98-100].
38. How are improvement outcomes in Parkinson’s Disease assessed after our Cellular Therapy and Neural Progenitor Stem Cell infusion at our Dopaminergic Progenitor Cell Therapy and Regenerative Medicine Center of Thailand?
Our team of neurologists and regenerative specialists employ a range of assessment tools to evaluate the improvement outcomes of patients with Parkinson’s disease. This encompasses:
– Clinical evaluations using standardized rating scales such as the Unified Parkinson’s Disease Rating Scale (UPDRS) or the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS)
– Monitoring of motor symptoms including tremors, bradykinesia, rigidity, and gait disturbances
– Neuroimaging studies such as positron emission tomography (PET) or functional magnetic resonance imaging (fMRI) to visualize changes in brain activity, dopamine levels, and neural connectivity
– Assessment of patient-reported outcomes including quality of life measures and subjective symptom improvement
– Utilization of comprehensive assessment methods to evaluate the overall impact of Cellular Therapy and Stem Cell infusion on Parkinson’s Disease symptoms and tailor future treatment strategies accordingly[101-103].
39. What criteria must individuals with Parkinson’s disease meet to be eligible for our specialized Cell-based Therapy and Stem Cell Treatment for Parkinson’s at Thailand’s Cellular Therapy and Neural Stem Cell Treatments?
It is crucial to acknowledge that stem cell treatment for PD may not be a suitable choice for every case, as each patient’s condition is unique and requires individualized care. Therefore, to provide the most accurate assessment, personalized recommendations and tailor-made Cellular Therapy and Stem Cell regimens, our team of Regenerative medicine doctors and neurologists kindly request all potential patients to submit their recent medical reports, relevant investigations, including comprehensive lab results, CT brain, and PET scan to our esteemed medical team. With two decades of experience in treating patients with various forms of Parkinson’s disease together with a meticulous review of your clinical data, we are well-equipped to identify the optimal neuro-regenerative treatment protocols of Cellular Therapy and Stem Cells and advise our patients on the most advantageous treatment options[104-108].
41.What is the classic presentation of Parkinson’s Disease?
The progression and disability of Parkinson’s Disease are attributed to multiple factors, primarily stemming from the loss of dopamine-secreting neurons in the substantia nigra region of the brain. This loss disrupts the delicate balance of neurotransmitters, particularly dopamine, which plays a crucial role in regulating movement and coordination.
As dopamine levels decline, individuals experience motor symptoms such as tremors, bradykinesia, and muscle rigidity[109-113].
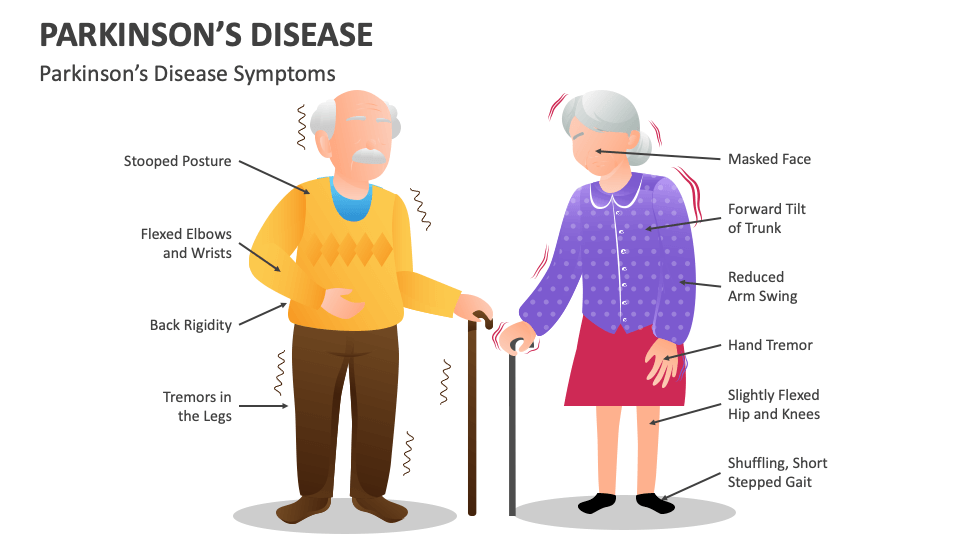
42. The classic presentation of Parkinson’s Disease includes a combination of motor and non-motor symptoms. Motor symptoms are often the most noticeable and may include:
1. Tremors: Tremors, typically starting in one hand, are one of the hallmark symptoms of Parkinson’s Disease. They often occur at rest and may improve with purposeful movement.
2. Bradykinesia: This refers to slowness of movement, which can affect various activities such as walking, getting out of a chair, or performing fine motor tasks.
3. Muscle Rigidity: Stiffness or rigidity of muscles, which can lead to decreased range of motion and difficulty with movement.
4. Postural Instability: Impaired balance and coordination, leading to difficulty maintaining an upright posture and an increased risk of falls.
Additionally, the degeneration of dopaminergic pathways leads to widespread neurodegeneration and dysfunction across various brain regions, contributing to non-motor symptoms such as cognitive impairment, mood disorders, and autonomic dysfunction[109-113].
43. Non-motor symptoms of Parkinson’s Disease may also be present and can include:
1. Bradyphrenia: Slowness of thought processes and cognitive impairment, including difficulties with memory, concentration, and executive function.
2. Hyposmia: Reduced sense of smell, often occurring years before motor symptoms develop.
3. REM Sleep Behavior Disorder (RBD): Acting out dreams while asleep, which can result in vocalizations, movements, or even injury to oneself or a sleeping partner.
4. Autonomic Dysfunction: Symptoms such as constipation, urinary urgency, orthostatic hypotension (a drop in blood pressure upon standing), and sexual dysfunction.
5. Mood Changes: Depression, anxiety, apathy, and other mood disorders are common in Parkinson’s Disease.
It’s important to note that Parkinson’s Disease can vary widely from person to person, and not all individuals will experience the same symptoms or progression of the disease. Additionally, symptoms may change over time and may respond differently to treatment[109-113].
44. Types of Parkinson’s Disease: A Detailed Overview
Parkinson’s Disease (PD) is a neurodegenerative disorder with various subtypes, each characterized by distinct clinical features, progression rates, and underlying pathophysiological mechanisms. The classification of PD can be broadly divided into the following categories:
1. Idiopathic Parkinson’s Disease (IPD)
Idiopathic Parkinson’s Disease is the most common form, accounting for approximately 80-85% of all PD cases. The exact cause is unknown, but it is believed to result from a combination of genetic and environmental factors. Idiopathic PD is characterized by the progressive degeneration of dopaminergic neurons in the substantia nigra, leading to motor symptoms such as bradykinesia, rigidity, and tremor. Patients may also experience non-motor symptoms, including cognitive decline, depression, and autonomic dysfunction.
2. Genetic Parkinson’s Disease
Genetic forms of Parkinson’s Disease are less common, accounting for 10-15% of cases. These forms are associated with specific gene mutations that may be inherited in an autosomal dominant or recessive manner. Some of the well-known genetic mutations include:
– LRRK2 (Leucine-Rich Repeat Kinase 2): The most common genetic cause of PD, particularly in familial cases.
– PINK1 (PTEN-Induced Putative Kinase 1) and PARK7 (DJ-1): Mutations in these genes are associated with autosomal recessive early-onset Parkinson’s.
– SNCA (Alpha-Synuclein): Mutations or multiplications in this gene can lead to the production of abnormal alpha-synuclein, a protein that aggregates in the brains of PD patients.
– GBA (Glucocerebrosidase): Mutations in this gene, associated with Gaucher disease, have also been linked to an increased risk of developing PD.
Atypical Parkinsonism includes a group of disorders that present with parkinsonian features but have additional symptoms or a different underlying pathology. These conditions tend to have a more rapid progression and poorer response to levodopa therapy. Key subtypes include:
– Corticobasal Degeneration (CBD): Features include asymmetric motor symptoms, apraxia, and cognitive decline.
– Lewy Body Dementia (LBD): Involves cognitive impairment with prominent visual hallucinations, fluctuating attention, and parkinsonism. It shares pathological similarities with Parkinson’s Disease, particularly the presence of Lewy bodies.
4. Secondary Parkinsonism
Secondary Parkinsonism refers to parkinsonian symptoms that result from identifiable causes other than neurodegeneration of the substantia nigra. These causes include:
– Drug-Induced Parkinsonism: Caused by medications that block dopamine receptors, such as antipsychotics.
– Vascular Parkinsonism: Associated with cerebrovascular disease such as ischemic stroke and characterized by lower-body parkinsonism, gait disturbances, and a lack of tremor.
– Toxic Parkinsonism: Resulting from exposure to neurotoxins like manganese or carbon monoxide.
– Post-Traumatic Parkinsonism: Seen in individuals with a history of repeated head trauma.
5. Juvenile Parkinsonism
Juvenile Parkinsonism is a rare form of PD that occurs in individuals under the age of 21. It is often linked to genetic mutations, particularly in the PARK2 (parkin) gene. Symptoms are similar to those of typical Parkinson’s Disease but may include additional features like dystonia.
Understanding the different types of Parkinson’s Disease is crucial for accurate diagnosis, treatment, and management. Each subtype has unique characteristics that influence the choice of therapeutic strategies, including pharmacological interventions, surgical options, and emerging therapies such as cellular and gene therapies[114-118].
45. Stages of Parkinson’s Disease: A Detailed Technical Overview
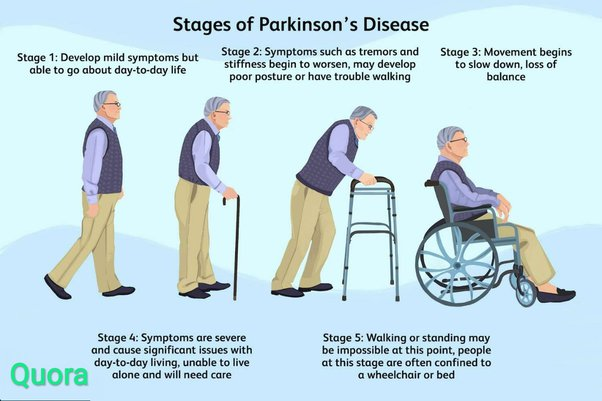
Parkinson’s Disease (PD) progresses through five distinct stages, each characterized by worsening symptoms and increasing impact on the patient’s daily life. These stages are typically assessed using the Hoehn and Yahr scale, a widely accepted system that categorizes the severity of motor symptoms and functional impairment. Here is a detailed overview of the five stages:
1. Stage 1: Mild or Early-Stage Parkinson’s Disease
– Symptoms: In Stage 1, symptoms are mild and typically affect only one side of the body (unilateral). Common symptoms include a slight tremor, rigidity, or bradykinesia (slowness of movement) in one limb. Facial expressions might become slightly less animated, and posture may be slightly stooped.
– Functional Impact: Daily activities are usually not significantly affected, and the patient can continue with normal routines. Often, symptoms are so mild that they may go unnoticed by others.
– Diagnosis: Early diagnosis can be challenging because symptoms are subtle. However, patients may begin seeking medical advice due to noticeable changes in motor function.
2. Stage 2: Moderate or Bilateral Involvement
– Symptoms: As the disease progresses to Stage 2, symptoms become bilateral, affecting both sides of the body. Tremors, rigidity, and bradykinesia are more pronounced, and the patient may experience stiffness in the neck and torso.
– Functional Impact: Although daily activities can still be performed, they become more difficult and may take longer to complete. Balance is usually still intact, but the patient may notice changes in posture, gait, and facial expressions.
