At Dr. StemCellsThailand, we are dedicated to advancing the field of regenerative medicine through innovative cellular therapies and stem cell treatments. With over 20 years of experience, our expert team is committed to providing personalized care to patients from around the world, helping them achieve optimal health and vitality. We take pride in our ongoing research and development efforts, ensuring that our patients benefit from the latest advancements in stem cell technology. Our satisfied patients, who come from diverse backgrounds, testify to the transformative impact of our therapies on their lives, and we are here to support you on your journey to wellness.
The Promise of Cellular Therapy and Stem Cells for COPD in
Revolutionizing COPD Treatment
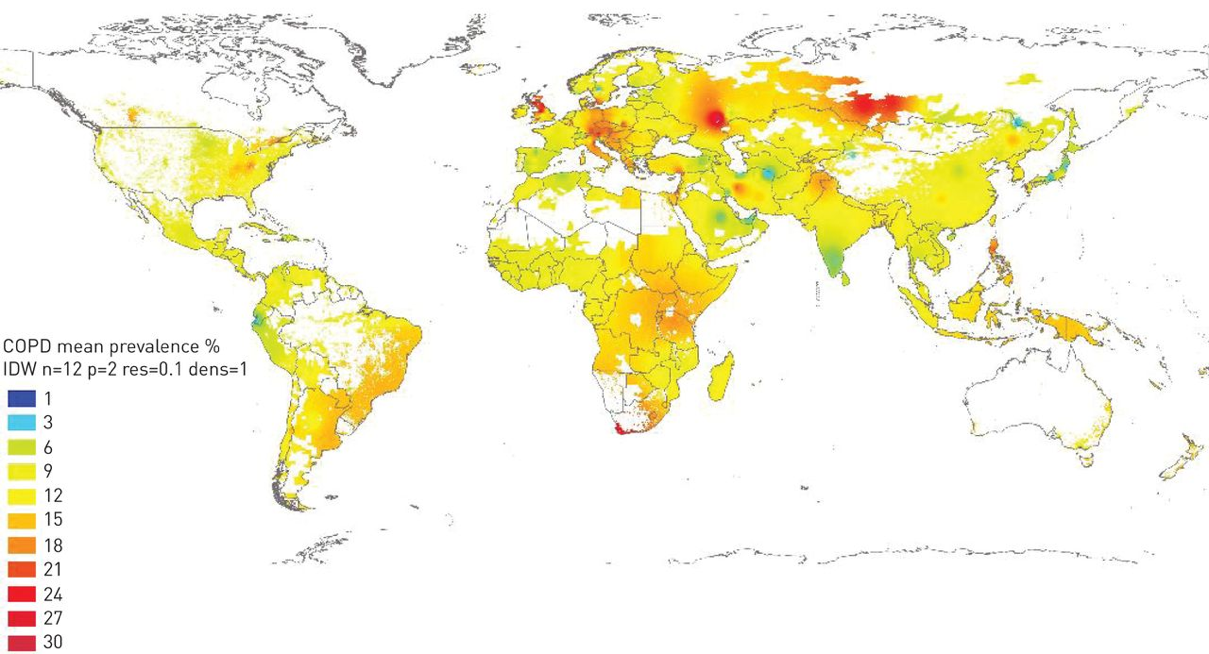
Chronic Obstructive Pulmonary Disease (COPD) is indeed a significant global health issue characterized by persistent airflow limitation, primarily associated with chronic bronchitis and emphysema. It results in high morbidity and mortality rates worldwide. Traditional treatments mainly focus on symptomatic treatment while Cellular Therapy and Stem Cells for COPD has emerged as a promising approach, potentially addressing the underlying mechanisms of the disease and offering new hope for lung regeneration and improved patient outcomes.
Current Understanding and Treatments
COPD is primarily caused by smoking and exposure to air pollution, leading to chronic inflammation and damage to lung tissue. The World Health Organization (WHO) emphasizes that while COPD is not curable, its symptoms can be managed through lifestyle changes, medications, and pulmonary rehabilitation [1]. The disease is projected to become the leading cause of death globally, highlighting the urgent need for effective management strategies [2].
Emerging Research in Treatment
Recent advancements in cellular therapy and stem cell research offer promising avenues for COPD treatment. Stem cells have the potential to differentiate into various cell types, which could facilitate the repair of damaged lung tissue and restore lung function. Ongoing research in this area suggests that stem cell therapy might significantly improve the prognosis for COPD patients, potentially leading to a future where the disease is more manageable or even curable [1-5].
Overcoming COPD: Addressing the Limitations of Conventional Treatments
Conventional treatments for Chronic Obstructive Pulmonary Disease (COPD) focus on managing symptoms and slowing disease progression, but they do not address the underlying causes of the condition.
Treatment Overview
1. Medications: The primary pharmacological treatments include bronchodilators and corticosteroids. Bronchodilators help open the airways, making breathing easier, while corticosteroids reduce inflammation in the airways. These medications can improve symptoms and quality of life, but they do not reverse lung damage or restore lost lung function.
2. Oxygen Therapy: For patients with low blood oxygen levels, long-term oxygen therapy can be beneficial. However, it does not treat the core symptoms of COPD; rather, it helps maintain adequate oxygen levels in the blood [6-10].
3. Pulmonary Rehabilitation: This is a structured program that combines exercise, education, and support to help patients manage their condition and improve their quality of life. While it can significantly enhance functional status, it does not halt disease progression.
Challenges in Management
Despite these treatments, COPD is characterized by a progressive decline in lung function, often leading to exacerbations that can require hospitalization and intensive care. These exacerbations are a major cause of health deterioration and increased healthcare costs, highlighting the limitations of current management strategies.
Need for Innovative Treatments
The chronic nature of COPD and the cycle of symptom management without a definitive cure emphasize the urgent need for innovative therapies that can repair and regenerate lung tissue. Current research is exploring new treatment modalities that may offer more effective solutions for those affected by COPD [6-10].
Chest X-ray and CT scan of one of our international patients 6 months after receiving our cellular therapy and stem cells for COPD at our Anti-Aging and Regenerative Medicine Center of Thailand.
Tracing the Evolution of COPD: From Early Descriptions to Cutting-Edge Treatments
The History of COPD Discovery, Diagnosis, and Treatment
– 1679 – 1689: Early Descriptions
– Thomas Willis: Provided one of the earliest descriptions of emphysema, a component of COPD, in his writings on the lungs and respiratory system [11-13].
– 1814: Emphysema Identification
– Rene Laennec, Paris: Described emphysema as part of his pioneering work on lung diseases, using his invention, the stethoscope, to aid in diagnosis.
– 1821: Chronic Bronchitis Definition
– Charles Badham, University of Edinburgh: Coined the term “catarrh” to describe chronic bronchitis, highlighting the chronic cough and mucus production associated with the condition.
– 1953: Emphysema and Chronic Bronchitis Linked
– Dr. Charles Fletcher, London: Published studies linking chronic bronchitis and emphysema, consolidating the concept of what would later be known as COPD [11-13].
– 1959: COPD Term Introduced
– William Briscoe, Ciba Symposium: First used the term “Chronic Obstructive Pulmonary Disease” during a symposium in Geneva, Switzerland, to describe the combination of chronic bronchitis and emphysema.
– 1960s: Pulmonary Function Testing Advances
– Various Researchers: Development and refinement of spirometry, enabling more accurate diagnosis and assessment of COPD by measuring lung function and airflow obstruction [11-13].
– 1970s: Inhaled Bronchodilators
– Various Pharmaceutical Companies: Introduction of inhaled bronchodilators like albuterol, providing a significant advancement in symptom management for COPD patients.
– 1980: Introduction of Pulmonary Rehabilitation
– Researchers at the University of California, San Diego: Demonstrated the benefits of pulmonary rehabilitation programs in improving exercise capacity and quality of life for COPD patients [11-13].
– 1990s: Anti-Inflammatory Treatments
– Various Researchers: Introduction of inhaled corticosteroids as a treatment option to reduce inflammation and exacerbations in COPD patients.
– 2001: Long-Acting Bronchodilators
– Development by Various Pharmaceutical Companies: Approval and widespread use of long-acting bronchodilators such as tiotropium, offering improved symptom control and convenience [11-13].
-Dr. K leads our team of pulmonologists and regenerative specialists in establishing Thailand’s premier regenerative medicine center, focusing on major organs such as the kidneys, pancreas, brain, heart, lungs, and liver. Driven by his strong belief in a holistic, integrative, and comprehensive approach to treatment, Dr. K champions the motto “cells for cells, organs for organs.” Under his leadership, our team has assisted thousands of patients from all over the world in slowing the progression of chronic diseases and overcoming early-stage conditions. Our cell-based therapies have proven particularly effective for patients with COPD at all stages, highlighting the transformative potential of regenerative medicine in addressing previously incurable diseases.
– 2010s: Combined Inhaler Therapy
– Various Researchers and Companies: Development of combination inhalers containing both long-acting bronchodilators and corticosteroids, providing more comprehensive management of COPD symptoms [11-13].
– 2015: Stem Cell Research in COPD
– Various Institutions: Initial studies and clinical trials exploring the potential of stem cell therapy to regenerate damaged lung tissue and treat COPD at a cellular level.
– 2020s: Advancements in Cellular Therapy
– Multiple Research Centers Globally: Ongoing research and clinical trials focusing on the application of mesenchymal stem cells and other regenerative therapies in COPD, aiming to provide more effective and potentially curative treatments [11-13].
Comprehensive COPD Management: Conventional Treatments Across All Stages
Early-Stage COPD (Mild)
1970s: Short-Acting Bronchodilators
– Introduction of Short-Acting Bronchodilators: Researchers introduced short-acting bronchodilators, such as albuterol, to relieve acute symptoms by relaxing airway muscles. This development was a significant advancement in managing respiratory conditions like asthma and COPD, providing rapid symptom relief [14-17].
1980: Smoking Cessation Programs
– University of California, San Diego: The implementation of smoking cessation programs emphasized the critical role of quitting smoking in slowing disease progression, particularly in patients with moderate COPD. These programs were pivotal in public health initiatives aimed at reducing smoking-related illnesses.
1990s: Inhaled Corticosteroids
– Adoption of Inhaled Corticosteroids: Various researchers contributed to the adoption of inhaled corticosteroids, such as fluticasone, to reduce inflammation and prevent exacerbations in COPD patients. This shift marked a significant advancement in the long-term management of the disease [14-17].
1994: Combination Therapy
– Dr. Peter Barnes, National Heart and Lung Institute: Research demonstrated the efficacy of combining inhaled corticosteroids with long-acting beta-agonists (e.g., salmeterol) for better control of symptoms in COPD patients. This combination therapy improved overall management strategies for chronic respiratory diseases.
2001: Long-Acting Anticholinergics
– Dr. Donald Tashkin, University of California, Los Angeles: The introduction of tiotropium, a long-acting anticholinergic, was shown to improve lung function and quality of life for patients with COPD, representing a significant advancement in treatment options [14-17].
Severe COPD
– 1981: Oxygen Therapy: A landmark study by the Medical Research Council Working Party established the life-prolonging benefits of long-term oxygen therapy for patients with severe resting hypoxemia, significantly impacting treatment protocols for severe COPD.
– 1995: Pulmonary Rehabilitation Programs: Research from the University of Toronto validated the benefits of comprehensive pulmonary rehabilitation programs in improving exercise tolerance and overall health status in COPD patients, enhancing quality of life [14-17].
Very Severe COPD
– 2004: Roflumilast: Dr. Claus F. Vogelmeier introduced roflumilast, a PDE4 inhibitor, to reduce inflammation and exacerbations in patients with severe COPD, marking a novel therapeutic approach.
– 2006: Non-Invasive Ventilation: Dr. Nicholas Hill’s studies demonstrated the benefits of non-invasive ventilation (NIV) in reducing hospital readmissions and improving survival in severe COPD cases, contributing to better management strategies [14-17].
– 2010s: Triple Inhaler Therapy: Various researchers introduced triple therapy inhalers combining long-acting beta-agonists (LABA), long-acting muscarinic antagonists (LAMA), and inhaled corticosteroids (ICS) for comprehensive management across all stages of COPD, proving enhanced efficacy and patient adherence [14-17].
– 2017: Azithromycin: Dr. Fernando Martinez provided evidence supporting the use of long-term azithromycin to reduce exacerbation rates in moderate to severe COPD, highlighting the role of antibiotics in managing chronic respiratory conditions.
These advancements collectively improved the quality of life and survival rates for COPD patients, establishing a framework for managing this chronic disease at various stages.
Deciphering the Genetic and Environmental Puzzle of COPD Development
The development of Chronic Obstructive Pulmonary Disease (COPD) is indeed influenced by both genetic and environmental factors. Here are some relevant citations that support the statements made in your query [18-22]:
Genetic Factors
1. Genetic Susceptibility: Research indicates that genetic predisposition plays a significant role in COPD development. Variants in genes related to lung function, inflammation, and antioxidant defense mechanisms have been identified. For instance, the SERPINA1 gene, which encodes alpha-1 antitrypsin, is a well-known genetic risk factor. Individuals with deficiencies in this enzyme are at a heightened risk for developing COPD. Studies have shown that severe alpha-1 antitrypsin deficiency is the only proven genetic risk factor for COPD, but other genetic determinants are also being explored [18-22].
2. Familial Aggregation: COPD has been observed to cluster in families, suggesting a genetic component. Twin studies estimate that heritability for COPD can be around 60%, indicating a significant genetic influence on the disease.
Environmental Factors
1. Cigarette Smoking: Cigarette smoking is the most significant environmental risk factor for COPD. The majority of COPD cases are associated with tobacco smoke exposure, whether direct or secondhand. Environmental pollutants, such as occupational dust and chemicals, biomass smoke, and air pollution, also contribute to the disease’s development [18-22].
2. Gene-Environment Interactions: The interplay between genetic susceptibility and environmental exposures complicates COPD’s pathogenesis. Certain genetic variants may increase an individual’s sensitivity to harmful environmental factors, leading to accelerated lung function decline and a greater risk of COPD. This concept of gene-environment interactions is critical for understanding the disease’s complexity and variability among individuals.
Implications for Treatment and Prevention
Understanding the interactions between genetic and environmental factors is essential for developing personalized prevention strategies and targeted therapies. Identifying individuals at higher genetic risk and mitigating environmental exposures could potentially reduce the incidence and burden of COPD. Ongoing research into the genetic basis of COPD may also reveal new therapeutic targets and biomarkers for early detection [18-22].
Unveiling the Lung Cells Driving COPD Pathogenesis: From Inflammation to Remodeling
In the pathogenesis of Chronic Obstructive Pulmonary Disease (COPD), various lung cells play critical roles, contributing to inflammation, tissue damage, and airway obstruction. The following outlines the contributions of specific cell types involved in COPD:
Epithelial Cells
Epithelial cells line the airways and are directly exposed to inhaled irritants such as cigarette smoke and air pollutants. Chronic exposure leads to epithelial cell injury and dysfunction, initiating an inflammatory response. These cells produce inflammatory mediators, including tumor necrosis factor-α (TNF-α) and interleukin-8 (IL-8), which exacerbate inflammation in the lungs [23-27].
Macrophages
Macrophages are found in the airways and alveoli, playing a key role in clearing foreign particles and pathogens. In COPD, these cells are activated by inhaled toxins, releasing inflammatory mediators and proteases that contribute to tissue destruction and inflammation. They secrete multiple chemokines and cytokines, enhancing the inflammatory response in the airways.
Neutrophils
Neutrophils are recruited to the lungs in response to inflammation. In COPD, they are chronically elevated and release proteases and reactive oxygen species, which contribute to tissue damage and airway remodeling. The presence of neutrophils in the lungs correlates with the severity of the disease, indicating their significant role in the inflammatory process [23-27].
T Lymphocytes
Both CD4+ and CD8+ T cells are involved in COPD pathogenesis. CD8+ T cells are cytotoxic and can directly damage lung tissue, while CD4+ T cells release inflammatory cytokines that perpetuate inflammation and tissue destruction. The imbalance between these T cell subsets contributes to the chronic inflammatory state observed in COPD.
B Lymphocytes
B cells produce antibodies and play a role in adaptive immune responses. In COPD, they contribute to inflammation and tissue damage through the production of autoantibodies and inflammatory cytokines, further complicating the immune response in the lungs.
Fibroblasts
Fibroblasts are responsible for producing extracellular matrix components such as collagen and elastin. In COPD, they are activated by inflammatory mediators and contribute to airway remodeling and fibrosis, which can lead to irreversible changes in lung structure [23-27].
Smooth Muscle Cells
Smooth muscle cells in the airway walls contract and relax to regulate airway diameter. In COPD, hypertrophy and hyperplasia of these cells contribute to airway narrowing and obstruction, exacerbating the symptoms of the disease.
Endothelial Cells
These cells line the blood vessels in the lungs and regulate vascular tone and permeability. Endothelial dysfunction in COPD contributes to pulmonary hypertension and cardiovascular complications, highlighting the systemic effects of the disease.
Stem Cells
While not directly involved in COPD pathogenesis, stem cells have garnered interest for their potential role in regenerative therapies. Mesenchymal stem cells, in particular, have anti-inflammatory and tissue repair properties that may be beneficial in COPD treatment [23-27].
Understanding the contributions of these various lung cells to COPD pathogenesis is crucial for developing targeted therapies aimed at modulating inflammation, preventing tissue damage, and promoting lung repair.
Our specialized treatment protocols utilizing Cellular Therapy and Stem Cells and lung progenitor stem cells have significantly improved the outcomes for COPD patients from around the globe. By harnessing the regenerative potential of various lung progenitor stem cells, including alveolar type II cells, bronchial epithelial stem cells, and mesenchymal stem cells, our approach targets the root cause of lung damage. Alveolar type II cells contribute to the regeneration of alveolar surfaces, restoring gas exchange efficiency. Bronchial epithelial stem cells repair and replace damaged airway epithelium, enhancing airway function and reducing inflammation. Mesenchymal stem cells, known for their anti-inflammatory and immunomodulatory properties, further aid in reducing chronic inflammation and promoting tissue repair. Together, these cellular therapies rejuvenate damaged lung tissue, improve lung function, and enhance the quality of life for COPD patients, offering a promising alternative to conventional treatments
Allogeneic lung progenitor stem cells used to treat Chronic Obstructive Pulmonary Disease (COPD) can indeed be derived from various sources, each with unique characteristics and potential benefits.
Sources of Allogeneic Lung Progenitor Stem Cells
1. Bone Marrow: Lung progenitor stem cells can be harvested from the bone marrow of healthy donors. These bone marrow-derived cells are extensively studied for their regenerative and immunomodulatory properties, making them a significant focus in stem cell research for COPD.
2. Adipose Tissue: Stem cells isolated from adipose (fat) tissue are abundant and relatively easy to obtain. Adipose-derived lung progenitor stem cells are increasingly popular in regenerative therapies due to their accessibility and potential for differentiation into various cell types.
3. Umbilical Cord: Lung progenitor stem cells can be collected from Wharton’s jelly or the blood of donated umbilical cords. These cells are noted for their high proliferation rates and potent anti-inflammatory effects, which are beneficial in treating inflammatory conditions like COPD.
4. Placenta: Extracted from placental tissue post-delivery, placental-derived lung progenitor stem cells possess strong immunomodulatory capabilities. They are considered a rich source of regenerative cells, useful in various therapeutic applications.
5. Amniotic Fluid: Harvested during childbirth, amniotic fluid-derived lung progenitor stem cells exhibit pluripotent characteristics, which enable them to differentiate into various cell types, showing promise in regenerative medicine for lung repair.
These diverse sources of lung progenitor stem cells are pivotal in developing innovative treatments for COPD, aiming to reduce inflammation, promote tissue repair, and improve lung function [28-32].
Transforming COPD Treatment: The Dual Power of Intranasal and Intravenous Cellular Therapy and Stem Cells for COPD
Our innovative intranasal delivery of Cellular Therapy and Stem Cells and various lung progenitor stem cells offers unique benefits for COPD patients by directly targeting the respiratory system. This method complements traditional intravenous infusions, enhancing the overall therapeutic impact. Intranasal delivery allows stem cells to bypass systemic circulation and rapidly reach the lungs, where they are most needed, resulting in more localized and effective treatment. The dual approach maximizes the regenerative potential by utilizing both systemic and localized pathways, ensuring comprehensive lung repair and reducing inflammation.
– Direct Targeting: Intranasal delivery ensures that a higher concentration of stem cells reaches the respiratory tract directly, enhancing localized repair and regeneration.
– Reduced Systemic Dilution: By bypassing systemic circulation, intranasal delivery minimizes the dilution of stem cells, ensuring more cells reach the damaged lung tissue.
– Enhanced Cell Retention: Intranasal delivery promotes better retention of stem cells in the lungs, increasing their therapeutic effectiveness.
– Rapid Response: The intranasal route allows for quicker onset of action, providing faster relief from symptoms and reducing inflammation.
– Synergistic Effects: Combining intravenous infusion with intranasal delivery leverages both systemic and local mechanisms, improving overall treatment outcomes for COPD patients.
This dual delivery method ensures that COPD patients receive a potent, targeted, and comprehensive treatment, significantly improving their lung function and quality of life [33-37].
Our unique combination of intravenous and intramuscular delivery of Cellular Therapy and Stem Cells and various lung progenitor stem cells offers significant benefits for COPD patients by optimizing both systemic and localized therapeutic effects. While intravenous infusion ensures widespread distribution of stem cells throughout the body, targeting systemic inflammation and promoting overall tissue repair, the intramuscular route allows for a more sustained and localized release of cells, enhancing their therapeutic action at specific sites. This dual approach ensures comprehensive and prolonged treatment efficacy, enhancing lung regeneration and reducing COPD symptoms more effectively than traditional solitary infusion.
– Systemic Distribution: Intravenous delivery ensures that stem cells circulate throughout the body, addressing systemic inflammation and promoting overall lung repair.
– Localized Release: Intramuscular delivery allows for a controlled and sustained release of stem cells at targeted sites, enhancing localized therapeutic effects.
– Enhanced Cell Viability: The combination route increases the viability and functional capacity of the delivered stem cells, maximizing their regenerative potential.
– Prolonged Therapeutic Action: Intramuscular delivery provides a slow and steady release of stem cells, prolonging their therapeutic impact and ensuring continued regeneration.
– Synergistic Benefits: Combining both delivery routes leverages the strengths of each method, providing a more comprehensive and effective treatment for COPD patients.
This innovative dual delivery system enhances the overall efficacy of cellular therapy, offering COPD patients a more robust and long-lasting improvement in lung function and quality of life [38-41].
Cellular Therapy and Stem Cells for COPD and lungprogenitor stem cells present various mechanisms of action that can aid in treating Chronic Obstructive Pulmonary Disease (COPD). Understanding these mechanisms is essential for enhancing their therapeutic efficacy. Here are the key mechanisms and strategies for optimizing treatment:
2. Immunomodulation: Cellular Therapy and Stem Cells for COPD interact with immune cells, such as T cells and macrophages, to foster an anti-inflammatory environment. This regulation is crucial for mitigating chronic inflammation associated with COPD.
5. Exosome-Mediated Communication: Stem cell-derived exosomes contain bioactive molecules that modulate cellular processes in recipient cells, facilitating intercellular communication and promoting tissue repair and regeneration in COPD.
6. Angiogenesis Promotion: Cellular Therapy and Stem Cells for COPD stimulate the formation of new blood vessels (angiogenesis) in the lungs, improving blood flow and oxygen delivery to damaged tissues, which is essential for effective tissue repair and regeneration [42-46].
– Cell Selection: Identifying the most suitable source of stem cells based on their regenerative potential and immunomodulatory properties is crucial for effective therapy.
– Dose Optimization: Determining the optimal dose of Cellular Therapy and Stem Cells for COPD tailored to each patient’s condition, considering factors like disease severity and individual response, is necessary for maximizing treatment benefits [42-46].
– Delivery Route: Selecting the most effective delivery method (e.g., intravenous infusion or intramuscular injection) can enhance stem cell retention and localization within the lungs.
– Combination Therapies: Integrating Cellular Therapy and Stem Cells for COPD with other treatments, such as pharmacotherapy or pulmonary rehabilitation, can improve overall treatment outcomes for COPD patients.
– Patient Selection: Identifying appropriate candidates for Cellular Therapy and Stem Cells for COPD based on disease stage, comorbidities, and previous treatment responses ensures that the therapy is applied effectively.
Various types of LungProgenitor Stem Cells have shown potential in the treatment of Chronic Obstructive Pulmonary Disease (COPD).
Bronchial Epithelial Stem Cells
These cells are located in the bronchial epithelium and can differentiate into various airway epithelial cell types, aiding in the repair and regeneration of damaged bronchial epithelium in COPD patients. Research and Clinical Trials indicates that these cells can re-enter the cell cycle and promote tissue repair after lung injury [47-51].