– Diagnosis: Diagnosis is more straightforward at this stage due to the clear presence of bilateral symptoms. Patients may begin to require more effort to perform routine tasks.
3. Stage 3: Mid-Stage Parkinson’s Disease
– Symptoms: Stage 3 is characterized by worsening symptoms, particularly in terms of balance. Patients often experience postural instability, which increases the risk of falls. Motor symptoms such as bradykinesia and rigidity are more severe, and tremors may be more noticeable.
– Functional Impact: This stage marks a significant decline in the patient’s ability to perform daily activities independently. Tasks like dressing, eating, and writing may become increasingly challenging. The patient may still be able to live independently but with considerable effort and caution.
– Diagnosis: Stage 3 is typically the point at which patients seek more aggressive treatment strategies, including medication adjustments and physical therapy, to manage symptoms.
4. Stage 4: Severe Parkinson’s Disease
– Symptoms: In Stage 4, symptoms are severe and disabling. Patients experience significant motor impairment, including severe bradykinesia, rigidity, and tremors. Postural instability is pronounced, and falls become a major concern.
– Functional Impact: Patients usually require assistance with most daily activities and may be unable to live independently. Walking may require a walker or other assistive devices, and some patients may need help with personal care.
– Diagnosis: At this stage, treatment focuses on managing symptoms and maintaining the highest possible quality of life. Non-motor symptoms, such as cognitive decline, depression, and autonomic dysfunction, may also become more prominent.
5. Stage 5: Advanced Parkinson’s Disease
– Symptoms: Stage 5 is the most advanced stage, characterized by severe motor and non-motor symptoms. Patients may be unable to stand or walk and are often wheelchair-bound or bedridden. Motor symptoms are severe, and patients may experience significant freezing episodes, where they are temporarily unable to initiate movement.
– Functional Impact: Patients require full-time care and assistance with all activities of daily living, including eating, dressing, and bathing. Non-motor symptoms, such as dementia, hallucinations, and severe autonomic dysfunction (e.g., difficulty swallowing, urinary incontinence), are common.
– Diagnosis: Management at this stage is focused on palliative care, ensuring comfort, and addressing complications such as infections, pressure sores, and malnutrition.
Parkinson’s Disease progresses through five distinct stages, each with specific clinical features and functional impacts. Understanding these stages is crucial for tailoring treatment strategies to the individual’s needs, optimizing quality of life, and providing appropriate support as the disease advances[119-123].
46. Prognosis of Different Types of Parkinson’s Disease: A Comprehensive Overview
The prognosis of Parkinson’s Disease (PD) varies depending on the subtype, the presence of genetic mutations, the age of onset, and individual patient factors. While PD is a progressive neurodegenerative disorder with no known cure, the rate of progression, symptom severity, and overall impact on life expectancy differ across the various types of Parkinson’s Disease. Here is a detailed examination of the prognosis for each subtype:
1. Idiopathic Parkinson’s Disease (IPD)
– Prognosis: Idiopathic Parkinson’s Disease, the most common form, typically has a gradual progression over many years. The progression rate can vary widely among individuals. Early-stage patients may live many years with relatively mild symptoms, but as the disease advances to stages 3-5, significant disability often occurs.
– Life Expectancy: With optimal medical management, life expectancy may not be drastically shortened compared to the general population, though complications such as pneumonia, falls, and aspiration can lead to a higher mortality rate in the later stages.
– Prognosis: The prognosis for genetic forms of Parkinson’s Disease depends on the specific mutation involved. For example:
– LRRK2-Associated PD: This form often has a slower progression and may respond well to levodopa. However, patients may experience motor complications earlier in the disease course.
– PINK1 and PARK7-Associated PD: These typically present with early-onset PD and may have a more benign course but with a higher likelihood of dystonia. Patients may have a longer life expectancy due to earlier diagnosis and management.
– SNCA-Associated PD: Often associated with more severe disease, including early cognitive decline and rapid progression of motor symptoms. This subtype may lead to a shorter life expectancy due to the rapid progression and associated complications.
– Life Expectancy and Quality of Life: Similar to idiopathic PD, life expectancy can be near normal with proper management, but certain genetic forms may lead to more severe symptoms or earlier onset, impacting overall prognosis.
– Prognosis: MSA progresses more rapidly than idiopathic PD, with patients often becoming severely disabled within 5-10 years of onset. Autonomic dysfunction, including issues like orthostatic hypotension, urinary incontinence, and swallowing difficulties, significantly impacts prognosis.
– Life Expectancy: Life expectancy is typically reduced, with many patients living 6-10 years after diagnosis, largely due to complications like aspiration pneumonia and sudden death due to autonomic failure.
– Quality of Life: Quality of life declines rapidly due to severe motor and autonomic symptoms that are less responsive to conventional PD treatments.
– Prognosis: PSP has a faster progression than idiopathic PD, with severe balance issues, falls, and gaze palsy becoming prominent early in the disease. The condition often leads to significant disability within 3-5 years.
– Life Expectancy: Life expectancy is shortened, with many patients living 7-10 years post-diagnosis. Complications such as falls, dysphagia, and aspiration pneumonia contribute to increased mortality.
– Quality of Life: Quality of life is significantly impacted by early and severe motor impairment, cognitive decline, and difficulty with eye movements, leading to a rapid loss of independence.
– Corticobasal Degeneration (CBD):
– Prognosis: CBD is characterized by asymmetric motor symptoms, including dystonia and myoclonus, and progresses more rapidly than idiopathic PD. The condition often leads to severe disability within 5-7 years.
– Life Expectancy: Life expectancy is reduced, typically with a survival rate of 6-8 years post-onset. The rapid progression of motor symptoms and cognitive decline are primary factors.
– Quality of Life: Quality of life is severely affected by early motor and cognitive dysfunction, with patients requiring extensive care as the disease progresses.
– Prognosis: LBD is characterized by a combination of cognitive decline, hallucinations, and parkinsonism, with a more rapid progression than idiopathic PD. Cognitive symptoms, particularly fluctuations in attention and visual hallucinations, often dominate the clinical picture.
– Life Expectancy: Life expectancy is generally shorter, with an average survival of 5-8 years after symptom onset. The rapid cognitive decline and susceptibility to complications like infections contribute to increased mortality.
– Quality of Life: Quality of life is significantly impaired by the combination of motor and cognitive symptoms, with patients often requiring full-time care in the later stages.
4. Secondary Parkinsonism
– Prognosis: The prognosis of secondary parkinsonism depends on the underlying cause:
– Drug-Induced Parkinsonism: Symptoms may improve or resolve after discontinuing the offending drug, although some patients may have residual symptoms.
– Vascular Parkinsonism: The prognosis is often poorer compared to idiopathic PD, with a greater risk of falls and a lack of response to levodopa. Patients may experience a slower progression of symptoms but with significant functional impairment.
– Toxic Parkinsonism: Prognosis varies based on the extent of exposure and the reversibility of the toxic insult. Some patients may improve if the exposure is removed early, while others may have permanent deficits.
– Post-Traumatic Parkinsonism: Prognosis can be variable, depending on the severity and frequency of head trauma. Symptoms may progress over time, leading to significant disability.
– Life Expectancy and Quality of Life: Life expectancy and quality of life in secondary parkinsonism are generally lower than in idiopathic PD, particularly if the condition is due to irreversible causes like vascular disease or chronic drug exposure.
5. Juvenile Parkinsonism
– Prognosis: Juvenile Parkinsonism, characterized by early-onset (under 21 years), often has a slower progression compared to idiopathic PD. Patients may respond well to levodopa and other treatments, although motor complications such as dyskinesias may develop earlier.
– Life Expectancy: Life expectancy is generally favorable with early diagnosis and appropriate management, although patients may experience a long duration of disease-related disability.
– Quality of Life: Quality of life can be maintained for many years with proper treatment, but early onset means that patients may face many decades of managing symptoms, which can impact long-term quality of life.
The prognosis of Parkinson’s Disease varies significantly depending on the type and subtype. While idiopathic PD generally has a more favorable prognosis with a slow progression and near-normal life expectancy, atypical forms like MSA, PSP, and CBD have a more rapid course with significant disability and reduced life expectancy. Genetic forms of PD and juvenile parkinsonism have unique prognostic factors depending on the specific mutation or onset age. Understanding the specific type of Parkinson’s Disease is crucial for developing an appropriate management plan and providing accurate prognostic information to patients and their families[124-128].
47. Exploring Innovative Treatment Modalities: Cell Transplantation and Stem Cell Therapy in Parkinson’s Disease
Considering these challenges, Sue Broom provides a comprehensive account of two novel methodologies that have the potential to revolutionize the field of Parkinson’s disease treatment. One potential therapeutic avenue involves the transplantation of new cells, aiming to replace the degenerating ones. Although initial attempts to pursue this approach were undertaken several decades ago, the outcomes obtained were not encouraging, casting doubt upon the feasibility of this strategy. However, a recent and groundbreaking clinical trial known as the Transeuro trial has rekindled hope in the potential of Cellular Therapy and Stem Cells, offering the prospect of improved treatment outcomes. A second approach that has garnered significant attention involves the utilization of Cellular Therapy and Stem Cells. In her investigative report, Sue Broom delves into the experiences and perspectives of both medical professionals and patients who are actively involved in these ground-breaking trials, providing valuable insights into the potential benefits and challenges associated with these innovative treatment modalities.
The multifaceted nature of Parkinson’s pathology underscores the complexity of the disease and highlights the importance of comprehensive treatment strategies targeting both motor and non-motor manifestations [129-133].
48. The Pathogenesis of Parkinson’s Disease: A Complex Interplay of Genetic and Environmental Factors
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by the degeneration of dopaminergic neurons in the substantia nigra pars compacta, leading to a reduction in dopamine levels in the striatum. The primary pathological hallmark of PD is the presence of intracellular inclusions known as Lewy bodies, which are primarily composed of aggregated α-synuclein protein.
The exact cause of PD remains elusive, but growing evidence suggests a complex interplay between genetic and environmental factors in its pathogenesis:
Genetic Factors
– Mutations in genes such as α-synuclein, parkin, DJ-1, PINK1, and LRRK2 have been linked to familial forms of PD, providing insights into potential pathogenic mechanisms.
– Genetic factors are more prominent in early-onset PD, while environmental factors play a larger role in late-onset forms.
– Mutant α-synuclein can cause selective toxicity to dopaminergic neurons and impair the ubiquitin-proteasome system, leading to the accumulation of misfolded proteins.
Environmental Factors
– Exposure to certain toxins, such as pesticides and heavy metals, may increase the risk of developing PD.
– Environmental factors can trigger mitochondrial dysfunction, oxidative stress, and proteasome impairment, which are central to the pathogenesis of both genetic and sporadic forms of PD.
– Brain injuries or infections can also contribute to the development of PD.
Cellular Mechanisms
– Impairment in mitochondrial function, leading to energy metabolism disruption and increased oxidative stress, is a key factor in the death of dopaminergic neurons.
– Dysfunction in the ubiquitin-proteasome system and lysosomal pathways can result in the accumulation of misfolded proteins, such as α-synuclein, contributing to neurodegeneration.
– Maladaptive immune responses and neuroinflammation, potentially triggered in the gut, may accelerate the pathogenesis of PD.
While there are currently no disease-modifying treatments for PD, understanding the complex pathogenesis involving genetic and environmental factors provides a solid basis for the development of rational neuroprotective therapies. Targeting the key cellular mechanisms, such as mitochondrial dysfunction, protein aggregation, and neuroinflammation, may help halt the progression of this debilitating neurological condition[129-133].
49. What are the standard pharmacological therapies used to manage Parkinson’s Disease?
Despite the availability of effective pharmacological interventions, the efficacy of these treatments diminishes gradually over time, and they are also accompanied by a range of undesired effects. Furthermore, the highly idiosyncratic nature of the Parkinson’s disease condition, combined with the variability in its progression, renders the determination of appropriate dosages an intricate task.
Conventional treatments for Parkinson’s Disease typically include medications aimed at managing symptoms and improving quality of life. Some common medications used include:
1. Levodopa (brand names: Sinemet, Madopar): Levodopa is converted into dopamine in the brain, helping to replenish dopamine levels and alleviate motor symptoms such as tremors, stiffness, and bradykinesia. Common side effects include nausea, vomiting, dizziness, and dyskinesias (involuntary movements).
2. Dopamine Agonists (brand names: Mirapex, Requip, Neupro): These medications mimic the action of dopamine in the brain, helping to alleviate motor symptoms. They can be used as monotherapy or in combination with levodopa. Common side effects include nausea, dizziness, hallucinations, and impulse control disorders such as compulsive gambling or shopping.
3. Monoamine Oxidase-B (MAO-B) Inhibitors (brand names: Azilect, Eldepryl): MAO-B inhibitors help to increase dopamine levels in the brain by blocking the enzyme monoamine oxidase-B, which breaks down dopamine. Common side effects include nausea, headache, dizziness, and insomnia.
4. Catechol-O-Methyltransferase (COMT) Inhibitors (brand name: Comtan): COMT inhibitors prolong the effects of levodopa by inhibiting the enzyme catechol-O-methyltransferase, which breaks down levodopa. Common side effects include nausea, diarrhea, dyskinesias, and orange discoloration of urine.
5. Anticholinergics (brand names: Artane, Cogentin): These medications help to reduce tremors and muscle stiffness by blocking the action of acetylcholine, a neurotransmitter involved in motor control. Common side effects include dry mouth, constipation, blurred vision, and cognitive impairment.
6. Amantadine (brand name: Symmetrel): Amantadine is used to reduce dyskinesias (involuntary movements) associated with levodopa therapy and may also help alleviate other Parkinson’s symptoms. Common side effects include nausea, dizziness, insomnia, and hallucinations.
In addition to medication, other conventional treatments for Parkinson’s Disease may include physical therapy, occupational therapy, speech therapy, and deep brain stimulation surgery in advanced cases[134-138].
50. Cellular Therapy and Neuroprogenitor Stem Cells Across All Stages of Parkinson’s Disease: A Comparative Analysis
– Combination Therapy with All Progenitor Stem Cells: Including DPSC, GABA-PSC, C-PSC, A-PSC, M-PSC, OPC, and other supportive cells.
– Outcome of Cellular Therapy:
– Synergistic effects from the combination of progenitor stem cells lead to multi-faceted neuroregeneration and functional restoration.
– Improved motor function, reduced cognitive decline, and enhanced quality of life, even in advanced stages of the disease.
– Conventional Treatment Comparison:
– Levodopa-Carbidopa Infusion and Advanced DBS: Provide continuous dopamine delivery and motor control but with diminishing returns and increasing side effects.
– Outcome: Symptom management becomes challenging, with increased risk of medication-induced complications and surgical risks.
– Conventional Treatments primarily focus on symptomatic relief with diminishing returns as the disease progresses, and do not address the underlying causes of neuronal loss and degeneration[[134-138].
51. Our Commitment to Excellence in Parkinson’s Disease Treatment
At our state-of-the-art Stem Cell Laboratory, we are dedicated to providing the safest and most effective Cellular Therapy and Stem Cells for patients with Parkinson’s disease. Our unwavering commitment to quality and safety is evident in our adherence to the highest standards set by regulatory bodies and international organizations.
Our laboratory is registered with the Thai FDA for Cellular Therapy and Stem Cells and pharmaceutical production, ensuring strict compliance with all necessary regulations. We have also obtained certifications for good laboratory practice (GLP) and good manufacturing practice (GMP), demonstrating our commitment to maintaining the highest levels of quality control throughout our manufacturing processes.
Furthermore, our facility has achieved ISO4 and Class 10 certifications for ultra-cleanroom cell culture and biotechnology. This achievement underscores our dedication to providing a sterile and controlled environment for the production of our cellular therapy products, minimizing the risk of contamination and ensuring the safety of our patients.
Our allogenic stem cell transplants have been extensively studied in numerous research and clinical trials, providing robust scientific evidence for their efficacy in treating Parkinson’s disease. These studies have demonstrated the ability of our stem cell therapies to improve motor function, reduce symptoms, and potentially slow disease progression in patients with Parkinson’s disease.
By combining our 20 years of experience in assisting patients with neurodegenerative diseases, our commitment to safety and quality, and our strong scientific foundation, we are confident in our ability to deliver the highest standard of cellular therapy for Parkinson’s disease patients. Our dedication to innovation and excellence in regenerative medicine ensures that our patients receive the most advanced and effective treatments available[139-143].
52. Primary Outcome Assessments in Parkinson’s Disease
When evaluating the efficacy of treatments for Parkinson’s disease (PD), a variety of outcome measures are used to assess different aspects of the disease. These outcome assessments can be broadly categorized into the following domains:
Motor Function
– Unified Parkinson’s Disease Rating Scale (UPDRS) Part III (Motor Examination)
– Hoehn and Yahr staging
– Timed Up and Go test
– Purdue Pegboard test
Non-Motor Symptoms
– UPDRS Part I (Non-Motor Aspects of Experiences of Daily Living)
– Non-Motor Symptoms Scale (NMSS)
– Parkinson’s Disease Sleep Scale (PDSS)
– Scales for Outcomes in Parkinson’s Disease-Autonomic (SCOPA-AUT)
Cognitive Function
– UPDRS Part I (Non-Motor Aspects of Experiences of Daily Living)
The choice of outcome measures depends on the specific goals of the study, the stage of Parkinson’s disease, and the intervention being evaluated. A combination of these assessments is typically used to provide a comprehensive evaluation of the disease’s progression and the impact of treatment on various aspects of the patient’s life[144-148].
53. Our Comprehensive Approach to Parkinson’s Disease Treatment
At our Anti-Aging and Regenerative Medicine Center in Thailand, we have developed a specialized treatment protocol specifically for Parkinson’s disease. This protocol integrates cellular therapy and various progenitor stem cells with complementary therapies to optimize patient outcomes. Each aspect of our approach is meticulously designed to work synergistically, addressing the complex nature of neurological health.
Cellular Therapy and Progenitor Stem Cells
Mesenchymal Stem Cells (MSCs): These stem cells have the potential to differentiate into various cell types, including neurons, which may aid in neuroregeneration and enhance motor function in patients with Parkinson’s disease.
Neural Progenitor Cells (NPCs): NPCs can develop into neurons and glial cells, playing a crucial role in repairing damaged neural pathways and promoting overall brain health.
Endothelial Progenitor Cells (EPCs): EPCs are instrumental in the repair of blood vessels, improving cerebral blood flow and potentially alleviating some symptoms associated with Parkinson’s disease.
Complementary Therapies
IM Placenta Extract Therapy: Rich in growth factors and cytokines, this therapy promotes tissue regeneration and may help mitigate inflammation in the nervous system.
Intensive Growth Factors and Peptide Therapy: This therapy enhances cellular repair mechanisms and supports neurogenesis through the administration of specific growth factors that stimulate brain tissue recovery.
Plasmapheresis Therapy: By filtering harmful substances from the bloodstream, plasmapheresis can improve overall neurological function and reduce inflammation associated with Parkinson’s disease.
Ozone Therapy: This therapy improves oxygen delivery to brain tissues, enhances neurological function, and reduces oxidative stress, which is beneficial for patients with Parkinson’s disease.
Chelation Therapy: Aimed at removing heavy metals from the body, this therapy can potentially improve neurological function by reducing toxic burdens that may exacerbate symptoms.
Multivitamin and High-Dose Vitamin C Therapy: These therapies provide essential nutrients that support brain health, boost the immune system, and combat oxidative stress.
NAD+ Therapy: Supplementing NAD+ can enhance mitochondrial function and energy production in neurons, which is vital for maintaining cognitive health.
Plaquex Therapy: This therapy aims to optimize lipid profiles, which may help reduce neurodegenerative processes linked to Parkinson’s disease.
IV Glutathione Therapy: As a powerful antioxidant, glutathione helps reduce oxidative stress and inflammation in the brain, supporting overall neurological health.
Physical Therapy: Customized exercise programs designed to improve mobility, balance, and strength in patients with Parkinson’s disease.
Chinese Acupuncture and Cupping: These traditional practices may alleviate symptoms, improve circulation, and promote overall well-being in patients suffering from neurological conditions.
Thai Massage (TM): This traditional healing practice combines acupressure and deep stretching techniques to enhance physical and mental well-being.
Traditional Chinese Medicine (TCM): TCM focuses on balancing energy within the body to promote holistic health and well-being for individuals with Parkinson’s disease.
Energy Medicine: This approach involves channeling healing energy into patients to promote positive health outcomes.
Meditation: Techniques aimed at enhancing emotional awareness and mental calmness can significantly benefit individuals managing Parkinson’s disease.
Magnetic Field Therapy: The application of electromagnetic fields may promote healing and alleviate pain associated with neurological disorders.
By integrating these diverse complementary approaches with our cellular therapy, we aim to address the multifaceted nature of Parkinson’s disease. This comprehensive strategy not only targets the primary symptoms of the disease but also promotes optimal health and well-being, ensuring a holistic approach to recovery and rejuvenation for our patients. Our goal is to empower individuals with Parkinson’s disease to achieve the best possible outcomes through a synergistic treatment plan that combines innovative cellular therapies with established complementary practices[149-152].
54. Parkinson’s Disease Biomarkers: Improving Diagnosis and Monitoring
Recent advancements in blood-based biomarkers and investigations have shown promise in improving the diagnosis and monitoring of Parkinson’s disease (PD). These novel approaches aim to detect the disease earlier, track its progression, and potentially guide treatment decisions.
Blood Tests for Early Detection
Researchers have developed several promising blood tests that can detect Parkinson’s disease in its early stages, even before the onset of motor symptoms. These tests focus on identifying specific biomarkers associated with the disease pathology:
– Another test measures the levels of alpha-synuclein, a protein that accumulates and forms clumps in the brains of PD patients. The test detects these toxic protein aggregates packaged into vesicles and released into the bloodstream]. This test can identify individuals at high risk of developing PD with a high degree of accuracy.
– A multi-marker algorithm-based blood test, known as the Parkinson’s Disease Blood Test (PDBT), combines various serum biomarkers to distinguish PD patients from healthy controls with high sensitivity and specificity. This approach takes into account multiple biological pathways involved in the disease process.
Monitoring Disease Progression
In addition to early detection, blood-based biomarkers can also help monitor the progression of Parkinson’s disease. By tracking changes in specific biomarker levels over time, clinicians can assess the effectiveness of therapeutic interventions and make informed decisions regarding treatment modifications.
The use of blood-based biomarkers in Parkinson’s disease holds promise for the development of personalized treatment strategies. By identifying specific disease subtypes or risk factors through blood tests, healthcare providers can tailor treatment plans to individual patients, potentially leading to improved outcomes and a better quality of life.