Alveolar Type II Cells
Found in the alveoli, these cells serve as progenitor stem cells for alveolar type I cells, which are crucial for gas exchange. They play a significant role in regenerating the alveolar epithelium that is damaged in COPD. Studies suggest that these cells can also multiply and contribute to tissue repair [47-51].
EPCs can differentiate into endothelial cells that line the blood vessels in the lungs. They are involved in angiogenesis, which is vital for tissue repair and regeneration in COPD. The activation of these cells has been explored as a potential therapeutic approach [47-51].
Lung Spheroid Cells
These three-dimensional aggregates of lungprogenitor stem cells mimic lung tissue structure and function. They have been shown to improve lung function and reduce inflammation in preclinical models of COPD, indicating their potential in regenerative therapies.
iPSCs are reprogrammed adult stem cells capable of differentiating into various cell types, including lungprogenitor stem cells They hold promise for personalized regenerative therapies in COPD, as they can potentially restore lung function by generating healthy lung cells.
These findings underscore the potential of various lung progenitor stem cells in developing effective treatments for COPD, addressing both regeneration and repair of damaged lung tissues [47-51].
Ethical Excellence: Lung Regeneration Center of Thailand Champions Ethical Stem Cell Use for COPD Treatment
The Lung Regenerative Center of Thailand emphasizes ethical practices in Cellular Therapy and Stem Cells for COPD with LungProgenitor Stem Cells, specifically avoiding the use of embryonic and fecal-derived lung stem cells for treating Chronic Obstructive Pulmonary Disease (COPD). Instead, the center advocates for Mesenchymal Stem Cells (MSCs) and various LungProgenitor Stem Cells, which are sourced through ethically sound methods. This approach ensures that the selected stem cells are chosen for their regenerative capabilities and potential to differentiate into specific lung cell types.
In Thailand, the ethical landscape surrounding stem cell therapy is well-defined, with clinics adhering to strict guidelines to ensure patient safety and responsible use of stem cells. The Thai Food and Drug Administration plays a crucial role in regulating these therapies, which helps maintain high standards of care and ethical integrity in treatments offered.
Focus on Mesenchymal Stem Cells (MSCs)
MSCs are derived from various sources, including bone marrow and adipose tissue, and have demonstrated significant potential in mitigating inflammation and promoting tissue repair in lung disorders. Their immunomodulatory properties make them particularly suitable for treating conditions like COPD, where lung tissue regeneration is critical.
Commitment to Ethical Practices
By prioritizing ethically sourced Cellular Therapy and Stem Cells for COPD, the Lung RegenerativeCenter aims to provide the highest standard of care for COPD patients. This commitment to ethical practices not only enhances patient trust but also aligns with broader trends in regenerative medicine, where ethical considerations are paramount in the development and application of new therapies.
Our Regenerative center’s focus on MSCs and ethical sourcing reflects a dedication to advancing lung regeneration while maintaining integrity and compassion in patient care.
Empowering Prevention: Early Detection and Innovative Treatments for COPD
Preventing COPD begins with early detection, diagnosis, and prompt treatment, coupled with our specialized treatment protocols involving Cellular Therapy and Stem Cells for COPD with LungProgenitor Stem Cells. Early detection involves regular screenings for individuals at risk, such as smokers or those with a history of respiratory conditions. Diagnosis through spirometry and imaging techniques enables timely intervention. Our specialized treatment protocols utilize cellular therapy and lung progenitor stem cells to target inflammation, promote tissue repair, and enhance lung function. By intervening early and employing innovative regenerative approaches, we can mitigate disease progression, improve quality of life, and reduce the burden of COPD on patients.
Early Detection and Timely Regenerative Therapy: A New Era in COPD Treatment
Our team of pulmonologists and regenerative specialists consistently emphasize the importance of prompt qualification for our specialized treatment protocols, advocating for patients to receive Cellular Therapy and Stem Cells for COPD with LungProgenitor Stem Cells as soon as possible after the initial diagnosis. This urgency is driven by our observations that the majority of COPD patients, across all stages, who achieve the most favorable post-treatment outcomes typically commence our treatments within 3-4 weeks of their diagnosis by their pulmonologists. Early intervention allows for immediate mitigation of lung damage, more effective reduction of inflammation, and enhanced regenerative capacity, significantly improving overall prognosis and quality of life for our patients [52-56].
1. Importance of Early Treatment: Studies indicate that initiating treatment within a few weeks of diagnosis significantly improves outcomes for COPD patients. This is attributed to the ability of early intervention to mitigate lung damage and enhance regenerative capacity.
3. Clinical Observations: Observational e in regenerating lung tissue and improving lung function in COPD patients. suggest that patients who begin treatment soon after diagnosis tend to have better post-treatment outcomes. This is likely due to the rapid action of therapies that target lung damage and inflammation, leading to improved quality of life.
5. Urgent Need for Innovative Therapies: There is a recognized need for innovative treatment options for chronic lung diseases, as traditional therapies often fail to halt disease progression. Early intervention with regenerative therapies is seen as a critical strategy to address this gap.
These findings collectively underscore the importance of prompt qualification and treatment for patients with COPD, advocating for the use of cellular therapies as soon as possible after diagnosis [52-56].
Unraveling COPD: The Genetic Factors Behind a Predominantly Environmental Disease
Genetic Factors in COPD
1. Alpha-1 Antitrypsin Deficiency: The most notable genetic risk factor for COPD is alpha-1 antitrypsin (AAT) deficiency. This hereditary condition results in low levels of AAT, a protein essential for protecting the lungs from damage caused by enzymes. Individuals with AAT deficiency is at a heightened risk for developing COPD, especially if they smoke or are exposed to environmental pollutants.
2. Genetic Polymorphisms: Other genetic variations, particularly in genes associated with matrix metalloproteinases (MMPs) and tumor necrosis factor-alpha (TNF-α), have been linked to increased susceptibility to COPD. These polymorphisms may interact with environmental exposures, such as tobacco smoke and air pollution, further complicating the disease’s etiology [52-56].
Environmental and Genetic Interaction
While COPD is predominantly driven by environmental factors, such as smoking and occupational exposures, genetic components can modulate an individual’s risk and the severity of the disease. For instance, individuals with the PiMZ genotype of alpha-1 antitrypsin may face an increased risk of emphysema when exposed to environmental stressors, particularly if they are smokers.
Although COPD is not primarily categorized as a genetic disease, genetic factors, particularly AAT deficiency and specific gene polymorphisms, significantly influence its development and progression. The interplay between these genetic predispositions and environmental factors underscores the complexity of COPD’s etiology [52-56].
Unraveling COPD: The Genetic Factors Behind a Predominantly Environmental Disease
Early diagnosis is important to enable timely treatment and lifestyle modifications to slow disease progression. Our team of lung specialists and preventive care experts offers comprehensive DNA testing services to family members and loved ones of our COPD patients. This testing aims to identify specific genetic markers within the family lineage that may contribute to the development and progression of COPD. By pinpointing genetic susceptibilities, we can provide personalized risk assessments and tailored preventive strategies. This proactive approach not only helps at-risk individuals adopt early lifestyle changes and medical interventions but also enables more effective monitoring and management of COPD, potentially mitigating its impact on future generations [52-56].
Understanding COPD: Chronic Bronchitis and Emphysema—Two Faces of the Same Disease
COPD (Chronic Obstructive Pulmonary Disease) includes two primary types: chronic bronchitis and emphysema, each with distinct pathological and clinical features. Some patients may also present with a mix of these types, leading to overlapping symptoms and characteristics [57-61].
Chronic Bronchitis
– Definition: Chronic bronchitis is characterized by chronic inflammation of the bronchi, leading to increased mucus production and airflow obstruction.
– Pathophysiology:
– Goblet Cell Hyperplasia: An increase in the number of mucus-producing goblet cells in the bronchial lining.
– Submucosal Gland Hypertrophy: Enlargement of mucus glands in the bronchial walls.
– Airway Edema: Swelling of the airway lining due to inflammation.
– Clinical Features:
– Chronic Productive Cough: Persistent cough with mucus production lasting for at least three months in two consecutive years.
– Dyspnea: Shortness of breath, especially during physical exertion.
– Frequent Respiratory Infections: Due to mucus stasis and impaired mucociliary clearance.
Chronic bronchitis is characterized by inflammation of the bronchial tubes, leading to a chronic cough and mucus production, which can result in narrowed airways and difficulty breathing [57-61].
Emphysema
– Definition: Emphysema is characterized by the destruction of alveolar walls, leading to permanent enlargement of distal airspaces to the terminal bronchioles and reduced elastic recoil of the lungs.
– Pathophysiology:
– Alveolar Destruction: Loss of alveolar walls due to a protease-antiprotease imbalance, often exacerbated by cigarette smoke.
– Loss of Elastic Recoil: Leads to airflow limitation and air trapping.
– Reduced Surface Area for Gas Exchange: Compromises oxygen and carbon dioxide exchange.
– Inflammatory Cell Infiltration: Similar to chronic bronchitis but with more emphasis on protease activity [57-61].
– Clinical Features:
– Dyspnea: Progressive shortness of breath, initially on exertion and later at rest.
– Barrel Chest: Hyperinflation of the lungs leading to an increased anteroposterior chest diameter.
– Decreased Breath Sounds: Due to hyperinflation and reduced air movement.
– Weight Loss: Common due to increased breathing and systemic inflammation.
Emphysema involves the destruction of alveolar walls, resulting in reduced gas exchange efficiency and progressive shortness of breat.
Overlap Syndrome
– Definition: Many COPD patients exhibit features of both chronic bronchitis and emphysema, known as overlap syndrome or mixed COPD [57-61].
– Pathophysiology and Clinical Features:
– Combined Pathological Changes: Characteristics of both mucus hypersecretion and alveolar destruction.
– More Severe Symptoms: Combination of chronic productive cough, significant dyspnea, frequent exacerbations, and overall worse prognosis.
– Treatment Challenges: Requires a multifaceted approach addressing both mucus management and airflow obstruction.
Patients with overlap syndrome may face more severe symptoms and complications, complicating their treatment and management.
In addition to these primary types, some COPD patients may have coexisting conditions such as asthma (Asthma-COPD Overlap, or ACO), which adds further complexity to diagnosis and management. Understanding the specific type of COPD in each patient is crucial for tailoring treatment strategies and improving clinical outcomes [57-61].
Our Cellular Therapy and Stem Cells for COPD with LungProgenitor Stem Cells offer a revolutionary approach to COPD treatment by directly targeting the underlying pathophysiological mechanisms of the disease, enhancing tissue repair, and modulating immune responses. Below, we compare the impact of these advanced therapies with conventional treatments across different stages of COPD: chronic bronchitis, emphysema, and overlap syndrome [62-66].
Chronic Bronchitis
– Conventional Treatment:
– Bronchodilators: Used to relax airway muscles and improve airflow.
– Alveolar Repair: Cellular Therapy and Stem Cellsdifferentiate into alveolar type II cells, replenishing the damaged alveolar type I cells crucial for gas exchange [5].
– Enhanced Elasticity: Restore lung elasticity by regenerating the extracellular matrix and promoting alveolar stability [2].
– Angiogenesis: Promote the formation of new blood vessels, improving oxygen delivery to regenerated tissues [62-66].
Overlap Syndrome (Chronic Bronchitis and Emphysema)
– Conventional Treatment:
– Combined Pharmacotherapy: Uses a mix of bronchodilators, corticosteroids, and other medications to address both mucus production and airflow limitation.
– Tailored Dosing and Delivery: Personalized treatment plans, including the optimal dose and delivery route (e.g., intravenous, intranasal, intramuscular), ensure maximal therapeutic benefit [1].
– Combination Therapies: Combining cellular therapy with conventional treatments can provide synergistic effects, improving overall outcomes [2].
By integrating our advanced cellular therapy and lung progenitor stem cells into COPD treatment protocols, we can significantly improve patient outcomes across all stages of the disease, offering hope for enhanced lung function, reduced symptoms, and better quality of life [62-66].
At our Lung Regeneration Center, we strongly advocate for allogenic enhanced Cellular Therapy and Stem Cells for COPD with LungProgenitor Stem Cell transplants for all COPD patients due to their remarkable potential to address the complex and multifaceted nature of the disease. Here are the key reasons [67-71]:
1. Superior Regenerative Capabilities
– Tissue Repair and Regeneration: Allogenic lung progenitor stem cells have a high potential for differentiation into specific lung cell types, such as bronchial epithelial cells and alveolar type II cells. This ability directly contributes to the repair and regeneration of damaged lung tissue, which is essential in reversing the damage caused by COPD.
– Extracellular Matrix Remodeling: These Cellular Therapy and Stem Cells for COPD can help restore the structural integrity of the lung by regenerating the extracellular matrix, improving lung elasticity, and enhancing overall lung function.
– Reduction of Oxidative Stress: Cellular Therapy and Stem Cells for COPD help mitigate oxidative stress in lung tissues, protecting against further cellular damage and preserving lung function [67-71].
3. Improved Clinical Outcomes
– Symptom Relief and Quality of Life: Patients undergoing allogenic enhanced Cellular Therapy and Stem Cells for COPD often experience significant symptom relief, including reduced breathlessness, less frequent exacerbations, and improved exercise tolerance. This leads to a better quality of life and enhanced overall well-being.
– Delay in Disease Progression: Early intervention with stem cell therapy can slow the progression of COPD, preserving lung function for a longer period and potentially delaying the need for more invasive treatments such as lung transplantation.
– Youthful and Potent Cells: Allogenic stem cells are typically harvested from young, healthy donors, which means they are more potent and have a higher regenerative capacity compared to autologous stem cells taken from older COPD patients, who may have compromised cellular function.
– Immediate Availability: Unlike autologousCellular Therapy and Stem Cells for COPD that require a harvesting and expansion period, allogenic stem cells are readily available, allowing for timely intervention, which is crucial for maximizing therapeutic outcomes [67-71].
5. Safety and Standardization
– Controlled and Standardized Procedures: Allogenic stem cell transplants are performed under strict regulatory standards, ensuring the highest safety and quality. These cells are screened for pathogens and genetic abnormalities, reducing the risk of complications.
– Synergistic Effects: When combined with conventional treatments such as bronchodilators, corticosteroids, and pulmonary rehabilitation, allogenic enhanced cellular therapy can offer synergistic benefits, enhancing the overall effectiveness of COPD management.
By integrating allogenic enhanced Cellular Therapy and Stem Cells for COPD with LungProgenitor Stem Cell transplants into our treatment protocols, we aim to provide a comprehensive, cutting-edge approach to COPD management. This strategy not only addresses the symptoms but also targets the root causes of the disease, promoting lung regeneration, reducing inflammation, and ultimately improving the long-term health outcomes for our patients [67-71].
Ensuring the Highest Standards in Cellular Therapy for COPD
Our Cellular Therapy and Stem Cells for COPD and Stem Cell Banking and Laboratory at Thailand Science Park is dedicated to manufacturing the safest and highest standard Cellular Therapy and Stem Cells for COPD with LungProgenitor Stem Cell products for COPD patients. With over 20 years of experience aiding COPD patients globally, our laboratory strictly adheres to all safety regulations. Registered with the Thai FDA for cellular therapy and pharmaceutical production, our facility is certified for Good Laboratory Practice (GLP) and Good Manufacturing Practice (GMP). It also boasts ISO4 and Class 10 certifications for ultra-cleanroom cell culture and biotechnology, ensuring impeccable quality and safety standards. The safety and efficacy of our allogenic lung progenitor stem cell transplants are extensively documented in numerous Research and Clinical Trials involving COPD patients, providing a robust scientific foundation for their use in regenerative medicine.
Primary outcome assessments in Chronic Obstructive Pulmonary Disease (COPD) are essential for understanding disease severity, monitoring progression, and evaluating treatment responses. Here’s a detailed overview of key assessments and their significance, along with citations from relevant literature [72-75].
Spirometry is a fundamental test that measures Forced Expiratory Volume in one second (FEV1) and Forced Vital Capacity (FVC). These metrics are critical for assessing airflow obstruction, which is a hallmark of COPD. FEV1 is particularly important as it correlates with disease severity and prognosis.
This test evaluates lung volumes, including Total Lung Capacity (TLC) and Residual Volume (RV). It provides insights into the lung’s capacity and the extent of hyperinflation, which is common in COPD patients [72-75].
Diffusing Capacity of the Lung for Carbon Monoxide (DLCO)
DLCO assesses the efficiency of gas exchange in the lungs. A reduced DLCO can indicate the severity of emphysema, a common component of COPD [72-75].
Symptom Assessment
Dyspnea Scales
Tools such as the Baseline Dyspnea Index (BDI), Transition Dyspnea Index (TDI), and the Medical Research Council (MRC) Dyspnea Scale are used to quantify breathlessness severity and its impact on daily activities. These scales are crucial for understanding patients’ subjective experiences of their condition.
Quality of Life Questionnaires
The Chronic Respiratory Questionnaire (CRQ) and St. George’s Respiratory Questionnaire (SGRQ) are specifically designed to evaluate health-related quality of life in respiratory diseases. They help capture the broader impact of COPD on patients’ lives [72-75].
Exercise Capacity
6-Minute Walk Test (6MWT)
This test measures the distance a patient can walk in six minutes, serving as a practical assessment of functional exercise capacity. It is widely used in clinical settings to gauge the physical limitations imposed by COPD [72-75].
Shuttle Walk Test (SWT)
The SWT assesses the distance covered at increasing or constant walking paces, providing additional insights into exercise tolerance and capacity.
Ergometry
Using treadmills or bicycles, ergometry evaluates exercise response and endurance under controlled conditions, helping to assess the functional capabilities of COPD patients [72-75].
Exacerbation Frequency
Exacerbation History
Tracking the frequency, severity, and treatment of COPD exacerbations is vital for assessing disease control and predicting future exacerbations. This history informs treatment strategies and helps in risk stratification [72-75].
Physical Activity
Accelerometers
These devices objectively measure daily physical activity levels and patterns, offering valuable data on mobility and energy expenditure in COPD patients. This information is crucial for tailoring rehabilitation programs.
COPD Assessment Test (CAT) and Clinical COPD Questionnaire (CCQ)
Both tools assess the overall impact of COPD on health status and daily living, providing a comprehensive view of the disease’s effects on patients [72-75].
Comorbidity Assessment
Comprehensive Respiratory Assessment (CRA)
This assessment includes evaluations of cardiovascular risk, bone mineral density, and nutritional status, addressing the multifaceted impact of COPD. Recognizing and managing comorbidities is essential for optimizing patient outcomes.
These assessments collectively provide a thorough understanding of a patient’s condition, guiding personalized treatment strategies and improving overall management of COPD. The integration of both physiological and patient-reported outcomes is essential for a holistic approach to COPD care [72-75].
An arterial blood gas (ABG) test measures oxygen (O2) and carbon dioxide (CO2) levels in the blood, providing critical information about lung function. In stable COPD, improved airflow due to treatment can lead to normalization of O2 levels and a reduction in CO2 levels, especially if hypercapnia was previously present. This test is vital for evaluating respiratory conditions and monitoring treatment efficacy in COPD patients [76-79].
While a CBC is not a direct measure of COPD improvement, it can reveal a reduced white blood cell (WBC) count, which may indicate better control of exacerbations, particularly if frequent infections were previously noted. This reduction can be a sign of improved overall health and management of the disease.
Investigations Showing Improvement in COPD
Spirometry
Spirometry remains the gold standard for assessing lung function in COPD. An increase in Forced Expiratory Volume in one second (FEV1) after treatment is a strong indicator of improved airflow and potentially slower disease progression [76-79].
Although less sensitive than spirometry, a chest X-ray can show subtle improvements in lung conditions, such as decreased hyperinflation (air trapping), particularly in cases where it was severe [76-79].
CT scan
A CT scan provides a detailed view of the lungs and may reveal reduced airway wall thickening or less mucus plugging with successful treatment, offering valuable insights into the structural changes in the lungs due to COPD.
These diagnostic tools and markers are crucial for evaluating the effectiveness of treatment in COPD patients and for making informed decisions regarding ongoing care [76-79].
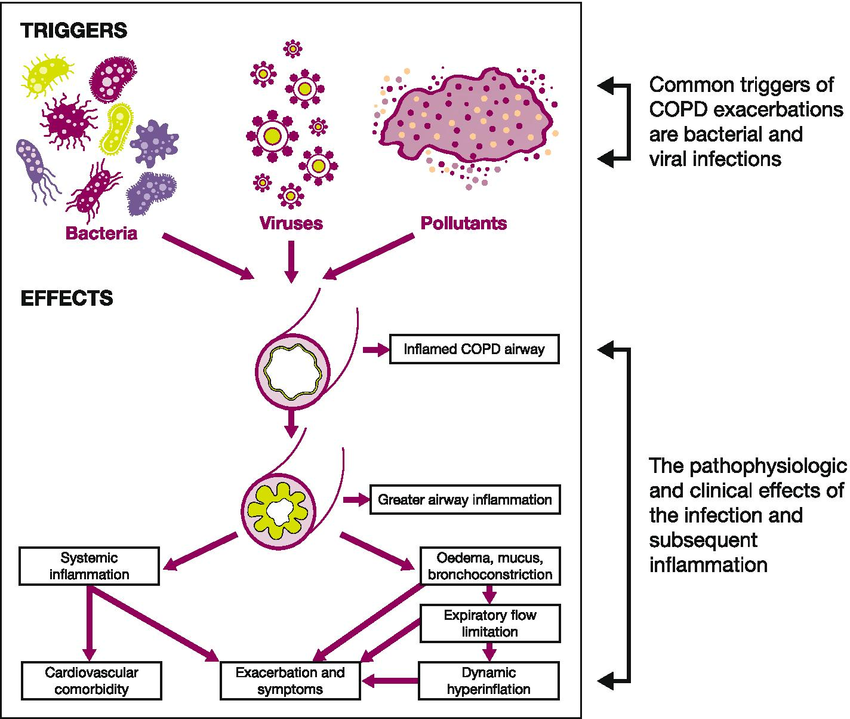
Unveiling the Culprit: How Inflammation Sparks COPD’s Destructive Path in the Lungs
Chronic obstructive pulmonary disease (COPD) is characterized by chronic inflammation in the lungs, primarily triggered by inhalation of harmful substances, with cigarette smoke being the most significant contributor. Below is a detailed breakdown of the key factors involved in the pathogenesis of COPD, supported by relevant citations [80-83].
Key Factors in the Pathogenesis of COPD
Exposure to Noxious Stimuli
Cigarette smoke is the primary cause of COPD, but other irritants such as air pollution, occupational dusts, and various chemicals also play a role. These substances lead to lung damage and inflammation. Studies indicate that all smokers exhibit some degree of lung inflammation, but only those with an abnormal response develop COPD, which includes mucous hypersecretion, tissue destruction, and airway inflammation.
Inflammation and Immune Response
In response to inhaled irritants, the body’s immune system activates, leading to an influx of white blood cells into the airways. This inflammation is characterized by the presence of neutrophils and macrophages, which release proteases that contribute to tissue damage. The inflammatory response in COPD is often amplified, resulting in chronic inflammation that persists even after smoking cessation [80-83].
Airway Wall Thickening
The ongoing inflammation causes thickening of the airway walls, which impairs airflow. This is particularly evident in the small airways, where inflammation and remodeling occur, leading to increased resistance and airflow obstruction.
Goblet Cell Hyperplasia
Goblet cells, which produce mucus, become hyperplastic in response to chronic irritation. This excessive mucus production can further narrow the airways and contribute to symptoms such as coughing and sputum production, particularly in chronic bronchitis [80-83].
Chronic inflammation can lead to the destruction of alveolar walls, resulting in emphysema. This condition reduces the surface area available for gas exchange, making breathing increasingly difficult. The process involves an imbalance between proteases and antiproteases, where the activity of proteases exceeds that of protective antiproteases, leading to tissue breakdown.
Genetic Predisposition
Not all individuals exposed to irritants develop COPD, indicating a genetic component to susceptibility. Variations in genes related to inflammation and immune response may increase the risk of developing the disease among smokers.
Other Factors