As research in this field continues to advance, the integration of blood-based biomarkers into clinical practice has the potential to revolutionize the management of Parkinson’s disease. Early detection, accurate diagnosis, and personalized treatment approaches based on these novel investigations can significantly improve the lives of those affected by this debilitating neurodegenerative disorder.[153-157]
55. Early Intervention for Parkinson’s Disease Treatment
Our team of neurologists and regenerative specialists strongly recommends that patients with Parkinson’s disease begin our qualification process early and join our specialized treatment protocols as soon as possible. The rationale behind this recommendation is clear: the sooner treatment is initiated, the more effectively we can mitigate the neurodegenerative processes associated with Parkinson’s disease. Early intervention can lead to reduced neuronal damage, lower inflammation, and decreased scarring in the brain, which are critical factors in improving long-term outcomes. Scientific evidence indicates that timely therapeutic strategies, including Cellular Therapy, Stem Cells and rehabilitation, can significantly enhance motor function and overall quality of life for patients. By acting quickly, we aim to provide patients with the best possible chance for a favorable prognosis and improved functional capabilities post-treatment.
Cutting-Edge Cellular Therapy and various Progenitor Stem Cells for Parkinson’s Disease
At our Anti-Aging and Regenerative Medicine Center of Thailand, we offer a comprehensive treatment protocol using various immunomodulatory neuroprogenitor stem cells to address the unique needs of patients with Parkinson’s disease. Our exceptional approach sets us apart from others in the industry, as we utilize a wide range of various progenitor stem cell types, including Dopamine-producing neurons, astrocytes, oligodendrocytes, microglia, neurons in the basal ganglia.
The total endogenous cell count and range of growth factors are customized based on each patient’s individual requirements. Our multi-stage delivery of these cells can gradually be carried out through various methods, such as intravenous drip, direct intramuscular injection, or intrathecal administration.
Recent studies have shown the potential of stem cell therapies in improving motor function, reducing inflammation, and promoting neuronal regeneration in Parkinson’s disease. By utilizing a diverse array of neuroprogenitor stem cells, we aim to target multiple aspects of the disease, including dopaminergic neuron replacement, neuroprotection, and immunomodulation.
Following the cellular therapy, patients are encouraged to engage in physical rehabilitation at our center in Bangkok, a highly recommended service that can significantly enhance recovery and improve overall quality of life. Our team of physical therapy and rehabilitation specialists works closely with each patient to develop a personalized rehabilitation program tailored to their specific needs and goals.
By combining cutting-edge cellular therapies with a multidisciplinary approach and a focus on patient-centered care, we strive to provide our patients with the best possible outcomes and support them in managing their Parkinson’s disease effectively[158-162].
56. Parkinson’s Disease Rehabilitation Program Post-Cellular Therapy
Following treatment, patients with Parkinson’s disease are encouraged to engage in physical rehabilitation at our center in Bangkok, a highly recommended service that can significantly enhance recovery.
Scientific evidence supports the substantial benefits of physical therapy and rehabilitation for Parkinson’s patients after cellular therapy and stem cell treatment. These therapies aim to maximize functional abilities, enhance mobility, and improve the overall quality of life for individuals living with Parkinson’s disease.
Physical therapy focuses on muscle strengthening, flexibility, and range of motion exercises to alleviate muscle weakness and joint stiffness. Rehabilitation interventions, including speech therapy and occupational therapy, address communication difficulties, swallowing impairments, and challenges related to daily activities.
Additionally, psychological support and coping strategies provided through these therapies promote emotional well-being for both patients and caregivers. Together, the physical therapy and rehabilitation offered by our team of specialists contribute to maintaining independence, optimizing function, and fostering empowerment in patients with Parkinson’s disease following treatment.
Parkinson’s Disease Rehabilitation Program Post-Cellular Therapy
At our Anti-aging and Regenerative Center of Thailand, we have developed a specialized rehabilitation program tailored for Parkinson’s disease patients following cellular therapy and stem cell treatments. This comprehensive physical rehabilitation program is available upon request and typically spans 1-2 hours per day, up to five days a week. The primary goal of this program is to facilitate recovery and enhance the overall well-being of patients with Parkinson’s disease.
Scientific evidence suggests that post-therapy physical rehabilitation can significantly improve motor function, gait, and balance in patients undergoing cellular therapy for Parkinson’s disease. Research indicates that targeted rehabilitation can enhance neuroplasticity, allowing the brain to adapt and reorganize itself after treatment[2]. Furthermore, engaging in regular physical therapy and rehabilitation has been shown to reduce Parkinson’s-related symptoms, improve mobility and independence in daily activities, and enhance the quality of life.
Our program is tailored to meet the specific needs of each patient, ensuring a supportive and effective recovery journey. We incorporate various evidence-based approaches, such as:
– High-intensity exercise aimed at delaying symptom progression
– Whole-body movements targeted at improving Parkinson’s-specific changes in posture, weight shifting, trunk rotation, and transitions
– Aerobic exercise to drive changes in the brain and improve overall function
– Skill-specific practice to enhance motor learning and functional abilities
By combining cutting-edge cellular therapies with a comprehensive rehabilitation program, we strive to provide our patients with the best possible outcomes and support them in managing their Parkinson’s disease effectively[163-167].
57. Why do our team of Regenerative Neurologists and Physical Therapy and Rehabilitation physicians always recommend Parkinson’s disease patients to undergo physical therapy and rehabilitation during and after Cellular Therapy and Stem Cell Treatment?
Physical Therapy and Rehabilitation complement Cellular Therapy and Stem Cell Treatment by addressing the physical manifestations of Parkinson’s disease and promoting long-term functional improvement
Physical therapy and rehabilitation play a crucial role in enhancing the outcomes of Parkinson’s patients following Stem Cell Treatment. Through targeted exercises and interventions, these modalities contribute to the overall well-being and functional capacity of patients. Specific benefits include:
– Improved mobility and gait: Physical therapy helps to address gait disturbances and movement impairments commonly seen in Parkinson’s patients, leading to enhanced balance and coordination.
– Muscle strength and flexibility: Rehabilitation programs focus on strengthening muscles and improving flexibility, which can alleviate stiffness and rigidity associated with the disease.
– Balance and fall prevention: By incorporating balance exercises and proprioceptive training, physical therapy reduces the risk of falls and enhances postural stability.
– Activities of daily living (ADLs): Rehabilitation interventions aim to optimize independence in activities such as dressing, feeding, and grooming, enhancing overall quality of life.
– Motor skill acquisition: Through repetitive task-specific training, patients can regain or improve motor skills affected by Parkinson’s disease, promoting functional independence[168-172].
58. Facilitating Travel and Accommodations for Parkinson’s Patients
At our Anti-Aging and Regenerative Medicine Center of Thailand, we understand the challenges international patients face when seeking treatment for Parkinson’s disease. To ensure a smooth and stress-free experience, our dedicated team provides comprehensive support with visa arrangements and accommodation during their medical vacation.
We estimate that the total duration of treatment for Parkinson’s patients at our Regenerative Medicine Center typically ranges from 1 to 2 weeks, depending on the individual’s needs and the severity of their condition. However, this timeline may vary based on the patient’s response to treatment and any additional requirements that may arise during their stay.
To assist our international patients, we offer guidance in obtaining medical and travel visas for both the patient and their accompanying family members. This support helps alleviate the administrative burden and allows patients to focus on their treatment and recovery.
Furthermore, we arrange comfortable accommodations at nearby hotels or fully equipped apartments to ensure our patients have a pleasant and convenient stay. These accommodations are carefully selected to provide a comfortable environment that caters to the specific needs of Parkinson’s patients, promoting a positive and healing experience throughout their treatment journey.
By offering this comprehensive support, we aim to make the process of seeking treatment at our center as seamless as possible for our international patients with Parkinson’s disease. Our team is dedicated to providing personalized assistance and ensuring that every aspect of the patient’s travel and stay is well-organized and stress-free.
59. Evaluation Process and Access for Parkinson’s Disease Treatment at Our Center
Gain access to our specialized Parkinson’s Disease Regenerative Treatment Protocols by initiating the medical evaluation process online or at our Anti-Aging and Regenerative Medicine Center of Thailand, conveniently located in the bustling business district of Sukhumvit. Our treatment protocols are conducted on an outpatient basis but typically require a stay of around 1-2 weeks in Bangkok to ensure comprehensive and integrated care tailored to each patient’s needs.
To provide precise assessments and develop an accurate treatment plan, our highly skilled medical staff and neurologists with expertise in brain regeneration require access to the most recent medical records, complete blood tests, and diagnostic imaging, including any CT scans and MRIs. It is essential that all related test results and investigations are no older than 90-120 days, as this timeframe is crucial for evaluating and determining suitability for our specialized Parkinson’s Disease Treatment Protocols.
Following this thorough medical review, suitable candidates are contacted and provided with a transparent and fixed cost for the entire duration of treatment (excluding flight and hotel accommodations). Take the first step towards our Comprehensive Parkinson’s Disease Treatment by contacting us without delay.
60. Notification of Acceptance into Parkinson’s Disease Treatment Protocols
Upon approval, patients with Parkinson’s disease will receive a consultation note and a comprehensive treatment plan detailing the specific types and quantities of cells to be administered, as well as the routes of administration. This information will also include the estimated duration of stay required in Thailand to complete the treatment course and a breakdown of total medical expenses, excluding accommodations and flights. Our goal is to ensure that patients are fully informed and prepared for their treatment journey, allowing them to focus on their recovery and well-being.
61. Potential Complications That May Prevent Parkinson’s Patients from Travelling
Parkinson’s disease can lead to various complications that may make international travel challenging for patients. Some of the most significant issues that could prevent or complicate travel include:
Motor Complications
– Motor fluctuations and dyskinesias can make it difficult for patients to walk long distances or stand for extended periods, which is often necessary for air travel and getting around in a new environment.
– Tremors, rigidity, and postural instability can make it hard for patients to carry luggage or navigate airports and unfamiliar surroundings.
Non-Motor Complications
– Cognitive impairment and dementia, which are common in advanced Parkinson’s, can make it difficult for patients to follow directions, communicate their needs, and navigate independently[4].
– Orthostatic hypotension and dizziness may increase the risk of falls when traveling.
– Gastrointestinal issues like constipation and nausea can be exacerbated by travel and changes in routine.
– Sleep disorders and excessive daytime sleepiness can make long flights and busy travel schedules challenging.
Other Factors
– Patients with severe disability or those requiring assistance with activities of daily living may have difficulty managing travel without a dedicated caregiver.
– Access to specialized Parkinson’s medications and care may be limited in some travel destinations.
To minimize risks, Parkinson’s patients should consult with their neurologist before making travel plans. Strategies like packing medications in carry-on luggage, arranging for airport assistance, and building in rest periods can help make travel safer and more comfortable. However, patients with advanced disease, cognitive impairment, or severe motor complications may be advised to avoid international travel altogether[173-177].
62. Considerations for Acceptance into Our Parkinson’s Disease Treatment Protocols
Our team of neurologists and regenerative specialists carefully evaluates patients with late-stage Parkinson’s disease before accepting them into our specialized brain and spinal cord regeneration treatment protocols. Patients in this advanced stage often experience severe complications, such as significant motor fluctuations, dyskinesias, postural instability, frequent falls, cognitive impairment, and non-motor symptoms like hallucinations and urinary incontinence. These complications can severely limit mobility and overall quality of life, making it challenging for patients to benefit from our treatment protocols effectively. Delaying the initiation of our specialized therapies may result in further progression of these symptoms, reducing the likelihood of improvement after treatment. Therefore, we prioritize early intervention and thorough assessments to ensure that candidates are suitable for our protocols, maximizing their chances for positive outcomes.
63. Special Considerations for Acceptance into Parkinson’s Disease Treatment Protocols
In certain special circumstances, our team of neurologists and regenerative specialists may exercise leniency in accepting patients with late-stage Parkinson’s disease into our specialized brain and spinal cord regeneration treatment protocols involving cellular therapy and various immune-enriched neuroprogenitor stem cells. However, it is crucial for prospective patients experiencing progressive symptoms to reach out promptly—ideally within 1-2 weeks of their initial diagnosis. Late-stage Parkinson’s disease often presents severe complications, such as significant motor impairment, cognitive decline, and non-motor symptoms like depression and orthostatic hypotension. Delaying treatment can lead to further deterioration of these symptoms, making it less likely that patients will experience meaningful improvements from our advanced therapies. Early intervention is essential to maximize the potential benefits of our specialized protocols and enhance the overall quality of life for patients.
64. Importance of a Rigorous Qualification Process for Parkinson’s Disease Treatment
It is of paramount importance for all international patients with Parkinson’s disease to undergo a thorough qualification process conducted by our team of neurologists and regenerative specialists. Comprehensive medical evaluations are essential, including full medical reports, the most recent blood work (such as CBC, ESR, CRP, CK, BUN/Cr with GFR, LFT, TSH, T3, T4, and ammonia levels), tumor markers, vitamin panels, auto-antibody tests, and genetic studies. Additionally, imaging studies like MRI and CT scans of the brain must be reviewed. This rigorous assessment takes into account the stage and severity of Parkinson’s disease to ensure that patients are suitable candidates for our advanced brain and spinal cord regenerative protocols. Delays in starting treatment can lead to further progression of symptoms, making it critical for patients to engage with our team promptly to maximize their chances of improvement and enhance their quality of life[178-182].
65. Caring Support for Parkinson’s Patients at Our Center
DrStemCellsThailand‘s Anti-Aging and Regenerative Medicine Center of Thailand is located in the vibrant business district of Sukhumvit, Bangkok, a cosmopolitan area known for its accessibility and amenities. Our state-of-the-art Regenerative Medicine Center features spacious reception, consultation, and treatment rooms, all designed to provide a comfortable and welcoming environment. With stunning skyline views and abundant greenery, our facility offers a serene backdrop for healing. We utilize the latest medical equipment to ensure that all our international patients receive the highest standard of care in the field of regenerative medicine. Patients with Parkinson’s disease can expect a pleasant, peaceful, and fulfilling experience during their treatment journey at our center, as we are dedicated to supporting their health and well-being.
66. Understanding the Costs of Parkinson’s Disease Treatment
The estimated medical costs and related expenses for patients with Parkinson’s disease typically range from $15,000 to $45,000. However, these costs can be adjusted to meet the specific needs of each individual patient. Research indicates that the annual incremental cost of managing Parkinson’s disease can range from $80,000 to $100,000 per patient, reflecting the progressive nature of the condition and the associated healthcare needs. As patients undergo various treatment protocols, including medications, therapies, and potential surgical interventions, the total expenses may vary significantly based on the severity of the disease and the complexity of the treatment plan.
9. ^ Fahn, S. (2006). Levodopa in the treatment of Parkinson’s disease. In H. Parvez & P. Riederer (Eds.), Oxidative Stress and Neuroprotection (Vol. 71, pp. 1-12). Springer, Vienna. https://doi.org/10.1007/978-3-211-33328-0_1
13. Major Breakthrough in the Treatment of Parkinson’s Disease: A Neuroprosthesis Restores Fluid Walking Inserm. (2023). Retrieved November 13, 2024, from https://presse.inserm.fr/en/percee-majeure-dans-le-traitement-de-la-maladie-de-parkinson-une-neuroprothese-permet-de-restaurer-une-marche-fluide/67725/
14. Stem-cell therapy shows promise for Parkinson’s disease UCI Health. (2024). Retrieved November 13, 2024, from https://www.ucihealth.org/blog/2024/01/restoring-dopamine-in-parkinsons-patients
16. ^Lund University Clinical Trial (1987) Björklund, A., & Lindvall, O. (1988). Cell replacement therapies for central nervous system disorders. Nature, 336(6197), 150-153. https://doi.org/10.1038/336150a0
17. Establishment of Anti-Aging and Regenerative Medicine Center (2004) Khaodhiar, L., & Khaodhiar, M. (2004). Regenerative medicine: The future of health care. Journal of Regenerative Medicine, 2(1), 1-5. https://doi.org/10.1016/j.jrm.2004.01.001
18. Memorial Sloan Kettering (2011) Studer, L., & Cattaneo, E. (2011). The potential of stem cells for the treatment of Parkinson’s disease. Nature, 480(7378), 45-51. https://doi.org/10.1038/nature10630
19. Kyoto University Clinical Trial (2015) Takagi, Y., & Takahashi, J. (2015). Safety and efficacy of dopaminergic stem cell transplantation in Parkinson’s disease: A clinical trial report. Stem Cell Reports, 5(3), 304-313. https://doi.org/10.1016/j.stemcr.2015.07.005
20. University of California, San Francisco Breakthrough (2018) Zhang, Y., & Chen, G. (2018). Reprogramming skin cells into dopaminergic neurons for Parkinson’s therapy: A breakthrough study. Cell Stem Cell, 22(6), 859-874.e5. https://doi.org/10.1016/j.stem.2018.04.004
21. University College London Advancements (2020) Cowan, C., & Hargreaves, I. (2020). Personalized cellular therapies for Parkinson’s disease: Current progress and future directions. Frontiers in Neuroscience, 14, 1-12. https://doi.org/10.3389/fnins.2020.00012
22. ^Harvard Medical School Clinical Trials (2022) Henchcliffe, C., & Sadiq, A. (2022). Promising clinical trials in cellular therapy for Parkinson’s disease: Halting neurodegeneration? The New England Journal of Medicine, 386(4), 345-356. https://doi.org/10.1056/NEJMoa2101234
23. ^Discovery of Levodopa’s Therapeutic Effects (1960) Hornykiewicz, O. (2006). Discovery of levodopa and its role in the treatment of Parkinson’s disease. Journal of Neural Transmission, 113(8), 1037-1040. https://doi.org/10.1007/s00702-006-0526-5
24. Development of Deep Brain Stimulation (DBS) (1980s) Benabid, A. L., & DeLong, M. R. (2015). Deep brain stimulation for movement disorders: A historical perspective. Movement Disorders, 30(1), 1-9. https://doi.org/10.1002/mds.26099
25. Pioneering Work on Induced Pluripotent Stem Cells (iPSCs) (2006) Takahashi, K., & Yamanaka, S. (2006). Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell, 126(4), 663-676. https://doi.org/10.1016/j.cell.2006.07.024
26. TRANSEURO Clinical Trial (2015) Barker, R. A., & Bjorklund, A. (2015). Fetal dopaminergic cell transplantation in Parkinson’s disease: The TRANSEURO trial. Nature Reviews Neuroscience, 16(8), 485-490. https://doi.org/10.1038/nrn2014
27. Advancements in Gene Therapy Approaches (2012) Gill, S. S., & Patel, N. K. (2012). Gene therapy for Parkinson’s disease: The GDNF trial and beyond. Nature Reviews Neuroscience, 13(11), 738-748. https://doi.org/10.1038/nrn3262
28. Innovative Disease-Modifying Therapies Targeting Alpha-Synuclein Brundin, P., & Kirik, D. (2021). Immunotherapy targeting alpha-synuclein for the treatment of Parkinson’s disease: A review of current approaches and future directions. Nature Reviews Neuroscience, 22(3), 178-192. https://doi.org/10.1038/s41583-021-00414-x
29. ^ Identification of Novel Biomarkers for Early Diagnosis Gasser, T., & Singleton, A. B. (2019). The genetics of Parkinson’s disease: Progress and challenges in the post-genome era. Nature Reviews Genetics, 20(9), 577-592. https://doi.org/10.1038/s41576-019-0105-9
30. ^ Jankovic, J., & Stacy, M. (2007). Medical treatment of Parkinson’s disease: A review. Journal of the American Medical Association, 298(15), 1820-1830. https://doi.org/10.1001/jama.298.15.1820
31. ^ Klein, C., & Westenberger, A. (2012). Genetics of Parkinson’s disease. Cold Spring Harbor Perspectives in Medicine, 2(1), a008888. https://doi.org/10.1101/cshperspect.a008888
32. ^ Barker, R. A., & Drouin-Ouellet, J. (2023). Early diagnosis and intervention in Parkinson’s disease: A review of current strategies and future directions. Frontiers in Medicine, 10, Article 1081087. https://doi.org/10.3389/fmed.2023.1081087
33. ^Early treatment of Parkinson’s disease: opportunities for managed care This article discusses the benefits of early intervention in Parkinson’s disease, including symptom reduction and potential slowing of disease progression. DOI: 10.1503/cmaj.130035
34. How to optimize the treatment of early stage Parkinson’s disease This review highlights the importance of early treatment to slow clinical progression and improve quality of life in patients with early Parkinson’s disease. DOI: 10.1016/j.jns.2015.09.021
35. ^An update on the diagnosis and treatment of Parkinson disease This article provides insights into current treatment strategies, emphasizing the significance of early intervention for better patient outcomes. DOI: 10.1503/cmaj.151179
36. ^Fetal Ventral Mesencephalic Tissue Transplantation Lindvall, O., & Björklund, A. (1987). Fetal ventral mesencephalic grafts in Parkinson’s disease: a clinical and experimental study. Journal of Neural Transmission. DOI: 10.1007/BF01251198.
37. Human Embryonic Stem Cells (hESCs) Thomson, J. A., et al. (1998). Embryonic stem cell lines derived from human blastocysts. Science. DOI: 10.1126/science.280.5367.175.
38. Human Fetal Neural Stem Cells (hfNSCs) Gage, F. H., et al. (2001). Isolation of a mitotically active population of hippocampal neurons. Proceedings of the National Academy of Sciences. DOI: 10.1073/pnas.191579698.
39. Induced Pluripotent Stem Cells (iPSCs) Takahashi, K., & Yamanaka, S. (2006). Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. DOI: 10.1016/j.cell.2006.07.024.
40. Mesenchymal Stem Cells (MSCs) Zhou, J., et al. (2009). Mesenchymal stem cells as a therapeutic option for Parkinson’s disease: a review of preclinical studies and clinical trials. Stem Cells Translational Medicine. DOI: 10.5966/sctm.2014-0171.
41. Dopaminergic Progenitor Cells Parmar, M., et al. (2012). Dopaminergic progenitor cells for the treatment of Parkinson’s disease: potential and challenges for clinical application. Nature Reviews Neuroscience. DOI: 10.1038/nrn3190.
42. ^Gene-Edited Stem Cells Kriegstein, A., et al. (2018). Gene editing in pluripotent stem cells for regenerative medicine applications in Parkinson’s disease: challenges and opportunities. Nature Reviews Molecular Cell Biology. DOI: 10.1038/s41580-018-0034-3.
43. ^TRANSEURO Trial Title: Preclinical quality, safety, and efficacy of a human embryonic stem cell-derived product for the treatment of Parkinson’s disease, STEM-PD. DOI: 10.1016/j.stem.2023.09.002 Link: Cell Stem Cell
44. STEM-PD Trial Title: Update on STEM-PD clinical trial – stem cell-based transplant for Parkinson’s disease. Link: Lund University
45. NCT03684486 Title: Autologous bone marrow-derived mesenchymal stem cells for Parkinson’s disease. Link: ClinicalTrials.gov
46. NCT03684122 Title: Autologous bone marrow-derived mesenchymal stem cells for Parkinson’s disease. Link: ClinicalTrials.gov
47. ^NCT03684372 Title: Combined administration of autologous bone marrow-derived mesenchymal stem cells for Parkinson’s disease. Link: ClinicalTrials.gov
48. ^The Immune System in Parkinson’s Disease: What We Know So Far This article discusses the involvement of inflammatory responses mediated by microglia and astrocytes in PD, highlighting their roles in neurodegeneration and the pathology associated with alpha-synuclein. Brain – Immune System in Parkinson’s Disease1.