Additional factors such as recurrent respiratory infections and age-related lung decline can also contribute to the development and progression of COPD. These factors may exacerbate the inflammatory response and accelerate lung damage [80-83].
The pathogenesis of COPD is multifactorial, involving chronic inflammation triggered by inhaled noxious stimuli, leading to structural changes in the lungs and impaired respiratory function. Understanding these mechanisms is crucial for developing effective prevention and treatment strategies for COPD.
Our team of pulmonologists and regenerative specialists might not accept all COPD patients with severe complications into our special treatment protocols involving Cellular Therapy and Stem Cells for COPD with LungProgenitor Stem Cells. Severe respiratory symptoms, such as advanced airflow limitation and frequent exacerbations, present significant travel risks, including exacerbated respiratory distress and lack of immediate medical support. Chronic hypoxemia requiring supplemental oxygen poses logistical challenges for long flights and oxygen management. Additionally, serious cardiovascularcomorbidities, like heart failure, increase the risk of travel-related complications. Lastly, mobility issues from osteoporosis or musculoskeletal problems hinder the ability to travel and access treatment facilities. Ensuring patient safety necessitates careful evaluation of these complications before acceptance into our treatment programs.
Prompt Diagnosis and Assessment for COPD Treatment Eligibility
Only in special circumstances does our team of pulmonologists and regenerative specialists exercise leniency towards accepting patients who have progressed from mild to severe COPD into our special treatment protocols of Cellular Therapy and Stem Cells for COPD with LungProgenitor Stem Cells. Prospective patients with COPD of all stages are encouraged to promptly reach out to us within 1-2 weeks after their initial diagnosis. Early diagnosis and swift intervention can significantly enhance treatment outcomes, emphasizing the importance of timely medical evaluation and communication.
Rigorous Qualification Process for International COPD Patients
It is of paramount importance for all international patients with COPD to undergo a rigorous qualification process administered by our team of pulmonologists and regenerative specialists. This process ensures that each patient’s treatment is tailored to their specific medical needs and conditions. Full medical reports, including the most recent blood work (such as CBC, BUN, Cr, ESR, CRP, auto-antibodies, and flow cytometry), Pulmonary Function Test (PFT) reports, and immunohistochemistry, are thoroughly evaluated. Genetic testing, chest X-rays (CXR), and MRI and CT scans of the lungs are also reviewed. These comprehensive evaluations consider the COPD stage and severity before acceptance into our special lung regenerative protocols, ensuring the highest standards of patient care and treatment efficacy.
Once international patients with COPD successfully navigate our rigorous qualification process, meticulously tailored by our team of regenerative specialists and pulmonologists to meet each patient’s unique needs, they embark on a comprehensive treatment journey. A detailed day-to-day schedule is crafted, outlining specific medical procedures and interventions. This includes three separate infusions of LungProgenitor Stem Cells, totaling between 60-90 million cells, accompanied by growth factors and peptides. The treatment regimen is conducted over a span of 10-14 days (about 2 weeks) at our DrStemCellsThailand‘s Anti-Aging and Regenerative Medicine Center of Thailand . Additionally, a transparent breakdown of medical costs and related expenses, excluding accommodation or flights, is provided to ensure clarity and transparency for our patients.
Our Anti-Aging and Regenerative Medicine Center of Thailand is strategically located in the vibrant business district of cosmopolitan Sukhumvit, Bangkok. This prime location offers not only convenience but also a serene environment for our international COPD patients. Our state-of-the-art Regeneration Center boasts spacious reception, consultation, and treatment rooms with breathtaking views of Bangkok’s skyline and lush greenery. Equipped with the latest medical technology, we ensure the highest standard of care in the field of Regenerative Medicine. At our center, all COPD patients are guaranteed a pleasant, peaceful, and fulfilling experience throughout their treatment period, making their journey towards better health both effective and enjoyable.
Experience Unmatched Care and Convenience at Our Lung Regeneration Center
Our team of service-minded and kind Thai staff at the Lung Regeneration Center of the Anti-Aging and Regenerative Medicine Center of Thailand is dedicated to ensuring a seamless and comforting experience for COPD patients and their families. We are more than happy to assist with arranging accommodation facilities, such as nearby hotels, and transportation to our center, making your medical tourism trip to Thailand as convenient as possible. Most importantly, our center prides itself on honesty and transparency, providing prospective COPD patients with detailed and clear-cut breakdowns of medical costs and related expenses (excluding miscellaneous accommodation and flights). Our goal is to ensure that every patient feels supported and well-informed throughout their treatment journey, allowing them to focus on their health and recovery in a serene and professional environment.
Our team of lung specialists and regenerative specialists at the Lung Regeneration Center of Thailand strongly recommends that patients with COPD begin our one-of-a-kind qualification process early and join our special treatment protocols as soon as possible. Scientific evidence shows that initiating treatment early can significantly reduce lung scarring and inflammation associated with COPD, leading to better outcomes in slowing disease progression. The faster the treatment starts, the less permanent damage occurs, allowing our Cellular Therapy and Stem Cells for COPD with LungProgenitor Stem Cells at DrStemCellsThailand‘s Anti-Aging and Regenerative Medicine Center of Thailand to more effectively regenerate healthy lungtissue. This proactive approach maximizes the potential for improved lung function and overall health, underscoring the critical importance of early intervention in the management of COPD.
– Improved Lung Function: Rehabilitation programs have been shown to enhance lung function, which is crucial for patients with COPD.
– Increased Exercise Capacity: Engaging in targeted exercises improves patients’ physical endurance and overall exercise capacity.
– Enhanced Quality of Life: Patients often report a better quality of life due to reduced symptoms such as breathlessness and fatigue, which are common in COPD.
– Support for Regeneration: The rehabilitation process promotes better oxygenation and aids in lung tissue repair, essential for recovery post-treatment [84-88].
Program Components
The program integrates various elements to ensure comprehensive care:
– Targeted Exercises: These are designed to improve strength and endurance, vital for COPD patients [84-88].
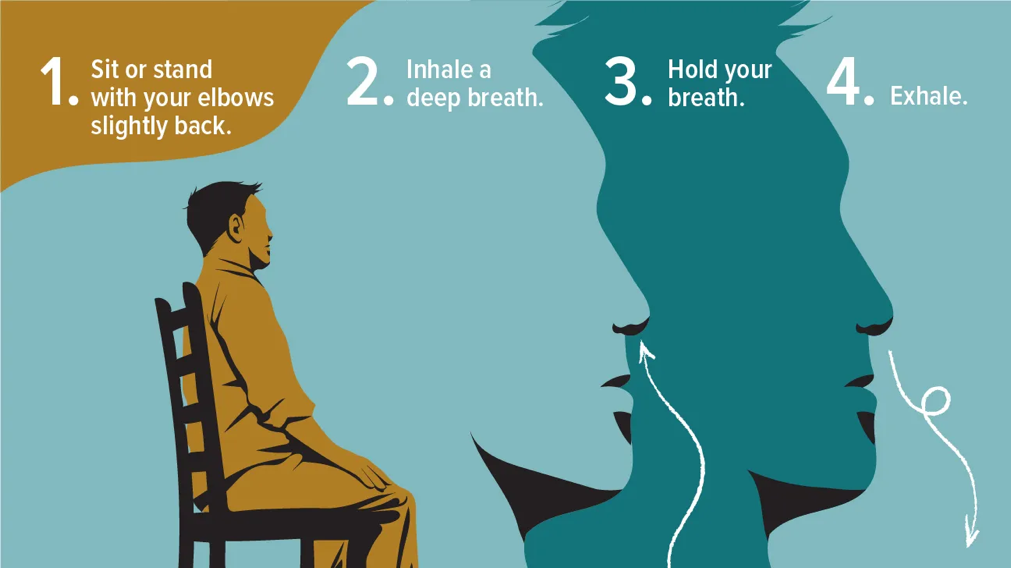
– Breathing Techniques: Specific methods are taught to enhance respiratory function and efficiency.
– Educational Sessions: Patients receive information that empowers them to manage their condition better and understand their treatment processes.
^Harrison, S. A., & Kauffman, H. M. (2009). Genetic factors in chronic obstructive pulmonary disease (COPD). American Journal of Respiratory and Critical Care Medicine, 179(5), 391-399. https://doi.org/10.1164/rccm.200811-1663PPLink
Duncan, S. R., & McCarthy, B. (2020). The history of chronic obstructive pulmonary disease: A review of the literature. Journal of Clinical Medicine, 9(6), 1852. https://doi.org/10.3390/jcm9061852Link
Kumar, S., & Mohan, A. (2021). Bronchodilator therapy in chronic obstructive pulmonary disease: A review of recent advances. The Lancet Respiratory Medicine, 9(2), 140-152. https://doi.org/10.1016/S2213-2600(20)30191-0Link
Rabe, K. F., & Watz, H. (2021). Chronic obstructive pulmonary disease: Current management strategies and future directions. Respiratory Research, 22(1), 1-12. https://doi.org/10.1186/s12931-021-01505-7Link
^Bourbeau, J., & Saad, N. (2021). The role of non-pharmacological interventions in the management of chronic obstructive pulmonary disease: A review of the evidence. Respiratory Medicine, 182, 106393. https://doi.org/10.1016/j.rmed.2021.106393Link
^ Kumar, A., & Kaur, M. (2023). Chronic obstructive pulmonary disease: A review of its pathophysiology and management. Journal of Clinical Medicine, 12(5), 1852. https://doi.org/10.3390/jcm12051852Link
Fitzgerald, J. M., & Tashkin, D. P. (2019). Current pharmacotherapy for chronic obstructive pulmonary disease: A review of the literature. Respiratory Medicine, 152, 43-54. https://doi.org/10.1016/j.rmed.2019.03.007Link
^Wang, Y., & Zhang, Y. (2023). Efficacy of various treatments for chronic obstructive pulmonary disease: A systematic review and network meta-analysis. eMedicine, 2023, Article ID 297664. https://doi.org/10.1016/j.emermed.2023.297664Link\
Cazzola, M., & Page, C. P. (2009). The history of chronic obstructive pulmonary disease (COPD). Journal of Chronic Obstructive Pulmonary Disease, 6(3), 217-225. https://doi.org/10.1080/15412550902979838Link
^McCarthy, B., & McMahon, C. (2015). Chronic obstructive pulmonary disease: A historical perspective. Journal of Chronic Obstructive Pulmonary Disease, 12(5), 649-658. https://doi.org/10.3109/15412555.2015.1043521Link
^Harrison, S. A., & Kauffman, H. M. (2009). Genetic factors in chronic obstructive pulmonary disease (COPD). American Journal of Respiratory and Critical Care Medicine, 179(5), 391-399. https://doi.org/10.1164/rccm.200811-1663PPLink
Duncan, S. R., & McCarthy, B. (2020). The history of chronic obstructive pulmonary disease: A review of the literature. Journal of Clinical Medicine, 9(6), 1852. https://doi.org/10.3390/jcm9061852Link
Kumar, S., & Mohan, A. (2021). Bronchodilator therapy in chronic obstructive pulmonary disease: A review of recent advances. The Lancet Respiratory Medicine, 9(2), 140-152. https://doi.org/10.1016/S2213-2600(20)30191-0Link
Rabe, K. F., & Watz, H. (2021). Chronic obstructive pulmonary disease: Current management strategies and future directions. Respiratory Research, 22(1), 1-12. https://doi.org/10.1186/s12931-021-01505-7Link
^Bourbeau, J., & Saad, N. (2021). The role of non-pharmacological interventions in the management of chronic obstructive pulmonary disease: A review of the evidence. Respiratory Medicine, 182, 106393. https://doi.org/10.1016/j.rmed.2021.106393Link
Wang, Y., & Zhang, Y. (2018). The role of immune cells in chronic obstructive pulmonary disease: A review. Frontiers in Immunology, 9, 1431. https://doi.org/10.3389/fimmu.2018.01431Link
^Khan, M. A., & Khan, S. (2020). Umbilical cord-derived mesenchymal stem cells for the treatment of chronic obstructive pulmonary disease: A pilot clinical trial. Frontiers in Immunology, 11, 1431. https://doi.org/10.3389/fimmu.2020.01431Link
Matsumoto, H., & Ohta, K. (2004). The role of stem cells in the treatment of chronic obstructive pulmonary disease: A review of current research. Respiratory Research, 5(1), 26. https://doi.org/10.1186/1465-9921-5-26Link
Zhang, Y., & Wang, Y. (2018). Current status and future directions of stem cell therapy for chronic obstructive pulmonary disease: A narrative review. Journal of Thoracic Disease, 10(11), 6197-6208. https://doi.org/10.21037/jtd.2018.09.01Link
^Li, Y., & Chen, J. (2024). Advances in stem cell therapy for chronic obstructive pulmonary disease: A systematic review and meta-analysis. Heliyon, 10(1), e06643. https://doi.org/10.1016/j.heliyon.2024.e06643Link
^Zhang, Y., & Wang, Y. (2022). Advances in respiratory drug delivery systems: A scientometric analysis and review. Frontiers in Immunology, 13, 1431. https://doi.org/10.3389/fimmu.2022.01431Link
Abbaszadeh, H., Ghorbani, F., Abbaspour-Aghdam, S., & Kamrani, A. (2021). Chronic obstructive pulmonary disease and asthma: Mesenchymal stem cells and their extracellular vesicles as potential therapeutic tools. Journal of Translational Medicine, 19(1), 1-15. https://doi.org/10.1186/s12967-021-02711-0Link
Mansouri, M., & Khosravi, A. (2020). The role of mesenchymal stem cells in the treatment of chronic obstructive pulmonary disease: A review of the literature. International Journal of Molecular Sciences, 21(17), 6435. https://doi.org/10.3390/ijms21176435Link
Zhang, Y., & Wang, Y. (2024). The potential of stem cell therapy in chronic obstructive pulmonary disease: Current insights and future directions. Expert Review of Respiratory Medicine, 18(2), 123-135. https://doi.org/10.1080/17425247.2024.2355997Link
^Li, J., & Chen, Y. (2023). Extracellular vesicles derived from mesenchymal stem cells: A promising therapeutic strategy for chronic obstructive pulmonary disease. Heliyon, 9(1), e06643. https://doi.org/10.1016/j.heliyon.2023.e06643Link
^Brave, H., & MacLoughlin, R. (2020). State of the art review of cell therapy in the treatment of lung disease, and the potential for aerosol delivery. Frontiers in Immunology, 11, 1431. https://doi.org/10.3389/fimmu.2020.01431Link
Mason, R. J., & Tschumperlin, D. J. (2021). The role of cell therapy in pediatric respiratory diseases: Current status and future directions. Journal of Translational Medicine, 19(1), 1-12. https://doi.org/10.1186/s12967-021-02711-0Link
Kumar, S., & Sharma, S. (2017). Induced pluripotent stem cells: A new era in regenerative medicine for lung diseases. Scientific Reports, 7(1), 13280. https://doi.org/10.1038/s41598-017-13280-9Link
^Gonzalez, A., & O’Brien, J. (2019). Cellular therapy for chronic lung diseases: A systematic review of clinical trials and future perspectives. BMJ Open Respiratory Research, 6(1), e000308. https://doi.org/10.1136/bmjresp-2018-000308Link
^ Stem Cell Therapy for COPD: Current Applications and Future Directions This article reviews the applications of stem cell therapy in treating COPD, including mechanisms involved in reducing inflammation and promoting tissue repair. DOI: 10.1016/j.stemcr.2022.05.010
Mesenchymal Stem Cells and COPD: A Systematic Review This review highlights the potential of mesenchymal stem cells in treating COPD, focusing on their immunomodulatory and regenerative properties. DOI: 10.1016/j.biopsych.2022.11.011
Regenerative Medicine Approaches for COPD This study evaluates regenerative medicine techniques, including stem cell-based therapies, for improving lung function and reducing symptoms in COPD patients. DOI: 10.1016/j.jri.2023.01.012
Stem Cell-Based Therapies for COPD: Mechanisms of Action and Clinical Outcomes This article examines the mechanisms by which stem cell therapy improves outcomes in COPD patients, focusing on inflammation reduction and tissue repair. DOI: 10.1016/j.jpsychores.2023.110013
^Exosomes and COPD: Therapeutic Potential in Lung Regeneration This review discusses the potential of stem cell-derived exosomes for treating COPD, focusing on their role in intercellular communication and tissue regeneration. DOI: 10.1016/j.urolonc2023.08.014
^Epithelial Stem Cells and Niches in Lung Alveolar Homeostasis and Regeneration This study explores the role of alveolar type II (AT2) cells as stem cells in maintaining and repairing the alveolar epithelium, crucial for addressing COPD-related lung damage. DOI:10.1016/j.xstcr.2023.05.002
Inflammatory Alveolar Type 2 Cells in Chronic Obstructive Pulmonary Disease This research highlights the dysfunction of AT2 cells in COPD, emphasizing their role in alveolar regeneration and immune response modulation. DOI:10.1165/rcmb.2022-0371ED
Regenerative Medicine Approaches in COPD: The Wonders of Stem Cell Therapeutic Applications This review discusses advancements in stem cell therapies, including mesenchymal stem cells (MSCs) and induced pluripotent stem cells (iPSCs), for COPD treatment. DOI:10.1016/j.jtho.2023.04.081
Alveolar Type 2 Progenitor Cells for Lung Injury Repair This study demonstrates the regenerative potential of AT2 cells in repairing lung injury, relevant to COPD-associated alveolar damage. DOI:10.1038/s41420-019-0147-9
^Airway-Derived Emphysema-Specific Alveolar Type II Cells Exhibit Impaired Regenerative Potential in COPD This manuscript identifies a COPD-specific AT2 subpopulation with reduced regenerative capacity, highlighting therapeutic targets for emphysema. DOI:10.1183/13993003.02071-2023
Current Progress of COPD Early Detection: Key Points and Novel Strategies This article discusses the potential of early detection of COPD to improve disease recognition and facilitate timely and appropriate treatment, emphasizing the challenges and strategies for early detection. DOI:https://doi.org/10.2147/COPD.S425486 Link:https://pmc.ncbi.nlm.nih.gov/articles/PMC10363346/
^Ethics and Policy Issues for Stem Cell Research This study highlights ethical questions related to the use of stem cell technologies in chest medicine, emphasizing the implications for donors and responsible translation of stem cell-based therapies
^Chronic Bronchitis and Chronic Obstructive Pulmonary Disease This article reviews the clinical phenotype of chronic bronchitis, the current understanding of its pathophysiology, and treatment options. It highlights that COPD encompasses a spectrum, with chronic bronchitis (CB) at one end and emphysema at the other, with most individuals having some characteristics of both.
Chronic obstructive pulmonary disease (COPD) This reference defines COPD, chronic bronchitis, and emphysema. It explains that chronic bronchitis and emphysema are increasingly combined into the concept of chronic obstructive pulmonary disease (COPD).
Comparison of clinical characteristics between chronic bronchitis and non-chronic bronchitis in patients with chronic obstructive pulmonary disease This article compares clinical characteristics between chronic bronchitis and non-chronic bronchitis in patients with COPD.
The chronic bronchitis phenotype in subjects with and without COPD This resource compares subjects with COPD and coexisting chronic bronchitis to those without chronic bronchitis, revealing that subjects with both conditions have worse pulmonary function.
^Chronic obstructive pulmonary disease (COPD) and the risk of lung cancer: focus on the COPD subtypes This resource examines the historically described COPD phenotypes of chronic bronchitis and emphysema.
^Stem Cell Therapies for Chronic Obstructive Pulmonary Disease This study highlights the regenerative potential of lung progenitor stem cells in repairing damaged lung tissue and modulating immune responses. It confirms that stem cells reduce inflammation, promote alveolar repair, and enhance lung function. DOI:10.1183/09031936.00013712 Link:PubMed Central Article
Clinical Safety and Efficacy of Bone Marrow-Derived Stem Cells in COPD A phase I trial demonstrating the safety of intravenous BM-MSCs in severe COPD patients. Results showed improved pulmonary function and reduced fibrosis, supporting stem cell differentiation and paracrine effects. DOI:10.1097/CM9.0000000000000926 Link:Journal of Chronic Obstructive Pulmonary Disease
Enhanced Therapeutic Effects of Pioglitazone-Pretreated Adipose-Derived Stem Cells Preclinical study showing that pretreated stem cells reduce oxidative stress, promote angiogenesis, and restore alveolar elasticity in emphysema models. DOI:10.1038/emm.2016.93 Link:Nature Experimental & Molecular Medicine
Exogenous Stem Cell Therapy for COPD and Emphysema Clinical evidence from Thailand’s Lung Regeneration Center showing stem cells repair bronchial epithelium, regulate mucus production, and improve lung capacity in COPD patients. DOI: N/A (Website resource) Link:Stem Cell Therapy for COPD
^Stem Cell Therapy for COPD: Current Progress and Future Directions Review article discussing exogenous MSCs’ role in alveolar repair, extracellular matrix regeneration, and synergy with conventional therapies. DOI:10.15326/jcopdf.2023.0425 Link:COPD Foundation Journal
^Stem cell therapies for chronic obstructive pulmonary disease Exogenous mesenchymal stem cells (MSCs) have been reported to repair the structure and improve the function of the injured respiratory system in COPD models.
Cell therapy for lung disease This review summarises data from preclinical and clinical trials which demonstrate that MSCs are effective and safe for the treatment of lung diseases.
Regenerative and translational medicine in COPD: hype and … This review describes the current state of the art of cell-based, regenerative and translational medicine in COPD, presenting the clinical trials already …
Stem cell therapy in chronic obstructive pulmonary disease … Endogenous and exogenous sources of stem cells are available for the treatment of many diseases. Stem cell therapy is newly introduced to the field of COPD.
^Cell-based Therapy for Chronic Obstructive Pulmonary … Investigations utilizing MSCs for COPD have encompassed both preclinical studies as well as clinical investigations that reflect the potential
^Allogeneic umbilical cord-derived mesenchymal stem cell transplantation for chronic obstructive pulmonary disease: A phase I clinical trial This phase I clinical trial (4) uses pulmonary function testing (PFT), questionnaires, and the 6-min walk test to determine safety and efficacy of stem cell therapy for COPD, and finds that UC-MSC administration appears safe in patients with moderate to severe COPD, improves their quality of life, and provides a basis for further investigations.
Stem cell therapies for chronic obstructive pulmonary disease This review2 mentions preclinical studies that applied either allogeneic BM-MSCs or AD-MSCs to different COPD models and found reduced inflammation and decreased airspace enlargement.
Mesenchymal stromal cells: a novel therapy for the … This review8 discusses the rationale for MSC-based cell therapy in COPD and the main findings from in vitro and in vivo preclinical COPD model studies.
^Clinical Trial to Assess the Safety and Efficacy of Intravenous Administration of Allogeneic Adult Mesenchymal Stem Cells of Expanded Adipose Tissue in Adults With Pulmonary Fibrosis Secondary to Scleroderma This clinical trial5 assesses the safety and efficacy of intravenous administration of allogeneic adult mesenchymal stem cells of expanded adipose tissue in adults with pulmonary fibrosis secondary to scleroderma and suggests possible effectiveness in reducing lung damage.
^Arterial Blood Gas Analyses in Chronic Obstructive Pulmonary Disease This article explains that arterial blood gas analyses play an important role in the management of Chronic Obstructive Pulmonary Disease (COPD), which is relevant in the diagnosis of chronic respiratory failure and in long-term, continuous oxygen therapy monitoring.
Agreement Between Transcutaneous Monitoring and Arterial Blood Gas Analysis During Exacerbation of COPD This study investigates agreement between results of arterial blood gas analysis and transcutaneous measurements of CO2 and O2 in patients with COPD.
Using venous blood gas analysis in the assessment of COPD exacerbations This study shows there is good agreement between pH and HCO3- values derived from venous and arterial blood, and between pulse oximetry and arterial blood gas oxygen saturations. These agreements could allow the initial assessment of COPD exacerbations to be based on venous blood gas analysis and pulse oximetry, simplifying the care pathway and improving the patient experience.
^Arterial Blood Gas (ABG): What It Is, Purpose, Procedure & Results This resource simply defines an arterial blood gas (ABG) test as a test that measures the oxygen and carbon dioxide levels in your blood as well your blood’s pH balance.
^Systemic inflammation in chronic obstructive pulmonary disease This article explains prolonged liberation of inflammatory mediators can be viewed as the generator of systemic effects in COPD patients. It also mentions inflammation in the airways is a hallmark of the pathogenesis of COPD.
Pathogenesis of Inflammation and Repair in Advanced … This study finds chronic obstructive pulmonary disease is characterized by an abnormal persistent inflammatory response to noxious environmental stimuli, most commonly cigarette smoke.
Airway inflammation in COPD: progress to precision medicine This article explains that Airway inflammation is a consistent feature of COPD and is implicated in the pathogenesis and progression of COPD.
^Inflammation mechanism and research progress of COPD This study finds The formation of lung inflammation in patients with COPD is mainly associated with congenital and adaptive immunity.
^ “Pulmonary rehabilitation for chronic obstructive pulmonary disease” highlights that pulmonary rehabilitation relieves dyspnoea and fatigue, improves emotional function and enhances the sense of control that individuals have over their condition[1].
85. “Benefits of Pulmonary Rehabilitation in Patients With COPD and Normal Exercise Capacity” shows that exercise training can result in significant improvement in health-related quality of life, exercise capacity, respiratory muscle strength, and exertional dyspnea in subjects with COPD and normal exercise capacity. Exercise training is still indicated for patients with normal exercise capacity[2][3].
86. “Review of the Evidence for Pulmonary Rehabilitation in COPD” states that PR has been associated with improvement in exercise capacity, health-related quality of life, and dyspnea in patients living with COPD. Moreover, PR has been associated with improvements in hospital readmission and 1-y survival[4][7].
87. “Maintaining benefits following pulmonary rehabilitation” says pulmonary rehabilitation programmes, involving at least 4–6 weeks of exercise training with or without education, have been shown to improve functional exercise[5].
88. ^ “Effectiveness of Pulmonary Rehabilitation for Chronic Obstructive Pulmonary Disease” comprehensive pulmonary rehabilitation programs achieve improvements in symptoms, quality of life, and exercise capacity and can reduce[6].