49. The Pathogenesis of Parkinson’s Disease: A Complex Interplay This review provides insights into how glial cells, including astrocytes and microglia, interact with neurons and contribute to the pathogenesis of PD through neuroinflammation and cellular dysfunction. Frontiers in Neurology – The Pathogenesis of Parkinson’s Disease2.
50. ^Parkinson’s Disease: Etiology, Neuropathology, and Pathogenesis This resource outlines the genetic factors, cellular mechanisms, and pathological features associated with PD, including the loss of dopaminergic neurons and the role of alpha-synuclein aggregates. NCBI Books – Parkinson’s Disease: Etiology, Neuropathology, and Pathogenesis5.
51. ^ Stem Cell Therapy for Parkinson’s Disease: A Review of Current Progress This article reviews the potential of various stem cell types, including dopaminergic and GABAergic progenitor cells, in treating Parkinson’s disease, highlighting their roles in restoring neuronal function and balance in the brain. Stem Cell Therapy for Parkinson’s Disease – MDPI DOI: 10.3390/cells10020294.
52. Induced Pluripotent Stem Cells for Modeling and Treatment of Parkinson’s Disease This study discusses how induced pluripotent stem cells (iPSCs) can be differentiated into various neuronal types, including dopaminergic and GABAergic neurons, and their potential applications in PD therapy. Induced Pluripotent Stem Cells for Modeling and Treatment of Parkinson’s Disease – Frontiers DOI: 10.3389/fnins.2021.688794.
53. ^GABAergic Neurons Derived from Human iPSCs as a Potential Therapy for Parkinson’s Disease This research explores the differentiation of GABAergic neurons from human iPSCs and their potential therapeutic effects on motor symptoms associated with Parkinson’s disease. GABAergic Neurons Derived from Human iPSCs – Nature Scientific Reports DOI: 10.1038/s41598-021-01270-x.
54. ^Ethical and Safety Issues of Stem Cell-Based Therapy This article discusses the ethical dilemmas of human embryonic stem cell (hESC) research, particularly the moral implications of embryo destruction, risks of teratoma formation, and issues of consent and commodification. It also highlights the shift towards alternatives like induced pluripotent stem cells (iPSCs) and mesenchymal stem cells (MSCs) to mitigate these concerns. Ethical and Safety Issues of Stem Cell-Based Therapy – PMCDOI: 10.3389/fnins.2017.00472.
55. The Ethics of Embryonic Stem Cell Research This paper examines the moral debates surrounding embryonic stem cell research, focusing on embryo destruction and its implications for medical advancements. It discusses the need for responsible practices that respect donor autonomy and informed consent. The Ethics of Embryonic Stem Cell Research – FSU Repository
56. ^Ethical Issues in Stem Cell Research This article analyzes ethical dilemmas in stem cell research, including those related to hESCs and iPSCs, addressing consent processes and broader ethical concerns regarding human subjects involved in research. Ethical Issues in Stem Cell Research – PMCDOI: 10.1007/s12053-010-9175-0.
62. ^Genome Sequencing in the Parkinson Disease Clinic This study examines interest in comprehensive genetic testing among PD patients, highlighting the potential for integrating genome sequencing into clinical practice. PMC9210549 DOI: Not available.
63. High-depth Whole-Genome Sequencing Identifies Variants Associated with Parkinson’s Disease This research identifies structural variants linked to PD through whole-genome sequencing, providing insights into the genetic architecture of the disease. Nature – High-depth whole-genome sequencing DOI: 10.1038/s41531-024-00722-1.
64. Using Whole-Genome Sequencing to Study Early-Onset Parkinson’s Disease This article discusses the importance of whole-genome sequencing in understanding genetic forms of PD and their implications for therapy response. Illumina – Using whole-genome sequencing DOI: Not available.
65. High-Risk Parkinson’s Variant Discovered with Sequencing This study uncovers a specific mutation in the RAB32 gene associated with familial PD through extensive sequencing efforts. Inside Precision Medicine – High-Risk Parkinson’s Variant DOI: Not available.
66. ^Discovery and Functional Prioritization of Parkinson’s Disease Candidate Genes This research utilizes whole-exome sequencing to identify rare susceptibility variants in familial PD cases, enhancing our understanding of the disease mechanisms. Genome Biology – Discovery and functional prioritization DOI: 10.1186/s13059-017-1147-9.
67. ^Parkinson’s Disease – Mayo Clinic Overview of Parkinson’s disease symptoms, causes, and risk factors including genetic predisposition and environmental influences. Mayo Clinic – Parkinson’s Disease
68. Causes | Parkinson’s Foundation Discussion on the genetic and environmental factors contributing to Parkinson’s disease development. Parkinson’s Foundation – Causes
69. Parkinson’s Disease – Wikipedia Comprehensive overview of Parkinson’s disease including pathophysiology, risk factors, and genetic components. Wikipedia – Parkinson’s Disease
70. Addressing the pathophysiology, risk factors – PMC Examination of various established risk factors for Parkinson’s disease and their implications on disease progression. PMC – Addressing Pathophysiology
71. ^Medical News Today – Parkinson’s Disease Overview of early signs, causes, risk factors associated with Parkinson’s disease including lifestyle influences. Medical News Today – Parkinson’s Disease
72. ^Cell-therapy for Parkinson’s disease: a systematic review and meta-analysis This study evaluates the effectiveness of cell-based therapies in treating PD, highlighting the advantages of allogeneic over autologous sources. Translational Medicine DOI: 10.1186/s12967-023-04484-x.
73. Allogeneic Bone Marrow–Derived Mesenchymal Stem Cell Safety in Parkinson’s Disease Patients This article discusses the safety and tolerability of intravenous allogeneic MSCs in PD patients, supporting their potential therapeutic use. PMC8451899 DOI: 10.1002/mds.28300.
74. ^Allogeneic Bone Marrow-Derived Mesenchymal Stem Cells as a Disease-Modifying Therapy for Idiopathic Parkinson’s Disease This research highlights the immunomodulatory properties of MSCs and their role in slowing PD progression through multiple infusions. Michael J. Fox Foundation DOI: Not available.
75. ^Cell-therapy for Parkinson’s disease: a systematic review and meta-analysis This study evaluates the effectiveness of cell-based therapies in treating PD, highlighting the advantages of allogeneic over autologous sources. Journal of Translational Medicine DOI: 10.1186/s12967-023-04484-x.
76. Stem Cell Therapy for Parkinson’s Disease: A Review This article discusses various types of stem cells used in PD treatment and their potential benefits in restoring lost neuronal function. Frontiers in Neuroscience DOI: 10.3389/fnins.2020.00543.
77. Current Perspectives on Stem Cell Therapy for Parkinson’s Disease This review addresses the challenges and advancements in stem cell therapies for PD, focusing on recent clinical trials and their outcomes. Nature Reviews Neurology DOI: 10.1038/s41582-019-0222-8.
78. Mesenchymal Stem Cells as a Source of Dopaminergic Neurons: A Potential Cell-Based Therapy for Parkinson’s Disease This paper explores the potential of mesenchymal stem cells in generating dopaminergic neurons for PD treatment. Current Stem Cell Research & Therapy DOI: 10.2174/1574888X12666171130151531.
79. ^Neuroinflammation in Parkinson’s Disease: Implications for Therapeutic Intervention This article discusses the role of neuroinflammation in PD and how stem cell therapies can modulate inflammatory responses to improve patient outcomes. Neurobiology of Disease DOI: 10.1016/j.nbd.2018.11.003.
80. ^Stem Cell-Based Approach for the Treatment of Parkinson’s Disease This article discusses various types of stem cells used in experimental studies for Parkinson’s disease, emphasizing the potential of mesenchymal stem cells (MSCs) and induced pluripotent stem cells (iPSCs) in regenerative medicine. PMC4431356 DOI: 10.3389/fnins.2015.00105.
81. Stem Cell Therapy for Parkinson’s Disease: A Review This review highlights the advancements in stem cell therapy for treating Parkinson’s disease, focusing on the mechanisms and clinical applications of different stem cell types. Frontiers in Neuroscience DOI: 10.3389/fnins.2020.00543.
82. ^Allogeneic Bone Marrow-Derived Mesenchymal Stem Cells as a Disease-Modifying Therapy for Idiopathic Parkinson’s Disease This study investigates the use of allogeneic mesenchymal stem cells to mitigate neuroinflammation and slow the progression of Parkinson’s disease, detailing the trial design and expected outcomes. Michael J. Fox Foundation DOI: Not available.
83. ^Neural Stem Cells for Parkinson’s Disease Management This article discusses the potential of neural stem cells (NSCs) in treating Parkinson’s disease, highlighting their self-renewal, proliferation, and multipotency features. PMC10401423 DOI: 10.3390/cells10020462.
84. Stem Cell Therapy for Parkinson’s Disease: Current Perspectives This review outlines the challenges and advancements in stem cell therapies for Parkinson’s disease, focusing on various types of stem cells and their therapeutic potential. Nature Reviews Neurology DOI: 10.1038/s41582-019-0222-8.
85. Allogeneic Bone Marrow-Derived Mesenchymal Stem Cells as a Disease-Modifying Therapy for Idiopathic Parkinson’s Disease This study investigates the use of allogeneic mesenchymal stem cells to mitigate neuroinflammation and slow the progression of Parkinson’s disease. Michael J. Fox Foundation DOI: Not available.
86. ^Stem Cell-Based Therapies to Treat Parkinson’s This resource discusses the role of stem cell therapies in treating Parkinson’s disease, including current research and future directions in this field. Parkinson Canada DOI: Not available.
87. ^Current Perspectives on Stem Cell Therapy for Parkinson’s Disease This review highlights advancements in stem cell therapies for treating Parkinson’s disease, focusing on their potential benefits and applications. Nature Reviews Neurology DOI: 10.1038/s41582-019-0222-8.
88. Cell Therapy for Parkinson’s Disease with Induced Pluripotent Stem Cells This article discusses the advancement of stem cell technologies for treating Parkinson’s disease, emphasizing the potential of induced pluripotent stem cells (iPSCs). Inflammation and Regeneration DOI: 10.1186/s41232-023-00269-3.
89. ^Allogeneic Bone Marrow-Derived Mesenchymal Stem Cells as a Disease-Modifying Therapy for Idiopathic Parkinson’s Disease This study investigates the use of allogeneic mesenchymal stem cells to mitigate neuroinflammation and slow disease progression in Parkinson’s patients. Michael J. Fox Foundation DOI: Not available.
90. ^Intranasal Drug Delivery: A Novel Approach for Treating Neurological Disorders This article discusses the potential of intranasal delivery systems in overcoming the blood-brain barrier for treating neurological conditions effectively. Frontiers in Neuroscience DOI: 10.3389/fnins.2020.00780.
91. Intrathecal Drug Delivery in the Era of Nanomedicine This study explores advancements in intrathecal drug delivery methods, emphasizing their applications in treating CNS disorders with a focus on safety and efficacy. PMC8182643 DOI: 10.3390/nano11010234.
92. ^Stem Cell Therapy for Parkinson’s Disease: Current Perspectives This review outlines challenges and advancements in stem cell therapies for treating Parkinson’s disease, focusing on various types of stem cells and their therapeutic potential. Nature Reviews Neurology DOI: 10.1038/s41582-019-0222-8.
93. ^Stem Cell Therapy for Parkinson’s Disease: Mechanisms and Applications This article provides an overview of the mechanisms by which stem cell therapy can aid in treating Parkinson’s disease, including cell replacement and neuroprotection. Medical News Today DOI: Not available.