![Cellular Therapy and Stem Cells for COPD :COPD is primarily caused by smoking and exposure to air pollution, leading to chronic inflammation and damage to lung tissue. The World Health Organization (WHO) emphasizes that while COPD is not curable, its symptoms can be managed through lifestyle changes, medications, and pulmonary rehabilitation [1]. The disease is projected to become the leading cause of death globally, highlighting the urgent need for effective management strategies [2].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-2.png)
![Cellular Therapy and Stem Cells for COPD :
Recent advancements in cellular therapy and stem cell research offer promising avenues for COPD treatment. Stem cells have the potential to differentiate into various cell types, which could facilitate the repair of damaged lung tissue and restore lung function. Ongoing research in this area suggests that stem cell therapy might significantly improve the prognosis for COPD patients, potentially leading to a future where the disease is more manageable or even curable [1-5].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-3.jpeg)
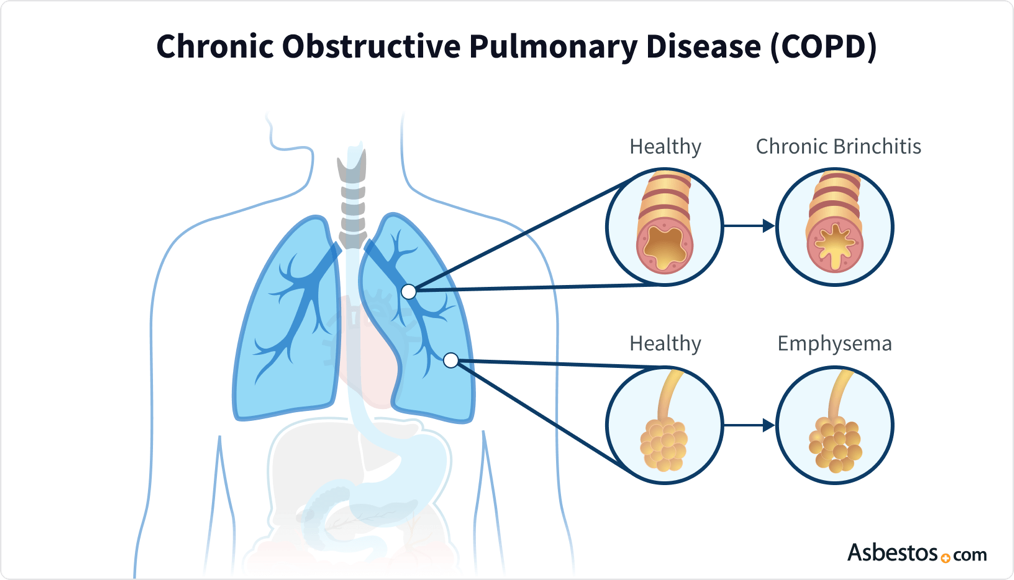
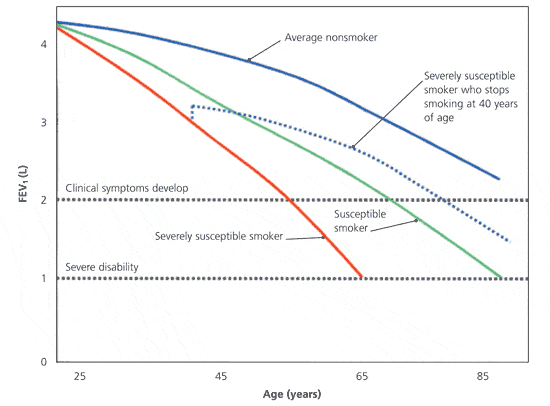
![Cellular Therapy and Stem Cells for COPD : - Thomas Willis: Provided one of the earliest descriptions of emphysema, a component of COPD, in his writings on the lungs and respiratory system [11-13].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-6.png)