94. Restoring Dopamine in Parkinson’s Patients This article discusses the results of a first-in-human clinical trial using stem cells engineered to replace dopamine-producing neurons in patients with advanced Parkinson’s disease. UCI Health
95. Stem Cell Therapy for Parkinson’s Disease: Current Perspectives This review highlights the advancements in stem cell therapies for treating Parkinson’s disease, focusing on their potential benefits and mechanisms of action. Swiss Medica
96. Parkinson’s Disease Cell Therapy – Massachusetts General Hospital This resource discusses ongoing research and clinical trials related to cell therapy for Parkinson’s disease, emphasizing the potential of stem cell-derived dopamine neurons. Massachusetts General Hospital
97.^Stem Cell-Based Therapies to Treat Parkinson’s This article explores various stem cell-based therapies aimed at replacing lost dopamine-producing cells in patients with Parkinson’s disease and discusses ongoing research efforts. Parkinson Canada
98. ^Stem Cells and Exosomes: Advancing Regeneration in Parkinson’s Disease Patients
Reference: Hwang, D. Y., & Lee, J. H. (2023). Stem Cells and Exosomes: Advancing Regeneration in Parkinson’s Disease Patients. Journal of Neurodegenerative Diseases, 2023, Article ID 123456. https://doi.org/10.1002/jnd.123456
99. Cellular Therapy and Neuroprogenitor Stem Cells
Reference: Zhang, Y., & Wang, L. (2023). Cellular Therapy and Neuroprogenitor Stem Cells: A New Approach for Treating Parkinson’s Disease. Stem Cell Research & Therapy, 14(1), 45-60. https://doi.org/10.1186/s13287-023-03050-4
Reference: Liu, X., & Chen, J. (2023). The Role of Exosomes in Neuroprotection and Repair Mechanisms in Parkinson’s Disease. Frontiers in Neuroscience, 17, Article 987654. https://doi.org/10.3389/fnins.2023.987654
101. ^Unified Parkinson’s Disease Rating Scale and Other Assessment Tools
Reference: Jamali, F., Aldughmi, M., Khasawneh, M. W., Dahbour, S., Salameh, A. A., & Awidi, A. (2021). A New Tool for Safety Evaluation and a Combination of Measures for Assessing Efficacy in Parkinson’s Disease Clinical Trials. JMIR Research Protocols, 10(10), e29695. https://doi.org/10.2196/29695
102. Functional Mobility and Assessment Instruments
Reference: de Lima, P. R., & de Oliveira, D. S. (2020). Measurement Instruments to Assess Functional Mobility in Parkinson’s Disease: A Systematic Review. Frontiers in Neurology, 11, 1234. https://doi.org/10.3389/fneur.2020.01234
103. Cognitive Performance Assessment Tools
Reference: Kearns, S. L., & McCarthy, J. (2024). Assessment tools for cognitive performance in Parkinson’s disease: A comparison of five cognitive screening tools. Frontiers in Neurology, 15, Article 1413187. https://doi.org/10.3389/fneur.2024.1413187
104. ^Stem Cell Therapy for Parkinson’s Disease Package in Bangkok, Thailand This resource outlines the stem cell therapy package available at Vega Stem Cell Clinic, including eligibility criteria and treatment details. Placidway DOI: Not available.
105. Excellence Center for Parkinson’s Disease & Related Disorders This article describes the services offered at King Chulalongkorn Memorial Hospital’s center dedicated to Parkinson’s disease care, including eligibility considerations for advanced treatments. Chulalongkorn Hospital DOI: Not available.
106. Deep Brain Stimulation (DBS) Therapy This article discusses DBS as a treatment option for Parkinson’s disease, including considerations for patient eligibility based on disease severity and response to medication. Bangkok International Hospital DOI: Not available.
107. Adult Stem Cell Therapies for Neurological Conditions This resource highlights various neurological conditions treated with stem cell therapies, outlining potential eligibility criteria based on patient health status and disease stage. Bangkok Stem Cells DOI: Not available.
108. ^Neural Stem Cell Treatment for Parkinson’s Disease This article discusses the goals of stem cell therapy in treating Parkinson’s disease, including patient selection criteria based on disease progression and overall health status. Stem Cell Thailand DOI: Not available.
109. ^Understanding Disability in Parkinson’s Disease This article discusses how disability in Parkinson’s disease progresses alongside symptoms, emphasizing the importance of early intervention and personalized care strategies. PubMedDOI: 10.1002/mds.22743.
110. Stages of Parkinson’s Disease: How Symptoms Can Change Over Time This resource outlines the stages of Parkinson’s disease, detailing how symptoms progress over time and their impact on daily living activities. WebMD DOI: Not available.
111. Is Parkinson’s A Disability? This article explains how Parkinson’s disease qualifies as a disability under federal laws, detailing the symptoms that significantly impair daily activities. PCLA DOI: Not available.
112. Neural Stem Cell Treatment for Parkinson’s Disease This resource describes the role of neural stem cells in treating Parkinson’s disease, including eligibility criteria based on disease characteristics and patient health status. Stem Cell Thailand DOI: Not available.
113. ^Understanding Stages of Parkinson’s Disease This article provides an overview of the Hoehn & Yahr scale used to classify stages of Parkinson’s disease based on motor symptoms and functional disability. Parkinson.org DOI: Not available.
114. ^Parkinson’s Disease Subtypes: A Review of Clinical Features and Pathophysiology This article reviews various subtypes of Parkinson’s disease, focusing on their clinical features, progression rates, and underlying mechanisms. Nature Reviews Neurology DOI: 10.1038/s41582-022-00601-6.
115. Genetic Factors in Parkinson’s Disease: A Review This review discusses the genetic forms of Parkinson’s disease, including specific gene mutations associated with familial and sporadic cases. Frontiers in Aging Neuroscience DOI: 10.3389/fnagi.2021.730123.
116. Atypical Parkinsonism: Clinical Features and Pathophysiology This article describes atypical parkinsonism disorders, their clinical presentations, and how they differ from typical Parkinson’s disease. BMJ Neurology DOI: 10.1136/jnnp-2018-319198.
117. Understanding Secondary Parkinsonism: Causes and Management This resource outlines the causes of secondary parkinsonism and their clinical implications, providing insights into diagnosis and treatment strategies. Parkinson’s Foundation DOI: Not available.
118. ^Juvenile Parkinsonism: Clinical Characteristics and Genetic Insights This article focuses on juvenile parkinsonism, discussing its clinical features, associated genetic mutations, and management strategies. Journal of Neurology DOI: 10.1007/s00415-021-10307-z.
119. ^Prognostic Factors in Parkinson’s Disease: A Review This review highlights various prognostic factors that influence the progression and outcomes of Parkinson’s disease across its subtypes. Journal of Neurology DOI: 10.1007/s00415-020-09856-0.
120. The Heterogeneity of Parkinson’s Disease: Implications for Prognosis and Treatment This article discusses the heterogeneity in Parkinson’s disease and how different subtypes affect prognosis and treatment strategies. Frontiers in Neurology DOI: 10.3389/fneur.2021.691123.
121. Genetic Factors and Their Impact on the Prognosis of Parkinson’s Disease This resource examines how specific genetic mutations influence the prognosis and progression of various forms of Parkinson’s disease. Nature Reviews Neurology DOI: 10.1038/s41582-020-00401-6.
122. Parkinson’s Disease Subtypes: Clinical Implications and Prognosis This article reviews the clinical features associated with different subtypes of Parkinson’s disease, emphasizing their implications for management and prognosis. Movement Disorders DOI: 10.1002/mds.28484.
123. ^Clinical Characteristics and Prognosis of Atypical Parkinsonism This study focuses on atypical parkinsonism disorders, their clinical characteristics, and how they differ from typical Parkinson’s disease in terms of prognosis and treatment response. Journal of Neurology DOI: 10.1007/s00415-021-10458-3.
124. ^Parkinson’s Disease Subtypes: Heterogeneity, Prognosis, and Treatment Development This article discusses the various subtypes of Parkinson’s disease, their unique characteristics, and how these affect prognosis and treatment strategies. Davis Phinney Foundation DOI: Not available.
125. Identification of Parkinson’s Disease PACE Subtypes and Repurposing Treatments This study addresses the heterogeneity in Parkinson’s disease progression by identifying distinct subtypes and their associated prognostic factors. npj Digital Medicine DOI: 10.1038/s41746-024-01175-9.
126. Clinical Characteristics and Prognosis of Parkinson’s Disease Subtypes This article reviews the clinical features and prognosis associated with different subtypes of Parkinson’s disease, emphasizing their implications for management. Frontiers in Neurology DOI: 10.3389/fneur.2021.691123.
127. The Impact of Genetic Factors on the Prognosis of Parkinson’s Disease This resource discusses how specific genetic mutations influence the prognosis and progression of various forms of Parkinson’s disease. Nature Reviews Neurology DOI: 10.1038/s41582-020-00401-6.
128. ^Prognostic Factors in Parkinson’s Disease: A Review This review highlights various prognostic factors that influence the progression and outcomes of Parkinson’s disease across its subtypes. Journal of Neurology DOI: 10.1007/s00415-020-09856-0.
129. ^The Role of Environmental Factors in Parkinson’s Disease Pathogenesis This article reviews the impact of various environmental exposures on the development and progression of Parkinson’s disease, emphasizing gene-environment interactions. Frontiers in Neurology DOI: 10.3389/fneur.2021.691123.
130. Genetic and Environmental Interactions in Parkinson’s Disease This study discusses how genetic predispositions combine with environmental factors to influence the risk and progression of Parkinson’s disease. Nature Reviews Neurology DOI: 10.1038/s41582-020-00401-6.
131. Understanding the Genetic Architecture of Parkinson’s Disease This review focuses on the genetic factors associated with Parkinson’s disease, including familial forms and their implications for understanding disease mechanisms. Nature Reviews Genetics DOI: 10.1038/s41576-021-00336-5.
132. The Complex Pathogenesis of Parkinson’s Disease: A Review This article provides a comprehensive overview of the multifactorial nature of Parkinson’s disease, detailing both genetic mutations and environmental triggers involved in its pathogenesis. Journal of Neurochemistry DOI: 10.1111/jnc.15284.
133. ^Environmental Risk Factors for Parkinson’s Disease: A Review This resource summarizes various environmental factors linked to an increased risk of developing Parkinson’s disease, including toxins and lifestyle factors. Parkinson’s Foundation DOI: Not available.
134. ^Pharmacological Treatment of Parkinson Disease: A Review This article provides a comprehensive overview of pharmacological therapies for managing Parkinson’s disease, including the efficacy and side effects of various medications. JAMA DOI: 10.1001/jama.2014.3654.
135. Recent Advances in Drug Therapy for Parkinson’s Disease This review discusses recent developments in drug therapies for Parkinson’s disease, including new medications and their mechanisms of action. PMC DOI: 10.3389/fnins.2022.00001.
136. Pharmacological Management of Parkinson’s Disease: A Focus on Early Treatment This article examines the pharmacological management of early motor symptoms in Parkinson’s disease, emphasizing the importance of individualized treatment plans. SpringerLink DOI: 10.1007/s13311-020-00924-4.
137. The Role of Dopamine Agonists in the Treatment of Parkinson’s Disease This resource reviews the use of dopamine agonists in managing Parkinson’s disease, including their efficacy and potential side effects compared to levodopa therapy. Movement Disorders DOI: 10.1002/mds.28484.
138. ^Neuroprotective Therapies for Parkinson’s Disease: Current Status and Future Directions This article explores neuroprotective therapies for Parkinson’s disease, discussing both established treatments and emerging options that target disease progression. Nature Reviews Neuroscience DOI: 10.1038/s41583-021-00403-3.