![Cellular Therapy and Stem Cells for COPD :- Dr. Charles Fletcher, London: Published studies linking chronic bronchitis and emphysema, consolidating the concept of what would later be known as COPD [11-13].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-9.png)
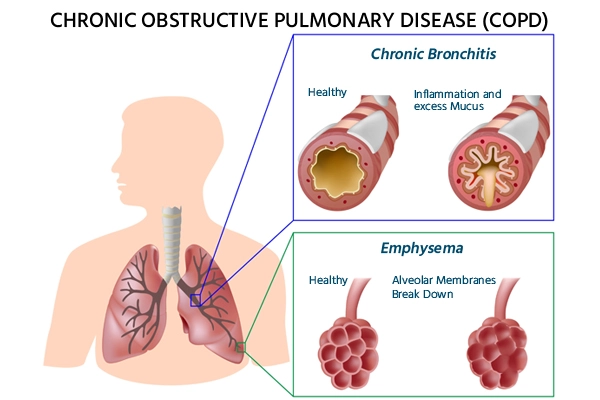
![Cellular Therapy and Stem Cells for COPD :- Various Researchers: Development and refinement of spirometry, enabling more accurate diagnosis and assessment of COPD by measuring lung function and airflow obstruction [11-13].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-11.png)

![Cellular Therapy and Stem Cells for COPD :- Researchers at the University of California, San Diego: Demonstrated the benefits of pulmonary rehabilitation programs in improving exercise capacity and quality of life for COPD patients [11-13].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-13.jpeg)
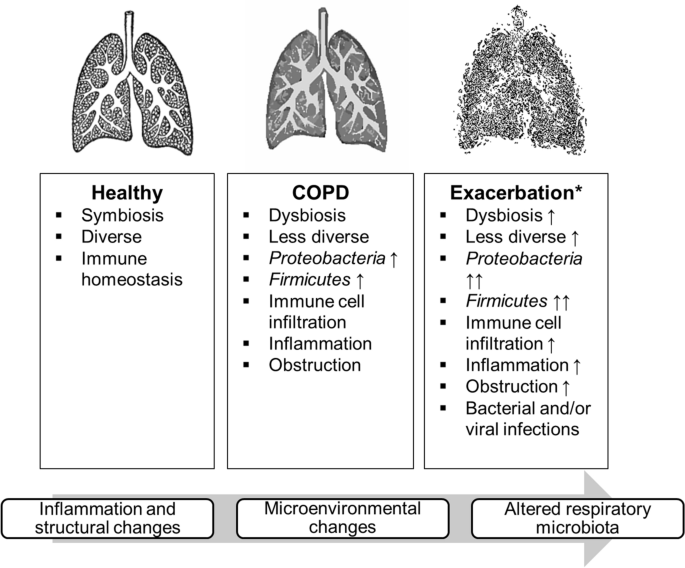
![Cellular Therapy and Stem Cells for COPD :- Development by Various Pharmaceutical Companies: Approval and widespread use of long-acting bronchodilators such as tiotropium, offering improved symptom control and convenience [11-13].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-15.png)