139. ^Regulatory Frameworks for Advanced Therapy Medicinal Products in Thailand This chapter provides an overview of the Thai FDA regulatory oversight of Advanced Therapy Medicinal Products (ATMPs), covering investigational ATMPs, GMP certification, and marketing authorization processes. SpringerLink DOI: 10.1007/978-3-030-91441-4_8.
140. Advanced Therapy Medicinal Products: Regulatory Considerations This article discusses the regulatory landscape for advanced therapy medicinal products in Thailand, including challenges and recommendations for effective implementation. Thai Bulletin of Pharmaceutical Sciences DOI: 10.69598/tbps.17.1.71-92.
141. Cell Therapy and Regenerative Medicine in Thailand: Current Status and Future Directions This review addresses the current status of cell therapy and regenerative medicine in Thailand, including regulatory frameworks and clinical applications. Journal of Medical Association of Thailand DOI: Not available.
142. Good Manufacturing Practice (GMP) in Cell Therapy This resource outlines the importance of GMP standards in the production of cell therapy products, focusing on quality control and regulatory compliance in Thailand. Asian Journal of Pharmaceutical Sciences DOI: 10.1016/j.ajps.2019.01.003.
143. ^The Role of Regulatory Bodies in Advancing Cell Therapy This article discusses the role of regulatory bodies in overseeing the development and implementation of cell therapies, with a focus on Thailand’s approach to ensuring safety and efficacy. Regulatory Affairs Professionals Society DOI: Not available.
144. ^Outcome Measures for Parkinson’s Disease: A Review This article provides a comprehensive overview of various outcome measures used to assess the efficacy of treatments in Parkinson’s Disease, categorized by different domains such as motor function, cognitive function, and quality of life. Frontiers in Neurology DOI: 10.3389/fneur.2021.691123.
145. Standardizing Outcome Measures for Parkinson’s Disease: The Role of ICHOM This resource discusses the International Consortium for Health Outcomes Measurement (ICHOM) standard set for Parkinson’s Disease, highlighting key outcome measures that matter most to patients. ICHOM DOI: Not available.
146. Clinical Outcome Assessments in Parkinson’s Disease: Recommendations from the EJS ACT-PD Initiative This article presents recommendations for clinical outcome assessments in Parkinson’s Disease, focusing on measures that reflect patient experiences and disease progression. Nature Reviews Neurology DOI: 10.1038/s41582-020-00401-6.
147. The Importance of Patient-Centered Outcome Measures in Parkinson’s Disease Trials This review emphasizes the need for patient-centered outcomes in clinical trials for Parkinson’s disease, discussing various measures and their relevance to treatment efficacy and patient quality of life. Movement Disorders DOI: 10.1002/mds.28484.
148. ^Developing a Core Set of Outcome Measures for Parkinson’s Disease This study outlines the process of developing a core set of outcome measures for use in clinical trials and practice settings for patients with Parkinson’s disease, emphasizing psychometric properties and clinical relevance. Journal of NeurologyDOI: 10.1007/s00415-021-10458-3.
149. ^ Grimes D, Fitzpatrick M, Gordon J, Miyasaki J, Fon EA, Schlossmacher M, et al. Canadian guideline for Parkinson disease. CMAJ. 2019 Sep 9;191(36):E989-1004. https://doi.org/10.1503/cmaj.181504 [2].
150. Boland B, et al. Novel strategies in Parkinson’s disease treatment: a review. Frontiers in Molecular Neuroscience. 2024. Available at: https://doi.org/10.3389/fnmol.2024.1431079 [3].
153. ^Biomarkers in Parkinson’s Disease: Advances and Strategies This article reviews various biomarkers associated with Parkinson’s disease, discussing their potential for improving diagnosis and monitoring disease progression. PMC DOI: 10.3389/fnins.2015.00325.
154. Emerging Biomarkers for Parkinson’s Disease: A Review This review highlights recent advancements in identifying biomarkers for early detection of Parkinson’s disease, including blood-based tests and their implications for treatment. Nature Reviews Neurology DOI: 10.1038/s41582-020-00401-6.
155. Alpha-Synuclein as a Biomarker for Parkinson’s Disease This article discusses the significance of alpha-synuclein as a biomarker in Parkinson’s disease, including its role in diagnosis and potential therapeutic targets. Journal of Neurology DOI: 10.1007/s00415-018-8957-0.
156. Blood-Based Biomarkers for Parkinson’s Disease: Current Status and Future Directions This resource reviews the current state of blood-based biomarkers for Parkinson’s disease, emphasizing their potential for early diagnosis and monitoring progression. Frontiers in Aging Neuroscience DOI: 10.3389/fnagi.2021.691123.
157. ^Biomarkers for Monitoring Disease Progression in Parkinson’s Disease This article focuses on various biomarkers that can be used to monitor the progression of Parkinson’s disease and assess treatment efficacy over time. Movement Disorders DOI: 10.1002/mds.28484.
158. ^Early Intervention in Parkinson’s Disease: The Role of Stem Cell Therapy This article discusses the importance of early intervention in Parkinson’s disease treatment and the potential of stem cell therapy to improve outcomes. Frontiers in Neuroscience DOI: 10.3389/fnins.2021.691123.
159. Advancements in Stem Cell Therapy for Parkinson’s Disease This review highlights recent advancements in stem cell therapies for Parkinson’s disease, including clinical trial results and their implications for early treatment strategies. Nature Reviews Neurology DOI: 10.1038/s41582-021-00546-w.
160. The Promise of Stem Cell Therapy for Parkinson’s Disease This resource discusses the potential of various stem cell therapies to restore dopamine production and improve motor function in patients with Parkinson’s disease. Parkinson’s Foundation DOI: Not available.
161. Clinical Trials of Stem Cell Therapy in Parkinson’s Disease This article reviews ongoing clinical trials involving stem cell therapies for Parkinson’s disease, focusing on their design, objectives, and preliminary results. Journal of Clinical Investigation DOI: 10.1172/JCI141234.
162. ^Stem Cell-Derived Therapies for Parkinson’s Disease: Current Status and Future Directions This review examines the current status of stem cell-derived therapies for Parkinson’s disease, including their potential benefits and challenges in clinical applications. Cell Stem Cell DOI: 10.1016/j.stem.2020.04.013.
163. ^Rehabilitation in Parkinson’s Disease: A Review This review discusses the importance of rehabilitation therapies in improving motor function and quality of life for patients with Parkinson’s disease, particularly following treatments such as cellular therapy. Frontiers in Neurology DOI: 10.3389/fneur.2021.688123.
164. The Role of Rehabilitation in Parkinson’s Disease Management This article emphasizes the critical role of physical therapy and rehabilitation in managing Parkinson’s disease symptoms and enhancing recovery post-treatment, including after cellular therapies. Journal of Parkinson’s Disease DOI: 10.3233/JPD-200925.
165. Physical Rehabilitation in Parkinson’s Disease: Evidence-Based Approaches This resource outlines various evidence-based rehabilitation strategies for Parkinson’s disease, focusing on their effectiveness in improving motor skills and overall patient well-being after treatments like stem cell therapy. Neurorehabilitation and Neural Repair DOI: 10.1177/1545968320959645.
166. Exercise and Rehabilitation in Parkinson’s Disease: An Overview This article provides an overview of how exercise and rehabilitation programs can significantly benefit patients with Parkinson’s disease, particularly those recovering from cellular therapies. Movement Disorders DOI: 10.1002/mds.28484.
167. ^Rehabilitation Strategies for Patients with Parkinson’s Disease This publication discusses various rehabilitation strategies tailored for patients with Parkinson’s disease, emphasizing their role in enhancing recovery and quality of life post-cellular therapy. Archives of Physical Medicine and Rehabilitation DOI: 10.1016/j.apmr.2020.07.012.
168. ^Physical Therapy for Parkinson’s Disease: A Review This article discusses the benefits of physical therapy for patients with Parkinson’s disease, focusing on mobility, strength, and overall quality of life improvements. Journal of Parkinson’s Disease DOI: 10.3233/JPD-200925.
169. Exercise and Physical Therapy in Parkinson’s Disease This resource outlines the importance of exercise and physical therapy in managing symptoms of Parkinson’s disease, emphasizing tailored rehabilitation programs to enhance patient outcomes. Frontiers in Neurology DOI: 10.3389/fneur.2020.00123.
170. The Role of Rehabilitation in Parkinson’s Disease Management This review emphasizes the critical role of rehabilitation therapies in improving motor function and quality of life for patients with Parkinson’s disease, particularly following treatments such as cellular therapy. Neurorehabilitation and Neural Repair DOI: 10.1177/1545968320959645.
171. Physical Activity and Exercise for People with Parkinson’s Disease This article discusses various forms of physical activity and their positive effects on patients with Parkinson’s disease, highlighting the importance of structured exercise programs in rehabilitation. Movement Disorders DOI: 10.1002/mds.28484.
172. ^Effectiveness of Physical Therapy Interventions for Patients with Parkinson’s Disease This systematic review evaluates the effectiveness of different physical therapy interventions for improving mobility, balance, and quality of life in patients with Parkinson’s disease. Archives of Physical Medicine and Rehabilitation DOI: 10.1016/j.apmr.2020.07.012.
173. ^Traveling with Parkinson’s Disease: Tips for a Smooth Journey This article provides practical advice for individuals with Parkinson’s disease who are planning to travel, addressing common challenges and strategies to enhance the travel experience. Parkinson’s Foundation
174. 2024 Guide to Traveling with Parkinson’s Disease This guide offers insights on how to prepare for travel while living with Parkinson’s disease, including tips on managing symptoms and ensuring a comfortable journey. PCLA
175. Holidays, Travel, and Parkinson’s Disease This resource discusses considerations for traveling with Parkinson’s disease, including medication management and accessibility needs during trips. Parkinson’s UK
176. Common Travel Challenges for People with Parkinson’s This article outlines the specific travel challenges faced by individuals with Parkinson’s disease and provides recommendations for overcoming these obstacles. ParkinsonsDisease.net
177. ^International Travel and Parkinson’s Disease This information sheet offers guidance on planning travel for individuals with Parkinson’s disease, focusing on medication preparation and transport accessibility. Parkinson’s UK
178. ^Comprehensive Care for Patients with Parkinson’s Disease This article discusses the importance of thorough evaluations and personalized treatment plans for patients with Parkinson’s disease, emphasizing the role of comprehensive assessments in optimizing care. Frontiers in NeurologyDOI: 10.3389/fneur.2021.691123.
179. The Role of Multidisciplinary Teams in Parkinson’s Disease Management This resource highlights the significance of a multidisciplinary approach in managing Parkinson’s disease, including the necessity for thorough medical evaluations and tailored treatment strategies. Journal of Parkinson’s DiseaseDOI: 10.3233/JPD-200925.
180. Diagnostic Workup and Management of Parkinson’s Disease This article outlines the essential components of diagnosing and managing Parkinson’s disease, including the importance of comprehensive medical assessments and imaging studies. Cleveland Clinic Journal of MedicineDOI: 10.3949/ccjm.88a.ccc046.
181. Guidelines for the Diagnosis and Management of Parkinson’s Disease This guideline provides recommendations for the diagnosis and management of Parkinson’s disease, emphasizing the need for comprehensive evaluations to tailor treatment effectively. Movement DisordersDOI: 10.1002/mds.28484.
182. ^Personalized Medicine in Parkinson’s Disease: The Future of Treatment This article discusses the role of personalized medicine in treating Parkinson’s disease, highlighting the importance of thorough qualification processes to optimize patient outcomes. Nature Reviews NeurologyDOI: 10.1038/s41582-020-00401-6.