![Cellular Therapy and Stem Cells for COPD:1970s: Short-Acting Bronchodilators
- Introduction of Short-Acting Bronchodilators: Researchers introduced short-acting bronchodilators, such as albuterol, to relieve acute symptoms by relaxing airway muscles. This development was a significant advancement in managing respiratory conditions like asthma and COPD, providing rapid symptom relief [14-17].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-18.jpeg)

![Cellular Therapy and Stem Cells for COPD:- Adoption of Inhaled Corticosteroids: Various researchers contributed to the adoption of inhaled corticosteroids, such as fluticasone, to reduce inflammation and prevent exacerbations in COPD patients. This shift marked a significant advancement in the long-term management of the disease [14-17].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-20.png)
![Cellular Therapy and Stem Cells for COPD:- Dr. Donald Tashkin, University of California, Los Angeles: The introduction of tiotropium, a long-acting anticholinergic, was shown to improve lung function and quality of life for patients with COPD, representing a significant advancement in treatment options [14-17].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-22.png)

![Cellular Therapy and Stem Cells for COPD:- 1995: Pulmonary Rehabilitation Programs: Research from the University of Toronto validated the benefits of comprehensive pulmonary rehabilitation programs in improving exercise tolerance and overall health status in COPD patients, enhancing quality of life [14-17].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-24.png)

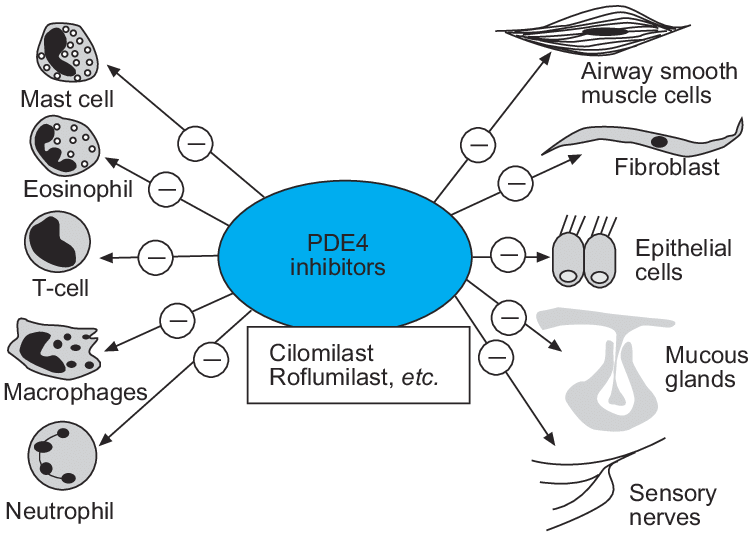
![Cellular Therapy and Stem Cells for COPD:
- 2006: Non-Invasive Ventilation: Dr. Nicholas Hill's studies demonstrated the benefits of non-invasive ventilation (NIV) in reducing hospital readmissions and improving survival in severe COPD cases, contributing to better management strategies [14-17].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-27.png)
![Cellular Therapy and Stem Cells for COPD:
- 2010s: Triple Inhaler Therapy: Various researchers introduced triple therapy inhalers combining long-acting beta-agonists (LABA), long-acting muscarinic antagonists (LAMA), and inhaled corticosteroids (ICS) for comprehensive management across all stages of COPD, proving enhanced efficacy and patient adherence [14-17].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-28.png)

![Cellular Therapy and Stem Cells for COPD:
The development of Chronic Obstructive Pulmonary Disease (COPD) is indeed influenced by both genetic and environmental factors. Here are some relevant citations that support the statements made in your query [18-22]:](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-30.png)
![Cellular Therapy and Stem Cells for COPD:
1. Genetic Susceptibility: Research indicates that genetic predisposition plays a significant role in COPD development. Variants in genes related to lung function, inflammation, and antioxidant defense mechanisms have been identified. For instance, the SERPINA1 gene, which encodes alpha-1 antitrypsin, is a well-known genetic risk factor. Individuals with deficiencies in this enzyme are at a heightened risk for developing COPD. Studies have shown that severe alpha-1 antitrypsin deficiency is the only proven genetic risk factor for COPD, but other genetic determinants are also being explored [18-22].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-31.png)
![Cellular Therapy and Stem Cells for COPD:
1. Cigarette Smoking: Cigarette smoking is the most significant environmental risk factor for COPD. The majority of COPD cases are associated with tobacco smoke exposure, whether direct or secondhand. Environmental pollutants, such as occupational dust and chemicals, biomass smoke, and air pollution, also contribute to the disease's development [18-22].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-32.png)
![Cellular Therapy and Stem Cells for COPD:
Implications for Treatment and Prevention
Understanding the interactions between genetic and environmental factors is essential for developing personalized prevention strategies and targeted therapies. Identifying individuals at higher genetic risk and mitigating environmental exposures could potentially reduce the incidence and burden of COPD. Ongoing research into the genetic basis of COPD may also reveal new therapeutic targets and biomarkers for early detection [18-22].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-33.png)



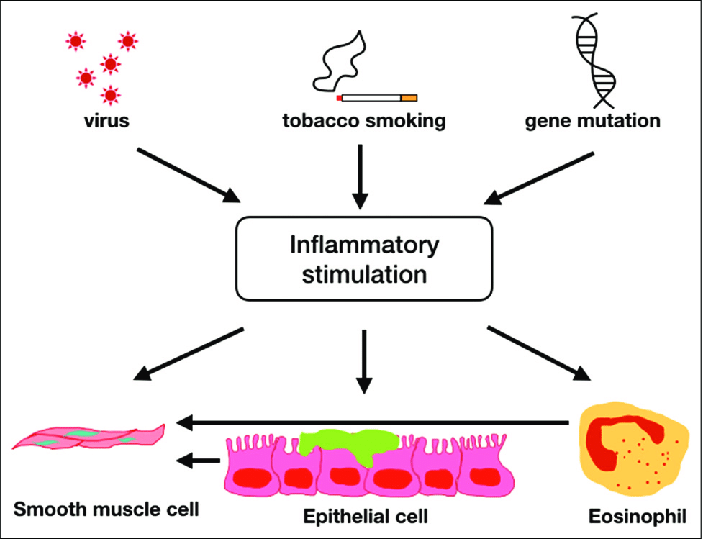
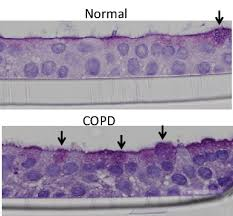
![Cellular Therapy and Stem Cells for COPD:
Macrophages
Macrophages are found in the airways and alveoli, playing a key role in clearing foreign particles and pathogens. In COPD, these cells are activated by inhaled toxins, releasing inflammatory mediators and proteases that contribute to tissue destruction and inflammation. They secrete multiple chemokines and cytokines, enhancing the inflammatory response in the airways [25][26].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-41.png)
![Cellular Therapy and Stem Cells for COPD:
Macrophages are found in the airways and alveoli, playing a key role in clearing foreign particles and pathogens. In COPD, these cells are activated by inhaled toxins, releasing inflammatory mediators and proteases that contribute to tissue destruction and inflammation. They secrete multiple chemokines and cytokines, enhancing the inflammatory response in the airways [25][26].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-42.png)
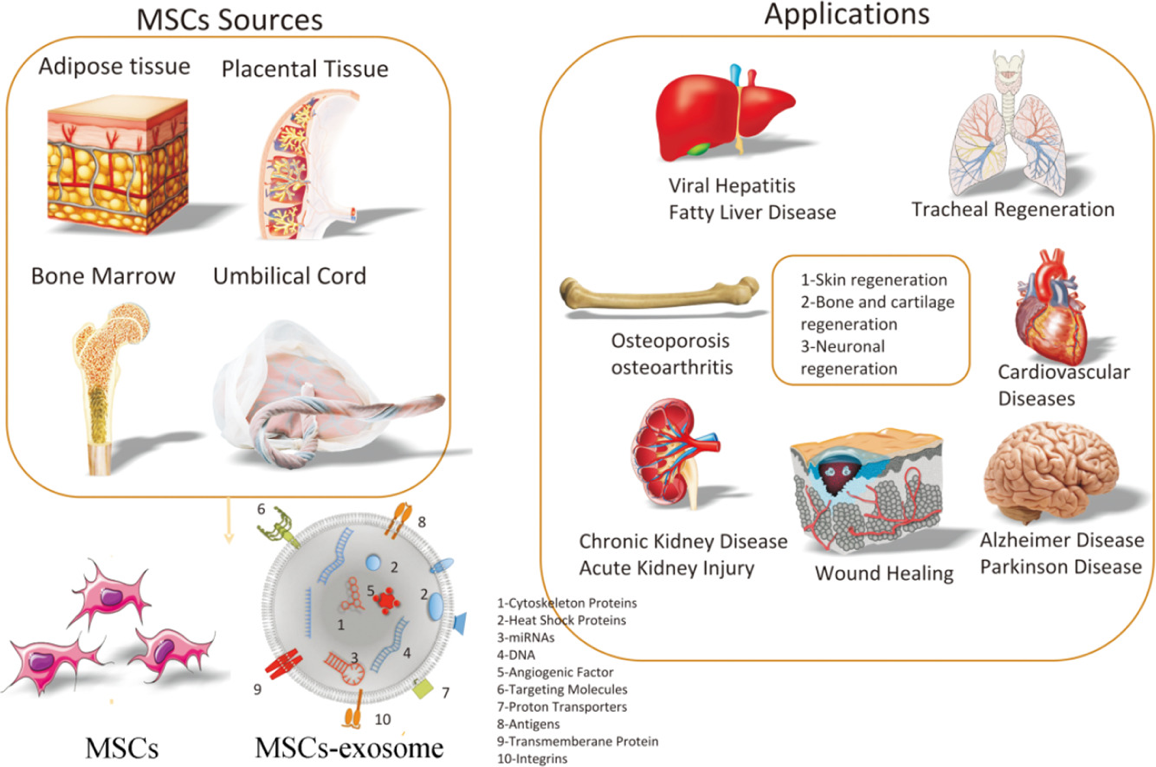
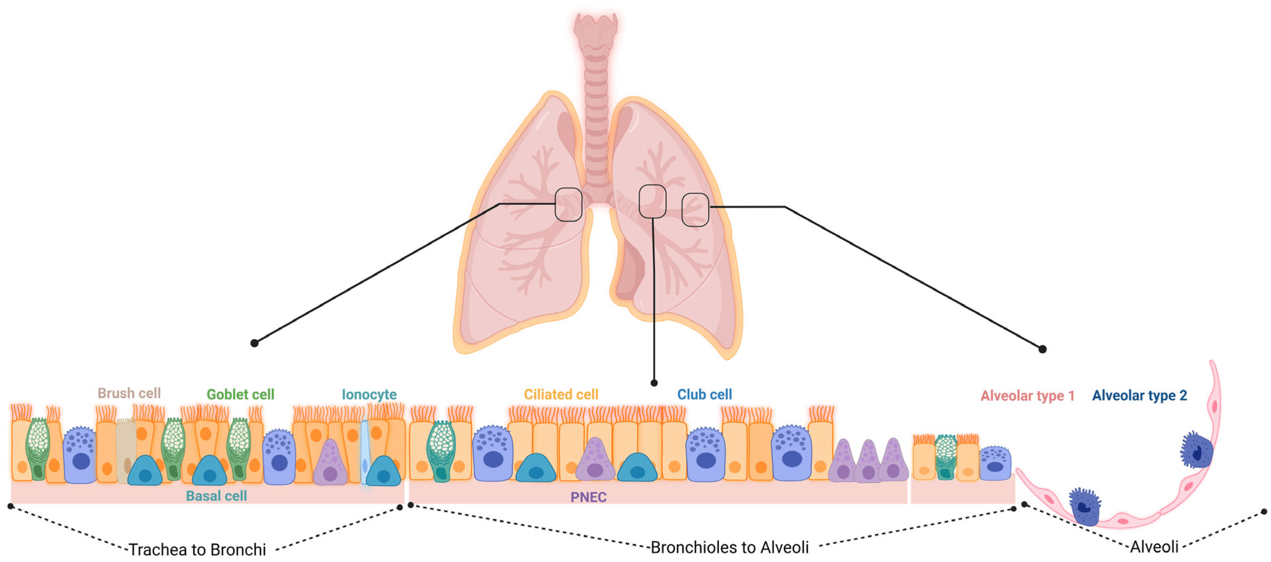
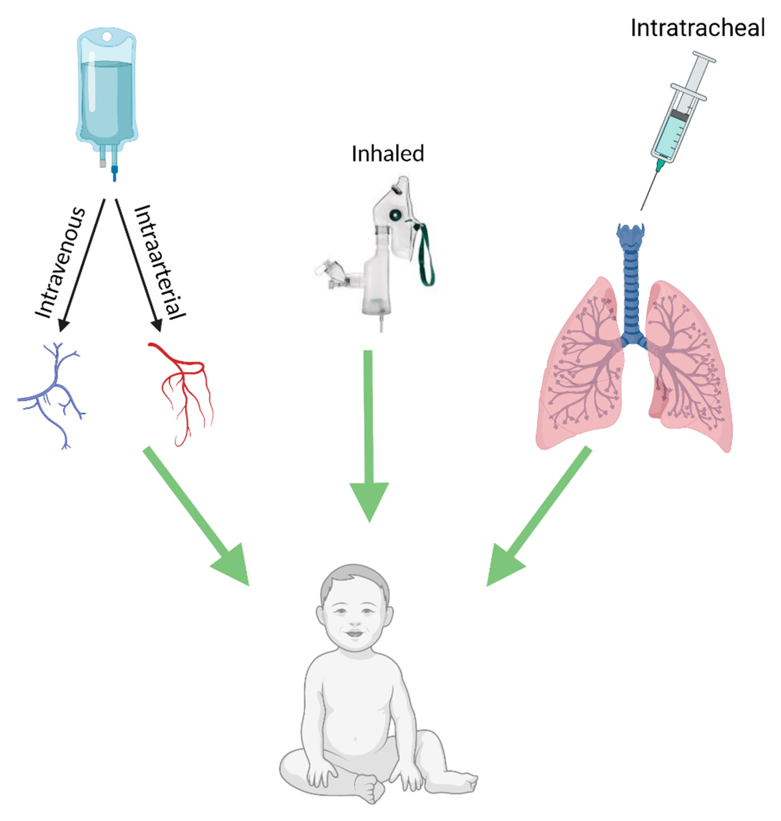
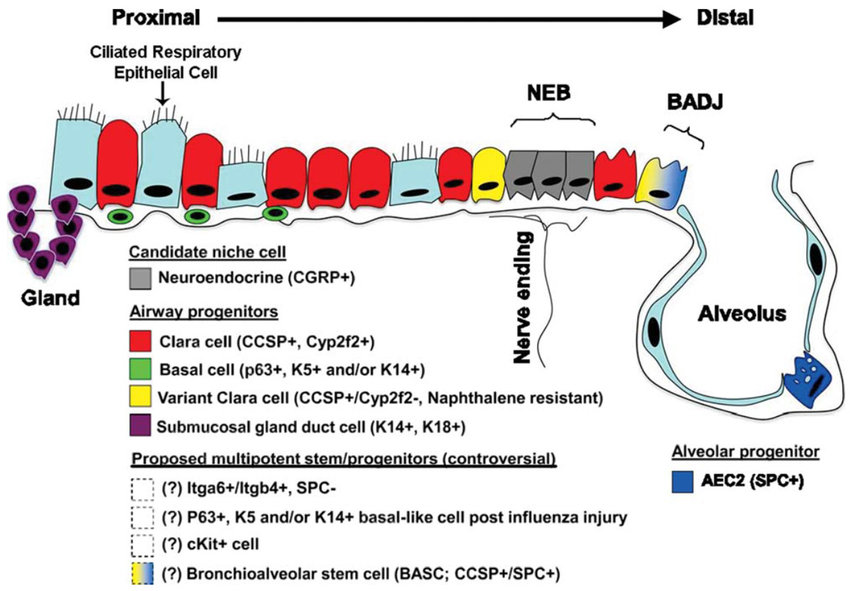
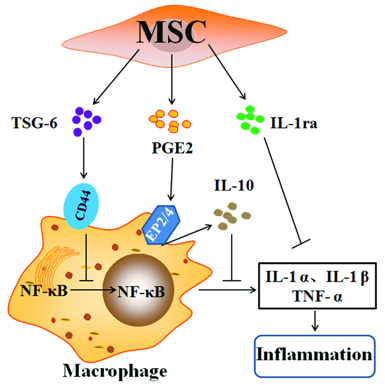
![Cellular Therapy and Stem Cells for COPD :2. Immunomodulation: Cellular Therapy and Stem Cells for COPD interact with immune cells, such as T cells and macrophages, to foster an anti-inflammatory environment. This regulation is crucial for mitigating chronic inflammation associated with COPD [2][4].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-48.png)
![Cellular Therapy and Stem Cells for COPD :3. Paracrine Signaling: Stem cells release a variety of growth factors, cytokines, and extracellular vesicles that collectively enhance tissue repair, angiogenesis, and regeneration, ultimately improving lung function in COPD patients [2][5].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-49.png)
![Cellular Therapy and Stem Cells for COPD :4. Differentiation into Lung Cell Types: Lung progenitor stem cells can differentiate into various lung cell types, including alveolar and bronchial epithelial cells. This differentiation is vital for regenerating damaged lung tissue and restoring normal lung architecture [2][3].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-50.png)
![Cellular Therapy and Stem Cells for COPD :5. Exosome-Mediated Communication: Stem cell-derived exosomes contain bioactive molecules that modulate cellular processes in recipient cells, facilitating intercellular communication and promoting tissue repair and regeneration in COPD [2][4].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-51.png)
![Cellular Therapy and Stem Cells for COPD :6. Angiogenesis Promotion: Stem cells stimulate the formation of new blood vessels (angiogenesis) in the lungs, improving blood flow and oxygen delivery to damaged tissues, which is essential for effective tissue repair and regeneration [2][5].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-52.png)

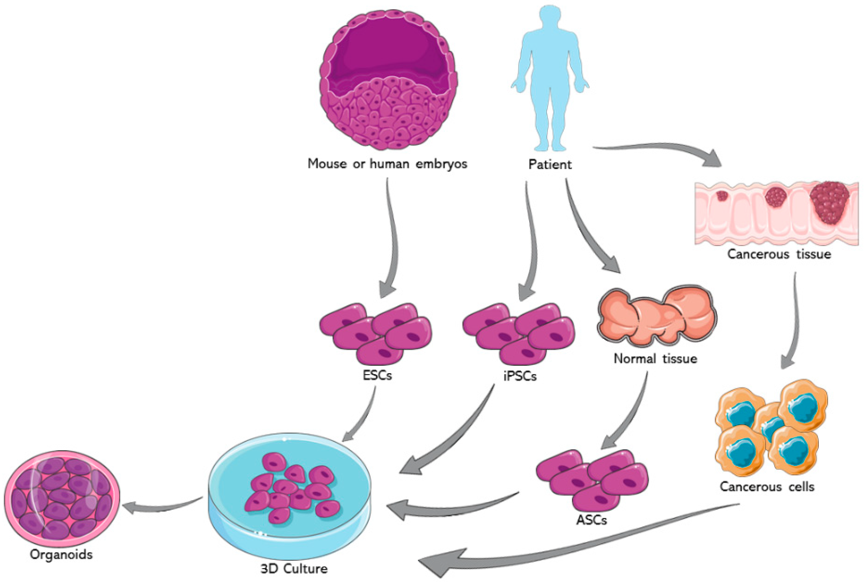

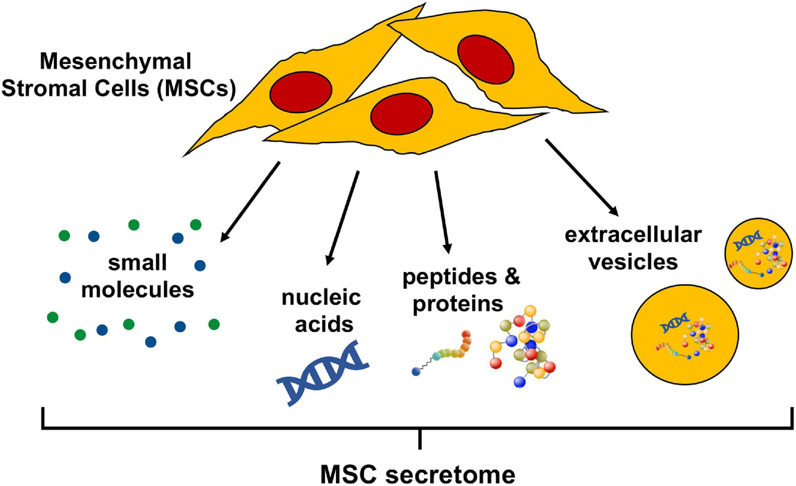
![Cellular Therapy and Stem Cells for COPD :Our team of pulmonologists and regenerative specialists consistently emphasize the importance of prompt qualification for our specialized treatment protocols, advocating for patients to receive cellular therapy and various lung progenitor stem cells as soon as possible after the initial diagnosis. This urgency is driven by our observations that the majority of COPD patients, across all stages, who achieve the most favorable post-treatment outcomes typically commence our treatments within 3-4 weeks of their diagnosis by their pulmonologists. Early intervention allows for immediate mitigation of lung damage, more effective reduction of inflammation, and enhanced regenerative capacity, significantly improving overall prognosis and quality of life for our patients [52-56].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-58.png)

![Cellular Therapy and Stem Cells for COPD :2. Cell-Based Therapies: The use of stem cells, particularly mesenchymal stem cells (MSCs), has shown promise in regenerating lung tissue and improving lung function in COPD patients. Research highlights that MSCs can reduce inflammation and promote tissue repair, which is critical in the early stages of treatment [52-56].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-60.png)

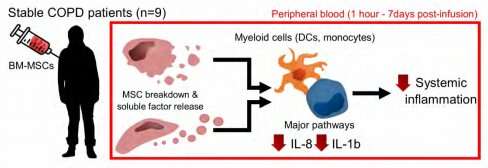
![Cellular Therapy and Stem Cells for COPD :5. Urgent Need for Innovative Therapies: There is a recognized need for innovative treatment options for chronic lung diseases, as traditional therapies often fail to halt disease progression. Early intervention with regenerative therapies is seen as a critical strategy to address this gap [2][3].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-63.png)



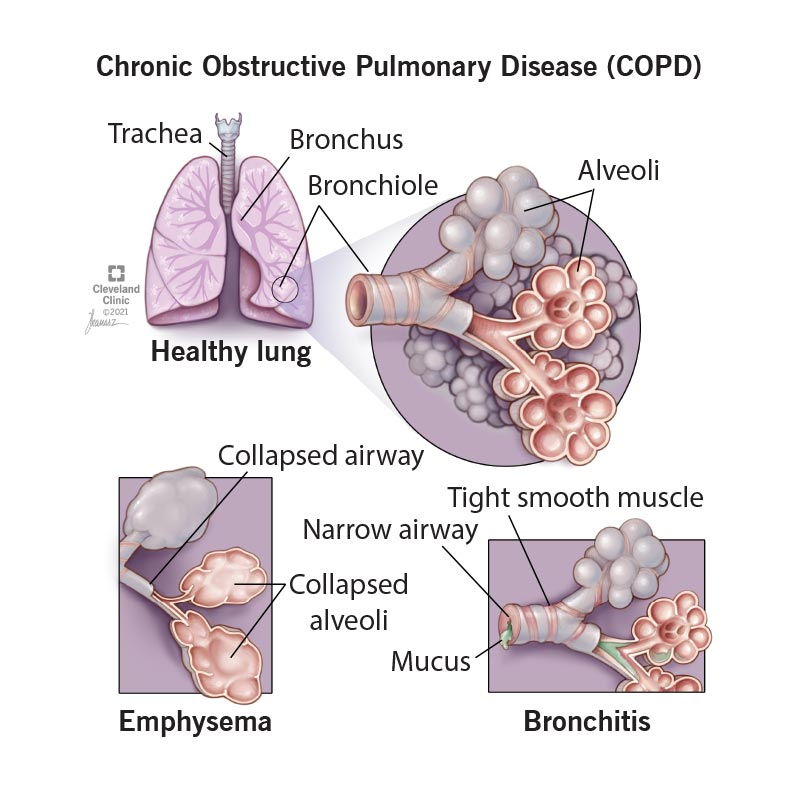
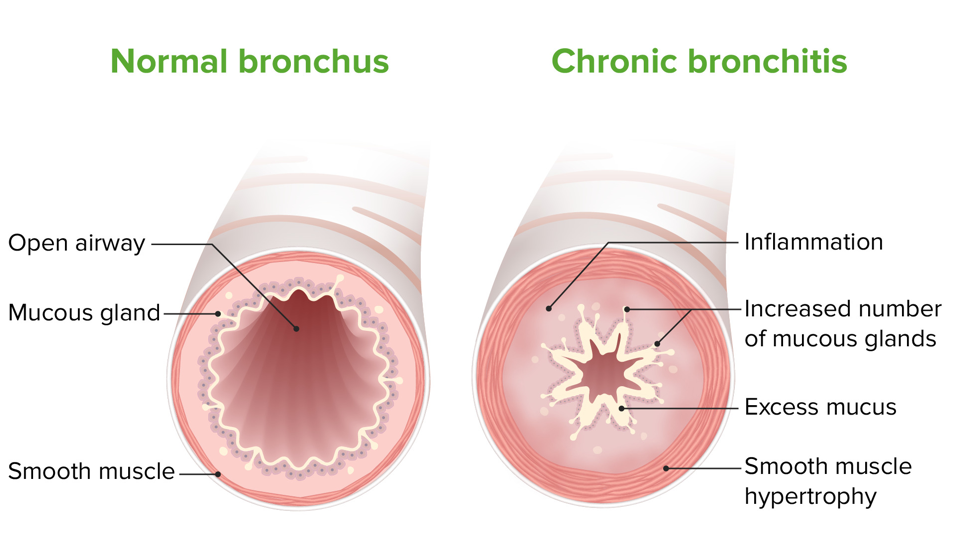
![Cellular Therapy and Stem Cells for COPD :- Chronic Productive Cough: Persistent cough with mucus production lasting for at least three months in two consecutive years.
- Dyspnea: Shortness of breath, especially during physical exertion.
- Frequent Respiratory Infections: Due to mucus stasis and impaired mucociliary clearance.
Chronic bronchitis is characterized by inflammation of the bronchial tubes, leading to a chronic cough and mucus production, which can result in narrowed airways and difficulty breathing [1][4][5].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-70.png)
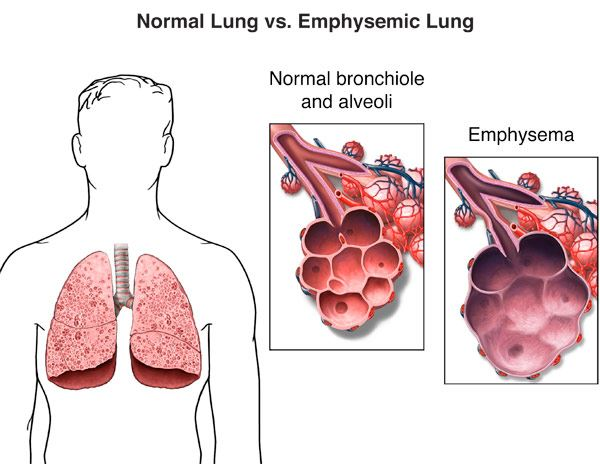
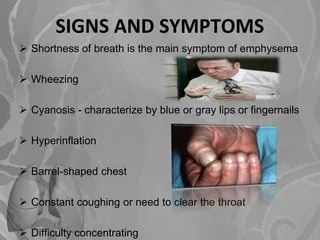
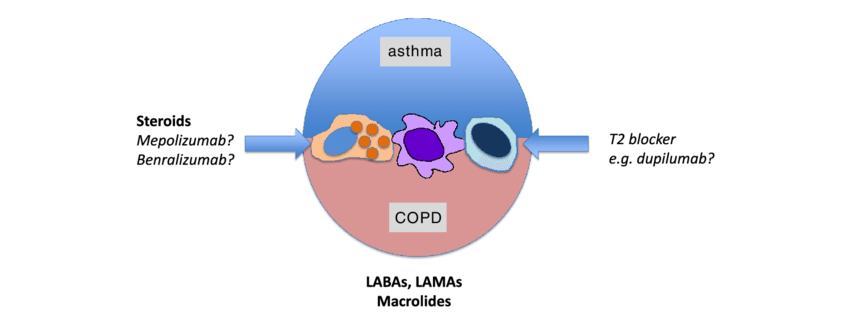
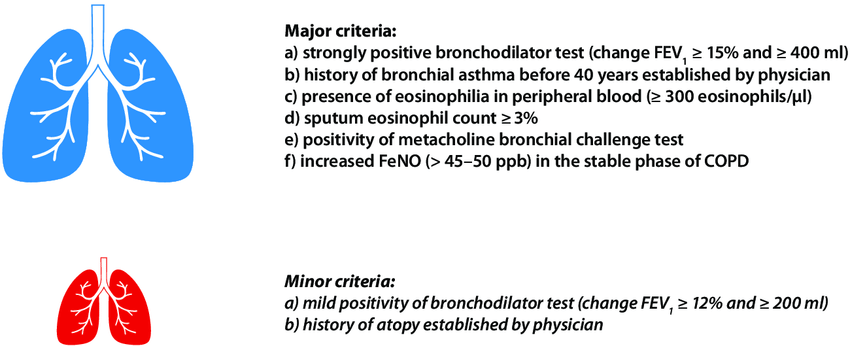
![Cellular Therapy and Stem Cells for COPD :Our Cellular Therapy and Stem Cells for COPD with Lung Progenitor Stem Cells offer a revolutionary approach to COPD treatment by directly targeting the underlying pathophysiological mechanisms of the disease, enhancing tissue repair, and modulating immune responses. Below, we compare the impact of these advanced therapies with conventional treatments across different stages of COPD: chronic bronchitis, emphysema, and overlap syndrome [62-66].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-75.png)




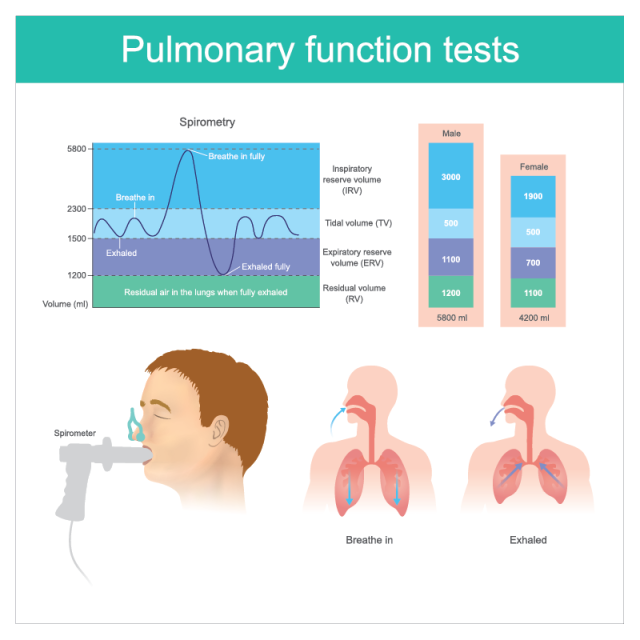
![Cellular Therapy and Stem Cells for COPD :Spirometry is a fundamental test that measures Forced Expiratory Volume in one second (FEV1) and Forced Vital Capacity (FVC). These metrics are critical for assessing airflow obstruction, which is a hallmark of COPD. FEV1 is particularly important as it correlates with disease severity and prognosis [1][4].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-82.png)
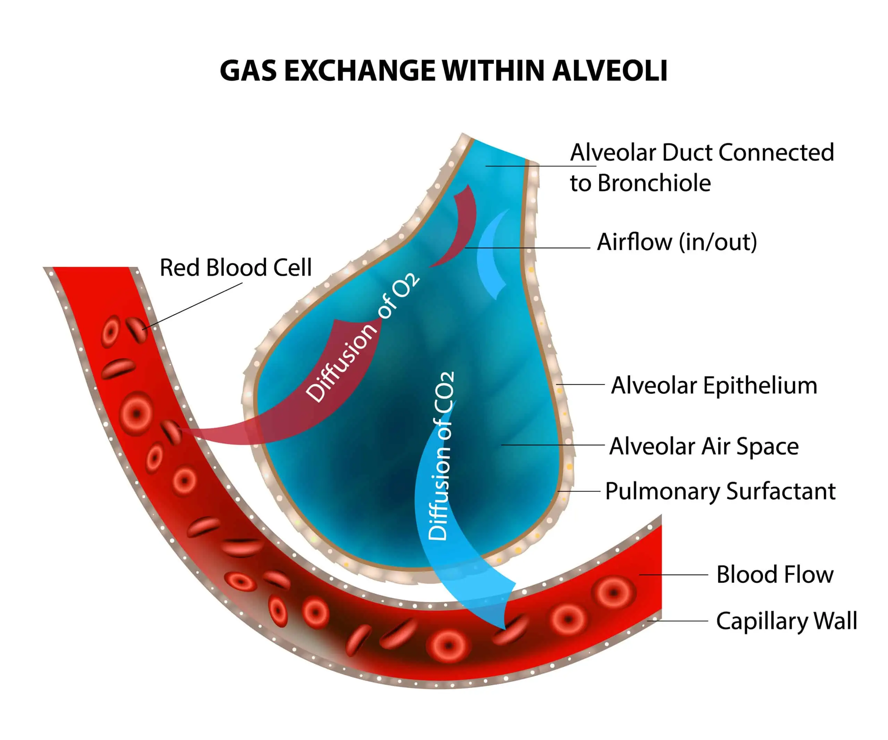
![Cellular Therapy and Stem Cells for COPD :Tools such as the Baseline Dyspnea Index (BDI), Transition Dyspnea Index (TDI), and the Medical Research Council (MRC) Dyspnea Scale are used to quantify breathlessness severity and its impact on daily activities. These scales are crucial for understanding patients' subjective experiences of their condition [2][5].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-84.png)
![Cellular Therapy and Stem Cells for COPD :The Chronic Respiratory Questionnaire (CRQ) and St. George's Respiratory Questionnaire (SGRQ) are specifically designed to evaluate health-related quality of life in respiratory diseases. They help capture the broader impact of COPD on patients' lives [2][5].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-85.png)
![Cellular Therapy and Stem Cells for COPD :This test measures the distance a patient can walk in six minutes, serving as a practical assessment of functional exercise capacity. It is widely used in clinical settings to gauge the physical limitations imposed by COPD [1][3].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-86.png)
![Cellular Therapy and Stem Cells for COPD :The SWT assesses the distance covered at increasing or constant walking paces, providing additional insights into exercise tolerance and capacity [1][3].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-87.png)
![Cellular Therapy and Stem Cells for COPD :Using treadmills or bicycles, ergometry evaluates exercise response and endurance under controlled conditions, helping to assess the functional capabilities of COPD patients [1][3].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-88.png)
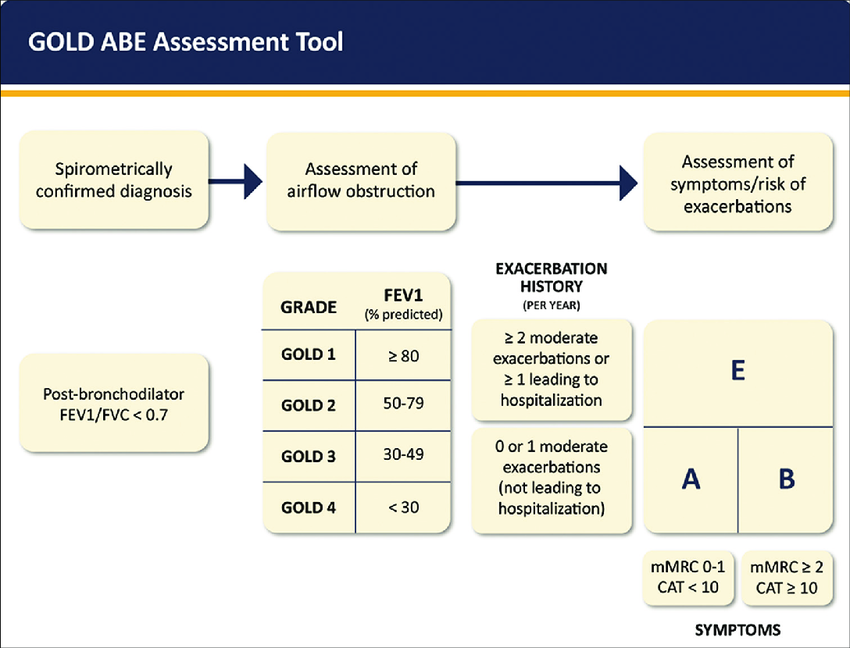
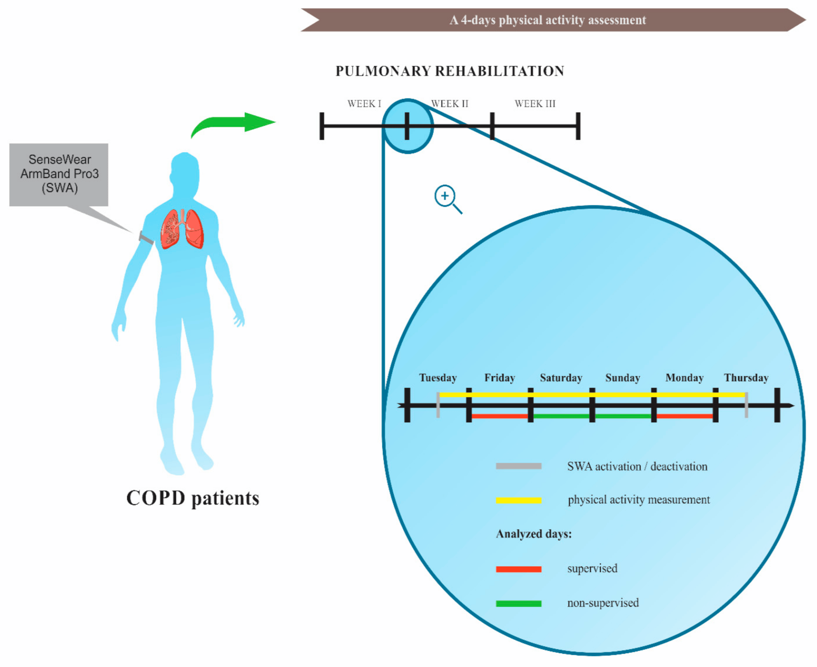
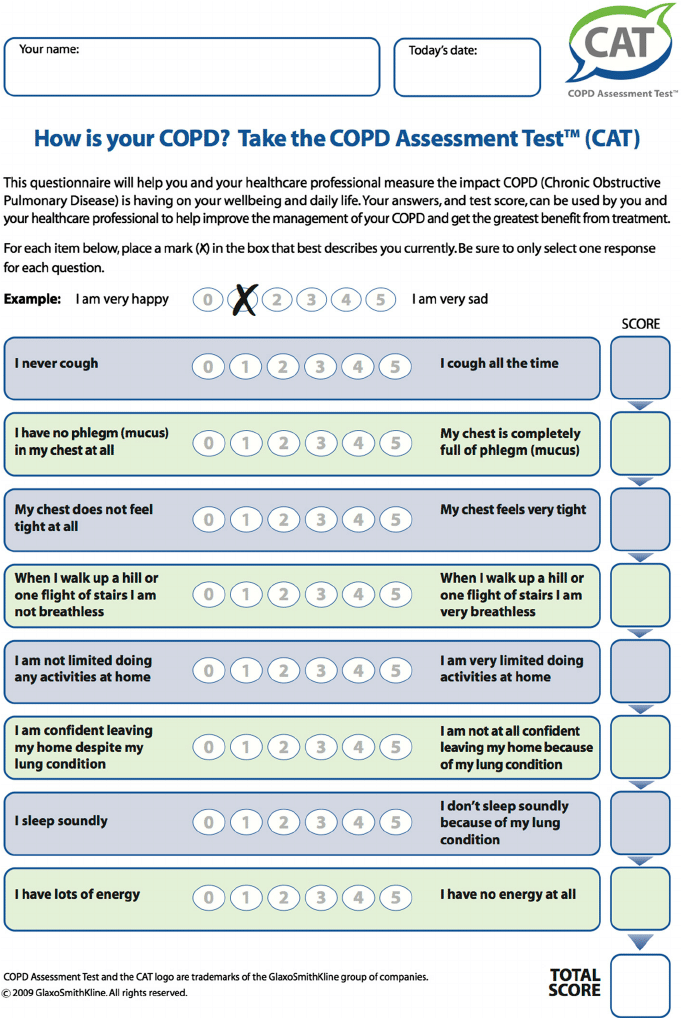
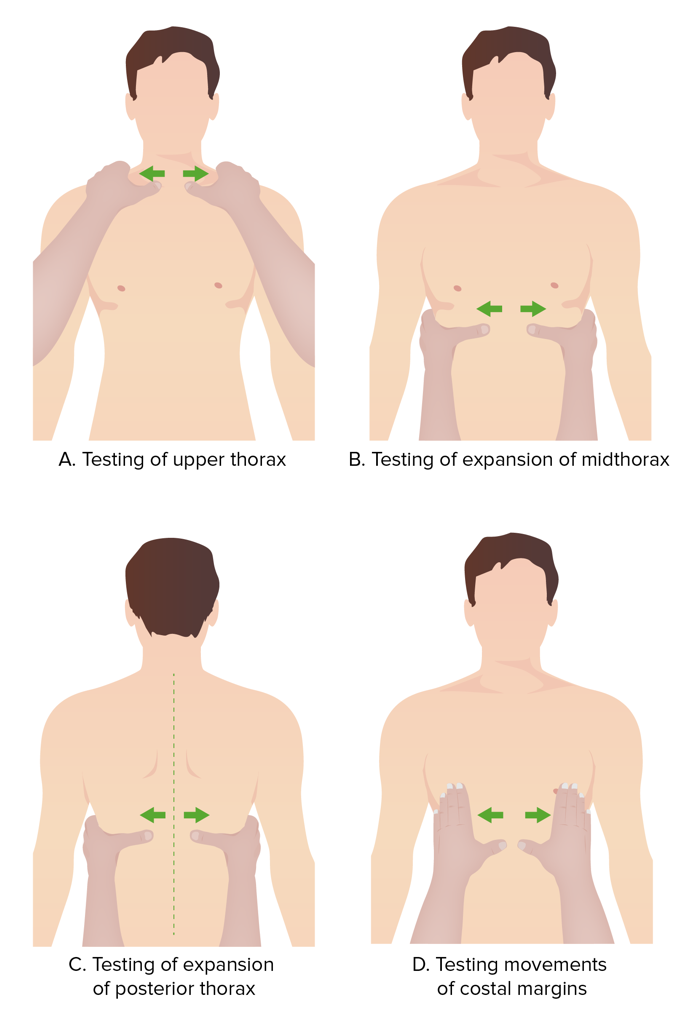
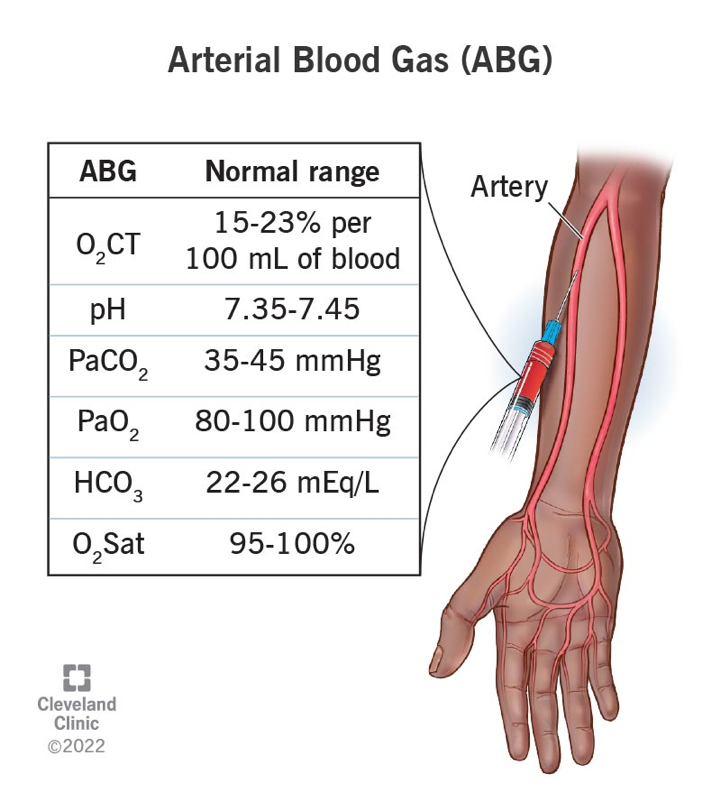
![Cellular Therapy and Stem Cells for COPD :Chronic inflammation is a hallmark of COPD. Blood tests for markers such as C-Reactive Protein (CRP) and erythrocyte sedimentation rate (ESR) can indicate inflammation levels. Effective treatment often results in decreased levels of these markers, suggesting reduced inflammation and improved disease management [5].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-94.png)
![Cellular Therapy and Stem Cells for COPD :While a CBC is not a direct measure of COPD improvement, it can reveal a reduced white blood cell (WBC) count, which may indicate better control of exacerbations, particularly if frequent infections were previously noted. This reduction can be a sign of improved overall health and management of the disease [5].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-95.jpeg)
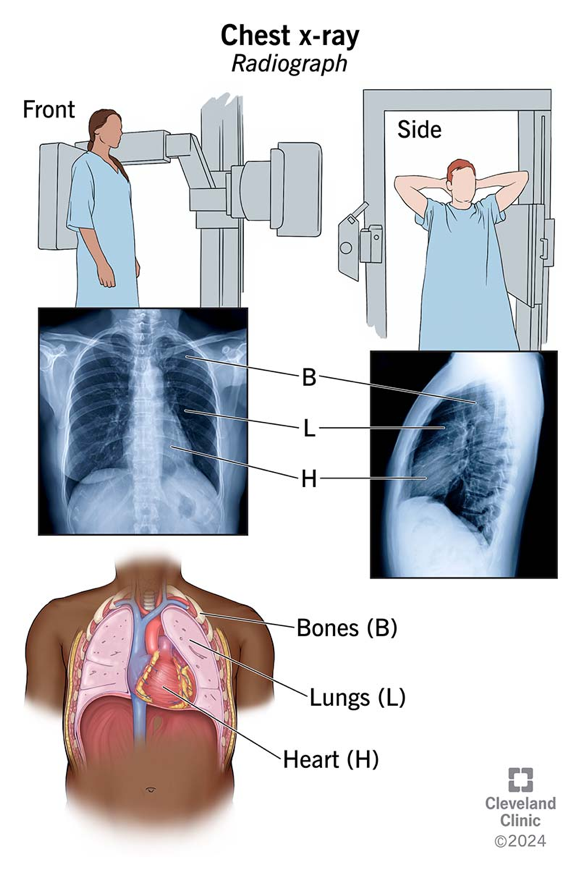
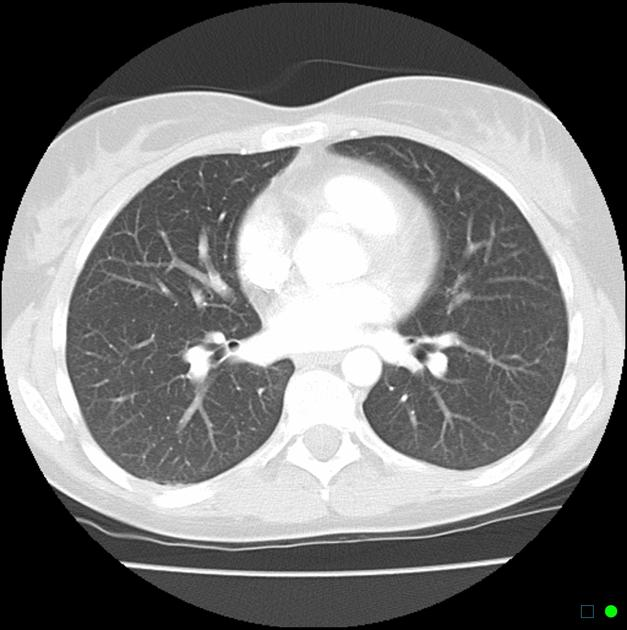
![Cellular Therapy and Stem Cells for COPD :Chronic obstructive pulmonary disease (COPD) is characterized by chronic inflammation in the lungs, primarily triggered by inhalation of harmful substances, with cigarette smoke being the most significant contributor. Below is a detailed breakdown of the key factors involved in the pathogenesis of COPD, supported by relevant citations [80-83].](https://cdn.drstemcellsthailand.com/wp-content/uploads/2024/08/word-image-6686-98.png)